
Health, United States
- 2018 -
ea t
I
nite
tates
-
2018-
Copyright information
Permission has been obtained from the copyright holders
to reproduce certain quoted material in this report. Further
reproduction of this material is prohibited without specific
permission of the copyright holder. All other material contained
in this report is in the public domain, and may be used and
reprinted without special permission; source citation, however,
is appreciated.
Suggested citation
National Center for Health Statistics.
Health, United States, 2018. Hyattsville, MD. 2019.
U.S. Department of Health and Human Services
Alex M. Azar, II
Secretary
Centers for Disease Control and Prevention
Robert R. Redfield, M.D.
Director
National Center for Health Statistics
Jennifer H. Madans, Ph.D.
Acting Director

iii
Preface
Health, United States, 2018 is the 42nd report on
the health status of the nation and is submitted by the
Secretary of the Department of Health and Human Services
to the President and the Congress of the United States in
compliance with Section 308 of the Public Health Service Act.
This report was compiled by the National Center for Health
Statistics (NCHS) of the Centers for Disease Control and
Prevention (CDC).
The Health, United States series presents an annual
overview of national trends in key health indicators. The
2018 report presents trends and current information on
selected measures of morbidity, mortality, health care
utilization and access, health risk factors, prevention, health
insurance, and personal health care expenditures in a
20-figure chartbook.
The Health, United States, 2018 Chartbook is
supplemented by several other products including Trend
Tables, an At-a-Glance table, Appendixes, and Spotlight
Infographics available for download on the Health,
United States website at: https://www.cdc.gov/nchs/hus/
index.htm.
The 2018 Edition
The Health, United States, 2018 Chartbook contains
20 figures and 20 tables on health and health care in the
United States. Examining trends in health informs the
development, implementation, and evaluation of health
policies and programs. The first section (Figures 1–12)
focuses on health status and determinants: life expectancy,
infant mortality, leading causes of death, overdose deaths,
teen births, preterm births, use of tobacco products, obesity,
asthma, diabetes prevalence, hypertension, and functional
limitations. The second section (Figures 13–15) presents
trends in health care utilization: childhood vaccination
coverage, use of prescription drugs, and unmet medical
needs. The third section (Figures 16–17) focuses on health
care resources: availability of dentists and use of long-term
care facilities. The fourth section (Figures 18–20) describes
trends in personal health care expenditures and health
insurance coverage. The Highlights section summarizes major
findings from the Chartbook.
Supplementary Materials Available
on the Web
Trend Tables
With the release of Health, United States, 2018, 47
detailed Trend Tables that highlight major trends in key
health indicators in the four areas: health status and
determinants, health care utilization, health care resources,
Health, United States, 2018
and health care expenditures will be available for download
at: https://www.cdc.gov/nchs/hus/contents2018.htm. An
important criterion used in selecting Trend Tables for the
Health, United States series is the availability of comparable
national data over a period of several years. Trend Tables are
included in the online supplement for indicators featured
in the Chartbook or on the NCHS FastStats site. FastStats
provides quick access to statistics on topics of public health
importance and is available at: https://www.cdc.gov/nchs/
fastats/default.htm.
The At-a-Glance table summarizes major findings from
the Trend Tables, and is available for download from the web
at: https://www.cdc.gov/nchs/hus/ataglance.htm.
Appendixes
Appendix I. Data Sources describes each data source
used in Health, United States, 2018 and provides references
for further information about the sources. Data sources
are listed alphabetically within two broad categories:
Government Sources and Private and Global Sources.
Appendix II. Definitions and Methods includes selected
terms used in Health, United States, 2018. It also contains
information on the statistical methodologies used in the
report.
The Appendixes for Health, United States, 2018 are
available for download at: https://www.cdc.gov/nchs/hus/
appendix.htm.
Spotlight Infographics
The Health, United States Spotlight is an infographic
series that explores topics of public health importance
using trend data from Health, United States. Spotlights are
published throughout the year and feature the most current
data available at the time of publication.
The Spotlight infographics are available for download at:
https://www.cdc.gov/nchs/hus/hus_infographic.htm.
Data Finder
The Data Finder is a useful tool on the Health,
United States website for locating data by topic. Using the
Data Finder, users may narrow down the list of tables and
charts by health topic and populations of interest. Topics
include areas such as drug overdose, prescription drug
use, and functional limitation. Populations include groups
classified by age, race and Hispanic origin, and geographic
region. See the Health, United States website at:
https://www.cdc.gov/nchs/hus/contents2018.htm.
iv Health, United States, 2018
Data Considerations
Racial and Ethnic Data
Some tables in Health, United States present data
according to race and Hispanic origin, consistent with a
department-wide emphasis on ensuring that health data
on racial and ethnic minority populations are presented
whenever possible. Trend data on race and ethnicity are
presented in the greatest detail possible after taking into
account the quality of the data, the amount of missing data,
and the number of observations. These issues significantly
affect the availability of reportable data for certain
populations, such as the Native Hawaiian or Other Pacific
Islander populations and the American Indian or Alaska
Native populations. Standards for the classification of federal
data on race and ethnicity are described in Appendix II. (See
Appendix II, Race.)
Education and Income Data
Some tables in Health, United States present data
according to socioeconomic status, using education
and family income as proxy measures. Education and
income data are generally obtained directly from survey
respondents, and are not usually available from records-
based data collection systems. (See Appendix II, Education;
Family income; Poverty.)
Statistical Significance
All statements in the text describing differences, or
lack thereof, between estimates or across time indicate
that statistical testing was performed. Differences between
two point estimates were determined to be statistically
significant at the 0.05 level using two-sided significance
tests (z-tests) without correction for multiple comparisons.
Terms such as “similar,” “no difference,” “stable,” and “no
clear trend” indicate that the statistics being compared were
not significantly different or that the slope of the trend line
was not significantly different from zero. For data sources
with no standard errors, relative differences greater than
10% are generally discussed in the text. Trends are tested
using regression analysis. The specific approaches used
to analyze trends over time depend on the data source,
type of dependent variable, and number of data points
(1). Chartbook data tables and Trend Tables include point
estimates and standard errors, when available, for users who
would like to perform additional statistical tests. Additional
information on statistical reliability and testing can be found
in the Technical Notes, which follow the Chartbook.
Accessing Health, United States
The Health, United States, 2018 Chartbook can be
accessed at: https://www.cdc.gov/nchs/hus/index.htm.
The Chartbook figures are also available for download as
PowerPoint slides. Trend Tables and Chartbook data tables
are available for download as Excel and PDF files. Excel Trend
Table files include additional years of data not shown in the
PDF files, along with standard errors, where available. Files
may be downloaded from the Health, United States website
at: https://www.cdc.gov/nchs/hus/contents2018.htm.
Visitors to the website can join the Health, United States
e-mail distribution list (https://www.cdc.gov/nchs/hus/
hus_electronic_mailing.htm) to receive announcements
about release dates and notices of updates. Previous editions
of Health, United States and its Chartbooks can also be
accessed from the website.
Printed copies of Health, United States can be purchased
from the U.S. Government Publishing Office at:
https://bookstore.gpo.gov.
Questions?
If you have questions about Health, United States or related
data products, please contact:
Office of Information Services
Information Dissemination Staff
National Center for Health Statistics
Centers for Disease Control and Prevention
3311 Toledo Road
Hyattsville, MD 20782–2064
Phone: 1–800–CDC–INFO (1–800–232–4636)
TTY: 1–888–232–6348
E-mail: healthus@cdc.gov
Online request form: https://www.cdc.gov/cdc-info/
requestform.html
For e-mail updates on NCHS publication releases, subscribe
online at: https://www.cdc.gov/nchs/email-updates.htm.

Health, United States, 2018 v
Acknowledgments
The National Center for Health Statistics’ (NCHS) Division
of Analysis and Epidemiology planned and coordinated the
content of this volume under the direction of Irma E. Arispe
and Renee M. Gindi.
Production of Health, United States, 2018 was managed
by Sheila J. Franco and Renee M. Gindi. Preparation of the
volume, including data, analysis, text for specific charts,
highlights, trend tables, and appendixes was completed by
Shilpa Bengeri, Mary Ann Bush, La-Tonya D. Curl, Barnali Das,
Sheila J. Franco, Nancy Han, Ji-Eun Kim, Florence C. Lee,
Xianfen Li, Diane M. Makuc, Zakia C. Nelson, Anita L. Powell,
and Ashley M. Woodall.
Publication assistance was provided by CDC/OSELS/
NCHS/OD/Office of Information Services, Information
Design and Publishing Staff (IDPS). Project management was
provided by Yolanda L. Jones and Danielle Taylor. Editorial
review was provided by Yolanda L. Jones and Laura Drescher.
Graphic design was provided by Simon McCann, Odell
Eldridge, and Kyung M. Park. Cover design was provided by
Liviu Tanase. Overview for IDPS publications and electronic
products was provided by Kyung M. Park and Tommy C.
Seibert, Jr. Electronic access through the NCHS website was
provided by Shilpa Bengeri, La-Tonya D. Curl, Florence C. Lee,
Diane M. Makuc, Jennifer A. Moore, and Ashley M. Woodall.
Printing was managed by Nathanael Brown (CDC/OD/OADC).
Data and technical assistance were provided by staff
of the following NCHS organizations: Division of Health Care
Statistics: Lauren Harris-Kojetin and Manisha Sengupta;
Division of Health and Nutrition Examination Surveys:
Namanjeet Ahluwalia, Lara Akinbami, Mark S. Eberhardt,
Eleanor B. Fleming, Crescent Martin, Cynthia L. Ogden,
Yechiam Ostchega, and Ryne Paulose-Ram; Division of Health
Interview Statistics: Veronica Benson, Lindsey I. Black, Debra
L. Blackwell, Peter Boersma, Amy E. Cha, Tainya C. Clarke,
Robin A. Cohen, Jacqueline B. Lucas, Tina Norris, Jeannine S.
Schiller, Emily P. Terlizzi, Maria A. Villarroel; Division of Vital
Statistics: Elizabeth Arias, Sally C. Curtin, Patrick Drake, Anne
K. Driscoll, Danielle Ely, Elizabeth C. Gregory, Joyce A. Martin,
Steven J. Steimel, Betzaida Tejada-Vera; Division of Analysis
and Epidemiology: Cheryl V. Rose and Julie Weeks.
Additional data and technical assistance were provided
by the following organizations of the Centers for Disease
Control and Prevention (CDC): National Center for Chronic
Disease Prevention and Health Promotion: Brian S. Armour,
Elizabeth A. Courtney-Long, Andrea Gentzke, and Ahmed
Jamal; National Center for HIV/AIDS, Viral Hepatitis, STD,
and TB Prevention: Lori Elmore, Jennifer Ludovic, and the
Surveillance and Data Management Branch; National Center
for Immunization and Respiratory Diseases: Laurie D. Elam-
Evans, Benjamin Fredua, Holly A. Hill, Samuel F. Posner, James
A. Singleton, Tanja Y. Walker, and David Yankey; OPHSS/
CSELS, Division of Health Informatics and Surveillance: Ruth
Ann Jajosky and Tara Strine; by the following organizations
within the Department of Health and Human Services:
Centers for Medicare & Medicaid Services: Mary Carol
Barron, Aaron C. Catlin, and Lekha S. Whittle; and Substance
Abuse and Mental Health Services Administration: Beth
Han; and by the following nongovernmental organization:
American Dental Association: Bradley Munson.
We acknowledge the contributions from local, state,
and territorial health departments and other sources in the
collection and reporting of health indicators.

vi Health, United States, 2018
Contents
Preface ............................................iii
The 2018 Edition ..................................iii
Supplementary Materials Available on the Web ........iii
Data Considerations ...............................iv
Acknowledgments ....................................v
List of Chartbook Figures .............................vii
List of Trend Tables .................................viii
Highlights .......................................... 1
Health Status and Determinants ..................... 1
Health Care Access and Utilization ................... 2
Health Care Resources ............................ 3
Health Care Expenditures and Payers ................ 3
Chartbook. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5
Health Status and Determinants ....................... 6
Life Expectancy at Birth ............................ 6
Infant Mortality .................................. 7
Selected Causes of Death .......................... 8
Drug Overdose Deaths ............................ 9
Teen Births ..................................... 10
Preterm Singleton Births .......................... 11
Use of Tobacco Products .......................... 12
Obesity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Current Asthma Among Children ................... 14
Diabetes ........................................ 15
Hypertension ................................... 16
Functional Limitation ............................ 17
Health Care Access and Utilization .................... 18
Vaccination Coverage Among Children
Aged 19–35 Months ............................ 18
Prescription Drugs ............................... 19
Unmet Need Due to Cost .......................... 20
Health Care Resources .............................. 21
Dentists ........................................ 21
Long-Term Care Services .......................... 22
Health Care Expenditures and Payers .................. 23
Personal Health Care Expenditures ................. 23
Health Insurance Coverage Among Children ......... 24
Health Insurance Coverage Among Adults
Aged 18–64 ................................... 25
Technical Notes .................................... 53
Data Sources ................................... 53
Data Presentation ................................ 53
Statistical Reliability of Estimates ................... 53
Statistical Testing ................................ 53
References ........................................ 55
Health, United States, 2018 vii
List of Chartbook Figures
Life Expectancy at Birth
Figure 1. Life expectancy at birth, by sex and race and
Hispanic origin: United States, 2007–2017
Infant Mortality
Figure 2. Infant mortality rates, by race and Hispanic origin of
mother and leading causes of death: United States, 2007–
2017
Selected Causes of Death
Figure 3. Age-adjusted death rates for selected causes of
death for all ages, by sex: United States, 2007–2017
Drug Overdose Deaths
Figure 4. Drug overdose death rates among persons aged 15
years and over, by sex and age: United States, 2007–2017
Teen Births
Figure 5. Teen births among females aged 15–19 years, by
race and Hispanic origin: United States, 2007–2017
Preterm Singleton Births
Figure 6. Preterm singleton births, by gestational age and
race and Hispanic origin of mother: United States, 2007–2017
Use of Tobacco Products
Figure 7. Cigarette smoking among adults aged 18 and over,
by age and tobacco use among adolescents in grades 9–12,
by type of product: United States, 2007–2018
Obesity
Figure 8. Obesity among children and adolescents aged 2–19
years and adults aged 20 and over, by sex: United States,
1999–2000 through 2015–2016
Current Asthma Among Children
Figure 9. Current asthma among children under age 18 years,
by race and Hispanic origin: United States, 2007–2017
Diabetes
Figure 10. Diabetes prevalence among adults aged 20 and
over, by diagnosis status and age: United States, 1999–2000
through 2015–2016
Hypertension
Figure 11. Hypertension and uncontrolled high blood
pressure among adults aged 20 and over, by sex and age:
United States, 1999–2000 through 2015–2016
Functional Limitation
Figure 12. Functional limitation among adults aged 18 and
over, by age and level of difficulty: United States, 2010–2017
Vaccination Coverage Among Children
Aged 19–35 Months
Figure 13. Vaccination coverage for combined series among
children aged 19–35 months, by selected characteristics:
United States, 2017
Prescription Drugs
Figure 14. Prescription drug use in the past 30 days, by
number of drugs taken and age: United States, 1999–2000
through 2015–2016
Unmet Need Due to Cost
Figure 15. Delay or nonreceipt of needed medical care and
nonreceipt of needed prescription drugs in the past 12
months due to cost among adults aged 18–64, by percent of
poverty level: United States, 2007–2017
Dentists
Figure 16. Number of dentists per 100,000 resident
population, by state: United States, 2017
Long-Term Care Services
Figure 17. Use of long-term care services, by type of service
and age: United States, 2011–2012 and 2015–2016
Personal Health Care Expenditures
Figure 18. Personal health care expenditures, by source of
funds and type of expenditure: United States, 2007–2017
Health Insurance Coverage Among Children
Figure 19. Health insurance coverage among children under
age 18 years, by type of coverage and race and Hispanic
origin: United States, 2007–2018 (preliminary data)
Health Insurance Coverage Among Adults
Aged 18–64
Figure 20. Health insurance coverage among adults aged
18–64, by type of coverage and race and Hispanic origin:
United States, 2007–2018 (preliminary data)
viii Health, United States, 2018
With the release of Health, United States, 2018, 47 detailed
Trend Tables are available as online-only supplements. They
are available for download at: https://www.cdc.gov/nchs/
hus/contents2018.htm.
List of Trend Tables
Table 1. Crude birth rates, fertility rates, and birth rates,
by age, race, and Hispanic origin of mother: United States,
selected years 1950–2017
Table 2. Infant, neonatal, postneonatal, fetal, and perinatal
mortality rates, by detailed race and Hispanic origin of
mother: United States, selected years 1983–2017
Table 3. Infant mortality rates, by race: United States,
selected years 1950–2017
Table 4. Life expectancy at birth, at age 65, and at age 75, by
sex, race, and Hispanic origin: United States, selected years
1900–2017
Table 5. Age-adjusted death rates for selected causes of
death, by sex, race, and Hispanic origin: United States,
selected years 1950–2017
Table 6. Leading causes of death and numbers of deaths, by
sex, race, and Hispanic origin: United States, 1980 and 2017
Table 7. Leading causes of death and numbers of deaths, by
age: United States, 1980 and 2017
Table 8. Drug overdose death rates, by drug type, sex, age,
race, and Hispanic origin: United States, selected years
1999–2017
Table 9. Death rates for suicide, by sex, race, Hispanic origin,
and age: United States, selected years 1950–2017
Table 10. Selected nationally notifiable disease rates and
number of new cases: United States, selected years 1950–
2017
Table 11. Human immunodeficiency virus (HIV) diagnoses, by
year of diagnosis and selected characteristics: United States,
2012–2017
Table 12. Health conditions among children under age 18
years, by selected characteristics: United States, average
annual, selected years 1997–1999 through 2015–2017
Table 13. Respondent-reported prevalence of heart disease,
cancer, and stroke among adults aged 18 and over, by
selected characteristics: United States, average annual,
selected years 1997–1998 through 2016–2017
Table 14. Diabetes prevalence and glycemic control among
adults aged 20 and over, by sex, age, and race and Hispanic
origin: United States, selected years 1988–1994 through
2013–2016
Table 15. Functional limitation among adults aged 18 and
over, by selected characteristics: United States, selected
years 2010–2017
Table 16. Respondent-assessed fair–poor health status,
by selected characteristics: United States, selected years
1991–2017
Table 17. Current cigarette smoking among adults aged 18
and over, by sex, race, and age: United States, selected years
1965–2017
Table 18. Age-adjusted prevalence of current cigarette
smoking among adults aged 25 and over, by sex, race, and
education level: United States, selected years 1974–2017
Table 19. Current cigarette smoking among adults aged 18
and over, by selected characteristics: United States, average
annual, selected years 1990–1992 through 2015–2017
Table 20. Use of selected substances in the past month
among persons aged 12 years and over, by age, sex, race, and
Hispanic origin: United States, selected years 2002–2017
Table 21. Selected health conditions and risk factors, by age:
United States, selected years 1988–1994 through 2015–2016
Table 22. Hypertension among adults aged 20 and over,
by selected characteristics: United States, selected years
1988–1994 through 2013–2016
Table 23. Cholesterol among adults aged 20 and over, by
selected characteristics: United States, selected years
1988–1994 through 2013–2016
Table 24. Mean macronutrient intake among adults aged
20 and over, by sex and age: United States, selected years
1988–1994 through 2013–2016
Table 25. Participation in leisure-time aerobic and muscle-
strengthening activities that meet the federal 2008 Physical
Activity Guidelines for Americans among adults aged 18 and
over, by selected characteristics: United States, selected
years 1998–2017
Table 26. Normal weight, overweight, and obesity among
adults aged 20 and over, by selected characteristics: United
States, selected years 1988–1994 through 2013–2016
Table 27. Obesity among children and adolescents aged 2–19
years, by selected characteristics: United States, selected
years 1988–1994 through 2013–2016
Table 28. Untreated dental caries, by selected characteristics:
United States, selected years 1988–1994 through 2013–2016
Table 29. Delay or nonreceipt of needed medical care,
nonreceipt of needed prescription drugs, or nonreceipt of
needed dental care during the past 12 months due to cost,
by selected characteristics: United States, selected years
1997–2017
Health, United States, 2018 ix
Table 30. Health care visits to doctor offices, emergency
departments, and home visits within the past 12 months,
by selected characteristics: United States, selected years
1997–2017
Table 31. Vaccination coverage for selected diseases among
children aged 19–35 months, by race and Hispanic origin,
poverty level, and location of residence in metropolitan
statistical area: United States, selected years 1998–2017
Table 32. Vaccination coverage for selected diseases among
adolescents aged 13–17 years, by selected characteristics:
United States, selected years 2008–2017
Table 33. Use of mammography among women aged 40 and
over, by selected characteristics: United States, selected
years 1987–2015
Table 34. Use of Pap smears among women aged 18 and
over, by selected characteristics: United States, selected
years 1987–2015
Table 35. Emergency department visits within the past
12 months among children under age 18, by selected
characteristics: United States, selected years 1997–2017
Table 36. Emergency department visits within the past
12 months among adults aged 18 and over, by selected
characteristics: United States, selected years 1997–2017
Table 37. Dental visits in the past year, by selected
characteristics: United States, selected years 1997–2017
Table 38. Prescription drug use in the past 30 days, by sex,
race and Hispanic origin, and age: United States, selected
years 1988–1994 through 2013–2016
Table 39. Persons with hospital stays in the past year, by
selected characteristics: United States, selected years
1997–2017
Table 40. Active dentists, by state: United States, selected
years 2001–2017
Table 41. Community hospital beds and average annual
percent change, by state: United States, selected years
1980–2016
Table 42. Gross domestic product, national health
expenditures, per capita amounts, percent distribution, and
average annual percent change: United States, selected years
1960–2017
Table 43. National health expenditures, average annual
percent change, and percent distribution, by type of
expenditure: United States, selected years 1960–2017
Table 44. Personal health care expenditures, by source of
funds and type of expenditure: United States, selected years
1960–2017
Table 45. Private health insurance coverage among persons
under age 65, by selected characteristics: United States,
selected years 1984–2017
Table 46. Medicaid coverage among persons under age 65,
by selected characteristics: United States, selected years
1984–2017
Table 47. No health insurance coverage among persons under
age 65, by selected characteristics: United States, selected
years 1984–2017

Health, United States, 2018 1
Highlights
This Highlights section focuses on the report subject
areas referred to in Section 308 of the Public Health
Service Act—health status and determinants, utilization of
health resources, health care resources, and health care
expenditures and payers. The Highlights section presents
trends for the recent 10-year period or examines information
for the most recent data year for topics of public health
interest. When 10 years of data are not available, the
analyses cover a time period as close as possible to 10 years
given the constraints of the data source. In the Highlights
section, estimates are for the total resident population when
based on vital or other administrative or provider records
and are for the civilian noninstitutionalized population when
based on surveys. Each highlight includes a reference to the
figure where definitions of terms and additional data can be
obtained.
Health Status and Determinants
Life Expectancy at Birth
• Life expectancy at birth in the United States for the total
population was 78.6 years in 2017, 0.5 year higher than in
2007. Despite the higher life expectancy in 2017 compared
with 2007, life expectancy at birth has decreased in
recent years. Life expectancy at birth decreased 0.2 year
between 2014 and 2015, did not change between 2015
and 2016, and then decreased another 0.1 year between
2016 and 2017 (Figure 1).
• In 2017, life expectancy at birth was 76.1 years for males
and 81.1 years for females—a difference of 5.0 years
(Figure 1).
• Life expectancy at birth was 1.4 years higher in 2017
than in 2007 for non-Hispanic black persons, while life
expectancy at birth was 0.1 year higher in 2017 than in
2007 for non-Hispanic white persons, narrowing the gap
in life expectancy between these two race and Hispanic-
origin groups. In 2007, life expectancy at birth for non-
Hispanic white persons was 4.9 years longer than for
non-Hispanic black persons; by 2017, the difference had
narrowed to 3.6 years (Figure 1).
• From 2007 to 2017, life expectancy at birth was higher
for Hispanic persons than for non-Hispanic white persons
and non-Hispanic black persons. In 2017, life expectancy
at birth for Hispanic persons was 81.8 years—3.3 years
longer than for non-Hispanic white persons and 6.9 years
longer than for non-Hispanic black persons (Figure 1).
Infant Mortality
• In 2017, the infant mortality rate was 5.79 deaths per
1,000 live births, 14% lower than in 2007 (Figure 2).
• The infant mortality rate in 2017 was 170% higher among
infants of non-Hispanic black women than among infants
of non-Hispanic Asian or Pacific Islander women (10.88
compared with 4.03 per 1,000 live births) (Figure 2).
• In 2017, the five leading causes of infant deaths were
congenital malformations, preterm births and low
birthweight, sudden infant death syndrome (SIDS),
maternal complications of pregnancy, and unintentional
injuries (accidents) (Figure 2).
Mortality
• In 2017, the age-adjusted all-cause death rate among
males was 6% lower than in 2007 (864.5 compared with
922.9 deaths per 100,000 resident population). Among
females, the age-adjusted all-cause death rate was also
6% lower in 2017 than 2007 (619.7 compared with 658.1
deaths per 100,000 resident population) (Figure 3).
• In 2017, the leading causes of death for all ages were heart
disease, cancer, unintentional injuries (accidents), chronic
lower respiratory diseases, cerebrovascular disease
(stroke), Alzheimer’s disease, and diabetes (Figure 3).
• From 2007 to 2017, the age-adjusted death rate for drug
overdose increased from 11.9 to 21.7 deaths per 100,000.
Drug overdose death rates were higher among males than
among females throughout the period for all age groups,
except for those aged 65 and over (Figure 4).
• Among males aged 15 and over, drug overdose death
rates ranged from 8.7 per 100,000 (among men aged 65
and over) to 54.3 per 100,000 (among men aged 25–34)
in 2017. Among females aged 15 and over, drug overdose
death rates ranged from 5.5 per 100,000 (among women
aged 65 and over) to 27.5 per 100,000 (among women
aged 45–54) in 2017 (Figure 4).
Natality
• From 2007 to 2017, the birth rate among teenagers aged
15–19 years fell by more than one-half, from 41.5 to 18.8
live births per 1,000 teens—a record low for the United
States (Figure 5).
• The total percentage of preterm singleton births (infants
born at less than 37 weeks of gestation) decreased
from 2007 through 2014, and then increased from 2014
2 Health, United States, 2018
through 2017. This rise in preterm births since 2014 was
largely driven by an increase in late preterm births (34–36
weeks of gestation) (Figure 6).
• In 2017, a total of 8.1% of singleton births occurred at
less than 37 weeks of gestation, including 6.0% at 34–36
weeks, 0.9% at 32–33 weeks, and 1.2% at less than 32
weeks (Figure 6).
• In 2017, the percentage of singleton births that were
born prior to 32 weeks of gestation—the group with
the greatest risk of death during infancy due to preterm
birth—was highest among non-Hispanic black women
(2.5%), and lowest among non-Hispanic white (0.9%)
and non-Hispanic Asian or Pacific Islander (0.9%) women
(Figure 6).
Use of Tobacco Products
• The percentage of students in grades 9–12 who smoked
cigarettes in the past 30 days was 7.7 percentage points
lower in 2018 than in 2011, while the use of electronic
cigarettes increased by 19.3 percentage points. In
2018, 8.1% of students had smoked cigarettes in the
past 30 days and 20.8% of students had used electronic
cigarettes (Figure 7).
• In 2017, 14.1% of adults aged 18 and over were current
cigarette smokers, a decline from 19.7% in 2007 (age
adjusted) (Figure 7).
• In 2017, current cigarette smoking prevalence was 8.0
percentage points lower than in 2007 among adults aged
18–44, 4.5 percentage points lower among adults aged
45–64, and not different among adults aged 65 and over.
In 2017, 14.6% of adults aged 18–44, 16.5% of adults
45–64, and 8.2% of adults 65 and over were current
smokers (Figure 7).
Obesity
• From 1999–2000 to 2015–2016, obesity among males
aged 2–19 increased from 14.0% to 19.1%. During the
same period, obesity among females aged 2–19 years
increased from 13.8% to 17.8% (Figure 8).
• From 1999–2000 to 2015–2016, the age-adjusted
prevalence of obesity among women increased from
33.3% to 41.2%. During the same period, the age-adjusted
prevalence of obesity among men increased from 27.4%
to 38.1% (Figure 8).
Current Asthma Among Children
• The prevalence of current asthma in children under age
18 years decreased from 9.1% in 2007 to 8.4% in 2017.
The prevalence of current asthma in non-Hispanic black
children was higher than for Hispanic and non-Hispanic
white children during the entire 2007–2017 period
(Figure 9).
Diabetes
• The age-adjusted prevalence of total diabetes among
adults aged 20 and over, which includes both physician-
diagnosed and undiagnosed diabetes, increased from
10.0% in 1999–2000 to 14.7% in 2015–2016 (Figure 10).
Hypertension
• From 1999–2000 to 2015–2016, the age-adjusted
prevalence of hypertension (systolic pressure of greater
than or equal to 140 mm Hg or diastolic pressure of
greater than or equal to 90 mm Hg or currently taking
antihypertensive medication) among adults aged 20
and over was stable and for men and women. The age-
adjusted prevalence of hypertension among men was
29.5% in 1999–2000 and 31.3% in 2015–2016, while the
prevalence among women was 30.2% in 1999–2000 and
28.7% in 2015–2016 (Figure 11).
• The age-adjusted prevalence of high blood pressure
(systolic pressure of greater than or equal to 140 mm Hg
or diastolic pressure of greater than or equal to 90 mm
Hg) among men aged 20 and over decreased from 19.6%
in 1999–2000 to 17.5% in 2015–2016. The age-adjusted
prevalence of high blood pressure among women aged 20
and over decreased from 21.1% in 1999–2000 to 13.6%
in 2015–2016. The prevalence of high blood pressure was
generally higher among men than women from 2005–
2006 to 2015–2016 (Figure 11).
Functional Limitation
• In 2017, the percentage of adults aged 18–64 who
reported having difficulty in functioning was 33.7%, with
27.8% reporting “some difficulty” and another 5.9%
reporting “a lot of difficulty” or “cannot do at all.” Among
adults aged 65 and over, the percentage of those who
reported having difficulty in functioning was 61.1%, with
41.6% reporting “some difficulty” and an additional 19.5%
reporting “a lot of difficulty” or “cannot do at all” in 2017
(data table for Figure 12). Functional limitation is defined
by the reported level of difficulty (no difficulty, some
difficulty, a lot of difficulty, or cannot do at all/unable to
do) in any of six core functioning domains: seeing, hearing,
mobility, communication, cognition, and self-care.
Health, United States, 2018 3
Health Care Access and Utilization
Vaccination Coverage Among Children
Aged 19–35 Months
• In 2017, 70.4% of children aged 19–35 months
had completed the combined 7-vaccine series of
recommended childhood vaccinations (includes
diphtheria, tetanus, pertussis, poliovirus, measles,
mumps, and rubella, among others). Children living
outside of metropolitan statistical areas (MSAs) (66.8%)
were less likely to have received the combined series than
those living in MSA principal cities (71.9%) (Figure 13).
Prescription Drugs
• The age-adjusted percentage of Americans taking five
or more prescription drugs in the past 30 days increased
from 6.5% in 1999–2000 to 10.0% in 2003–2004, and then
was stable through 2015–2016 (11.0%) (Figure 14).
• The percentage of Americans taking five or more
prescription drugs in the past 30 days increased with age.
In 2015–2016, fewer than 1% of children under age 18
years took five or more prescription drugs, compared with
3.9% of adults aged 18–44, 19.1% of adults aged 45–64,
and 39.8% of adults aged 65 and over (Figure 14).
Unmet Need Due to Cost
• In 2017, 16.2% of adults living below 100% and 15.3% of
adults living at 100%–199% of the poverty level delayed
or did not receive needed medical care due to cost
compared with 5.1% of those living at or above 400% of
the poverty level (Figure 15).
• In 2017, 11.9% of adults living below 100% and 11.6% of
adults living at 100%–199% of the poverty level did not
receive needed prescription drugs due to cost compared
with 2.7% of those at or above 400% of the poverty level
(Figure 15).
Health Care Resources
Dentists
• The supply of professionally active dentists per 100,000
total United States resident population was lowest in
Alabama (40.43), Arkansas (41.67), and Mississippi (42.86),
and highest in Alaska (79.48), Massachusetts (82.66),
and Washington, D.C. (103.89) in 2017. In general, the
southern states had the fewest dentists per population,
while the Mid-Atlantic and Pacific states had the most
(Figure 16).
Long-Term Care Services
• Home health care services were the most-used long-term
care services in 2015–2016 among adults aged 65 and
over, with 3.7 million users. The second and third most
used were hospice (1.3 million patients) and nursing home
services (1.2 million residents) (Figure 17).
Health Care Expenditures and
Payers
Personal Health Care Expenditures
• In 2017, personal health care expenditures in the United
States totaled almost $3.0 trillion—a 3.8% increase from
2016 (Figure 18).
• In 2017, expenditures for hospital care accounted for
38.6%, physician and clinical services accounted for
23.4%, and prescription drugs accounted for 11.3% of
personal health care expenditures, amounting to nearly
three-quarters of total personal health care expenditures.
The remaining expenditures included nursing care
facilities and continuing care retirement communities
(5.6%); dental (4.4%); home health care (3.3%); and
other professional services, other health residential and
personal care, durable medical equipment, and other
nondurable medical products (13.4%) (Figure 18).
• In 2017, 35.1% of the $2,961.0 billion personal health care
expenditures were paid by private health insurance,
22.3% by Medicare, 17.6% by Medicaid, 12.3% by
consumers out-of-pocket, and the remaining expenditures
were paid by other types of insurance, payers, and
programs (Figure 18).
Health Insurance Coverage Among
Children
• In 2018 (preliminary estimates), the percentage of
children under 18 years with Medicaid coverage was
36.0%, 7.4 percentage points higher than in 2007 (28.6%).
The percentage with private health insurance was 54.7%,
5.1 percentage points lower than in 2007 (59.8%), and the
percentage of children who were uninsured was 5.2%, 3.8
percentage points lower than in 2007 (9.0%) (Figure 19).
• In 2017, Hispanic children (7.7%) were more likely to be
uninsured than non-Hispanic white (4.1%), non-Hispanic
black (4.0%), and non-Hispanic Asian (3.8%) children
(Figure 19).
Health Insurance Coverage Among
Adults Aged 18–64
• In 2018 (preliminary estimates), the percentage of adults
aged 18–64 with private health insurance was 68.9%,
similar to the percentage in 2007 (69.5%). The percentage
of adults aged 18–64 with Medicaid coverage was 12.8%,
5.4 percentage points higher than in 2007 (7.4%), and the
percentage of adults aged 18–64 who were uninsured was
13.3% in 2018, 6.3 percentage points lower than in 2007
(19.6%) (Figure 20).
• In 2017, more than one-quarter of Hispanic adults (27.5%)
aged 18–64 were uninsured, which was higher than that
for non-Hispanic white (8.5%), non-Hispanic black (14.0%),
and non-Hispanic Asian (7.4%) adults (Figure 20).

Health, United States, 2018 5
Chartbook

6 Health, United States, 2018
Health Status and Determinants
Life Expectancy at Birth
Life expectancy at birth is the age to which a newborn is
expected to live given current age-specific death rates. The
measure is often presented by race, Hispanic origin, and sex,
allowing for comparisons between populations at one point
in time and within a population over time. Life expectancy
summarizes patterns in mortality across all age groups in a
given year, demonstrating the long-term impacts of age-
specific death rates (2). Changes in age-specific rates for
certain causes of death, particularly those impacting younger
age groups, can greatly impact life expectancy (3).
In the United States, life expectancy at birth was 78.6
years in 2017, 0.5 year higher than in 2007 (data table for
Figure 1). Despite the overall increase in life expectancy
in 2017 compared with 2007, life expectancy at birth has
decreased since 2015 (4). Increases in mortality from the
leading causes of death, specifically unintentional injuries,
suicide, and Alzheimer’s disease, have contributed to the
recent decreases in life expectancy (5).
Life expectancy at birth for males decreased 0.2 year
from 76.5 in 2014 to 76.3 years in 2015, another 0.1 year
from 2015 to 2016 to 76.2 years, and another 0.1 year from
2016 to 2017 to 76.1 years. Life expectancy at birth for
females decreased 0.2 year from 81.3 in 2014 to 81.1 years
in 2015, and remained at 81.1 years from 2015 to 2017. From
2007 to 2017, life expectancy for females was higher than
males, continuing a long-term pattern (3). In 2017, the life
expectancy at birth for females was 5.0 years higher than
that for males.
From 2007 to 2017, life expectancy was higher for
Hispanic persons than for non-Hispanic white and non-
Hispanic black persons. In 2017, the difference between the
group with the highest (Hispanic) and lowest (non-Hispanic
black) life expectancy at birth was 6.9 years, compared with
a 7.2-year difference between these groups in 2007. From
2007 to 2017, life expectancy at birth increased 1.4 years for
non-Hispanic black persons, 1.1 years for Hispanic persons,
and 0.1 year for non-Hispanic white persons. Despite higher
life expectancy in 2017 compared with 2007, life expectancy
at birth has declined for persons in all three race and
Hispanic-origin groups since 2014.
0
60
80
100
Hispanic
Black, not Hispanic
White, not Hispanic
20172007
Life expectancy (years)
0 20 40 60 80 100
Female
Male
Total
2014
2015
2016
2017
Life expectancy (years)
Life expectancy at birth, by sex:
2014, 2015, 2016, and 2017
78.9
78.7
78.7
78.6
76.5
76.3
76.2
76.1
81.3
81.1
81.1
81.1
Figure 1. Life expectancy at birth, by sex and race and Hispanic origin: United States, 2007–2017
NOTES: Some states reported multiple-race data. The multiple-race data for these states were bridged to the four single-race categories for comparability across the trend. Life
expectancy estimates for 2017 use preliminary Medicare data. For more information, see Appendix II, Life expectancy. See data table for Figure 1.
SOURCE: NCHS, National Vital Statistics System (NVSS), Mortality. Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_001

Health, United States, 2018 7
Health Status and Determinants
Infant Mortality
Infant mortality, the death of a baby before his or
her first birthday, is a public health measure that reflects
the health status of the whole population, including living
conditions, illness rates, access to health care, and maternal
health (6). Although the infant mortality rate has decreased
dramatically over the past seven decades, disparities in infant
mortality by race and Hispanic origin, socioeconomic status,
and geography remain (3,7).
From 2007 to 2011, the infant mortality rate decreased
by an average of 2.9% per year, then decreased by an
average of 0.6% per year to 5.79 infant deaths per 1,000 live
births in 2017. Among infants of non-Hispanic black women,
the mortality rate decreased by an average of 4.1% per year
from 2007 to 2011, and then was stable through 2017. From
2007 to 2014, mortality rates decreased by an average of
2.5% per year among infants of non-Hispanic Asian or Pacific
Islander women and then was stable through 2017. The
mortality rate among infants of non-Hispanic white women
decreased by an average of 2.9% per year from 2007 to 2010
and then decreased by an average of 1.2% per year to 4.69
infant deaths per 1,000 live births in 2017. The mortality rate
decreased by an average of 1.8% per year among infants
of Hispanic women from 2007 to 2013 and then was stable
through 2017 (5.10 infant deaths per 1,000 live births).
Mortality rates among infants of non-Hispanic American
Indian or Alaska Native women decreased by an average of
2.3% per year from 2007 to 2014 and then showed no
clear trend from 2014 to 2017.
From 2007 to 2017, infants of non-Hispanic black and
non-Hispanic American Indian or Alaska Native women
consistently had the highest rate of mortality, whereas
infants of non-Hispanic Asian or Pacific Islander women
consistently had the lowest mortality rate. In 2017, the
infant mortality rates for non-Hispanic black women (10.88
per 1,000 live births) and non-Hispanic American Indian or
Alaska Native women (8.90 per 1,000 live births) were more
than twice the rate for non-Hispanic Asian or Pacific Islander
women (4.03 per 1,000 live births).
In 2017, 55.7% of infant deaths were attributable to
the following leading causes: congenital malformations,
preterm births and low birth weight, sudden infant death
syndrome (SIDS), maternal complications of pregnancy, and
unintentional injuries (accidents) (5). From 2007 to 2017, the
mortality rate from congenital malformations decreased for
most of the period from 134.9 to 119.2 infant deaths per
100,000 live births. The rates for preterm births and low
birthweight (97.5 in 2017), SIDS (35.3 in 2017), and maternal
complications of pregnancy (37.2 in 2017) decreased for the
period. The rate of unintentional injuries showed no clear
trend from 2007 to 2017. However, the mortality rate from
unintentional injuries was the only leading cause of infant
mortality higher in 2017 (34.1) than in 2007 (29.7 infant
deaths per 100,000 live births).
0
2
4
6
8
10
12
14
American Indian or Alaska
Nave, not Hispanic
Congenital Preterm birth SIDS Maternal Unintenonal
malformaons and low complicaons injuries
birthweight of pregnancy (accidents)
14
140
Race and Hispanic origin Leading causes of death: 2007 and 2017
12
120
Black, not Hispanic
2007 2017
e births
10
100
ths per 1,000 liv
8
80
Total
134.9
6
60
119.2
Hispanic
112.7
t dea
97.5
White, not Hispanic
anf
4
40
In
Asian or Pacific Islander, not Hispanic
57.0
2
20
41.1
35.3
37.2
29.7
34.1
0
0
2007 2017
Figure 2. Infant mortality rates, by race and Hispanic origin of mother and leading causes of death: United States, 2007–2017
NOTES: Congenital malformations is congenital malformations, deformations, and chromosomal abnormalities. SIDS is sudden infant death syndrome. Some states reported multiple-
race data. The multiple-race data for these states were bridged to the four single-race categories for comparability across the trend. See data table for Figure 2.
SOURCE: NCHS, National Vital Statistics System (NVSS), Linked Birth/Infant Death Data Set. Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_002
134.9
119.2
112.7
97.5
57.0
35.3
41.1
37.2
29.7
34.1

8 Health, United States, 2018
Health Status and Determinants
Selected Causes of Death
Death rates are an important summary measure of
population health. Death rates are often age-adjusted to
remove the effects of changing age distributions over time or
across groups (8). In 2017, a total of 2,813,503 deaths were
registered in the United States (5). The age-adjusted all-
cause death rate was 731.9 deaths per 100,000 population
in 2017, down from 775.3 in 2007. In 2017, the age-adjusted
death rates were higher among males than females for all the
selected causes of death except Alzheimer’s disease, where
rates were lower among males than females.
From 2007 to 2017, heart disease and cancer continued
to be the top two leading causes of death for both males and
females. For both males and females, the age-adjusted death
rate for heart disease and cancer decreased throughout the
period, though the rate of decrease slowed for heart disease
from 2011 to 2017. In 2017, the age-adjusted death rate per
100,000 population for heart disease was 209.0 among males
and 129.6 among females. In 2017, the age-adjusted death
rate per 100,000 population for cancer was 181.1 among
males and 131.4 among females.
The age-adjusted death rate for unintentional injuries—
which includes unintentional drug overdoses (9)—was stable
for both males and females from 2007 to 2013, and then
increased from 2013 to 2017 by an average of 7.2% per year
for males (from 53.1 to 67.8 deaths per 100,000) and 5.0%
per year for females (from 26.6 to 32.0 deaths per 100,000).
From 2007 to 2017, the age-adjusted death rate for
chronic lower respiratory disease decreased by an average
of 1.3% per year for males (from 48.8 to 45.0 deaths per
100,000), while it remained stable throughout the period for
females (38.1 deaths per 100,000 in 2017). The age-adjusted
death rate for stroke decreased from 2007 to the early 2010s
by an average of 3.3% per year for males and 3.0% per year
for females, and then was stable through 2017. In 2017, the
age-adjusted death rate per 100,000 population for stroke
was 38.0 among males and 36.6 among females. The age-
adjusted death rate for Alzheimer’s disease was stable from
2007 to 2013 for both males and females, and then increased
from 2013 to 2017 by an average of 6.4% per year for males
(from 19.3 to 24.9 deaths per 100,000) and 7.8% per year for
females (from 25.9 to 34.8 deaths per 100,000).
From 2007 to 2017, the age-adjusted death rate for
diabetes decreased among females by an average of 4.7%
per year (from 19.8 to 17.1 deaths per 100,000), though
the decline slowed from 2009 to 2017. There was no clear
trend in the age-adjusted death rate for diabetes among
males from 2007 to 2009, and then the rate increased by an
average of 0.7% per year from 2009 to 2017 (from 25.0 to
26.8 deaths per 100,000).
ale) �on (log scDeaths per 100,000 popula
Uninten�onal injuries
Uninten�onal injuries
Figure 3. Age-adjusted death rates for selected causes of death for all ages, by sex: United States, 2007–2017
NOTES: CLRD is chronic lower respiratory disease. Unintentional injuries is another term for accidents. Stroke is another term for cerebrovascular disease. See data table for Figure 3.
SOURCE: NCHS, National Vital Statistics System (NVSS), Mortality. Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_003
10,000
Male
Female
All causes
1,000
All causes
Heart disease
Heart disease
Cancer
Cancer
100
CLRD
Stroke
Alzheimer’s disease
CLRD
Diabetes
Stroke
Alzheimer’s disease
Diabetes
10
2007 2017
2007 2017

9
Health Status and Determinants
Drug Overdose Deaths
Rates of drug overdose deaths have increased
nationwide since the 1990s, with more rapid increases
observed in recent years (9,10). While some drug overdose
deaths are classified as suicides (7%) or homicides (less than
1%), the majority (87%) were unintentional in 2017 (9).
In 2017, there were 70,237 deaths from drug
overdoses—up from 36,010 deaths in 2007 (9). The age-
adjusted drug overdose death rate in 2017 was nearly twice
as high as the death rate in 2007 (21.7 compared with 11.9
deaths per 100,000). The death rate increased by an average
of 3.2% per year from 2007 to 2014, and then accelerated to
an average of 15.5% per year from 2014 to 2017. Increases
in the rate of drug overdose deaths involving opioids—
particularly heroin and fentanyl, a synthetic opioid—have
contributed to the overall acceleration in the drug overdose
trend (9,11,12).
Among males, the age-adjusted drug overdose death
rate was almost twice as high in 2017 than in 2007 (29.1
compared with 14.9 deaths per 100,000). For the age groups
shown, drug overdose death rates increased more rapidly in
recent years after a period of either stability or increase. The
recent increases were especially pronounced among men
Health, United States, 2018
aged 25–34 and 35–44. From 2013 to 2017, the drug
overdose death rate increased by an average of 18.5% per
year among men aged 25–34 and by an average of 18.8% per
year among men aged 35–44. In 2017, drug overdose death
rates ranged from 8.7 per 100,000 among men aged 65 and
over to 54.3 per 100,000 among men aged 25–34. Drug
overdose death rates were higher among males than
females; however, similarly rapid increases were observed
for the younger age groups among women in recent years.
Increases were especially pronounced among females
aged 15–24 years and women aged 25–34. From 2014 to
2017, the drug overdose death rate increased by an average
of 17.5% per year among females aged 15–24 years and by an
average of 16.4% per year among women aged 25–34.
Among women aged 55–64 and women aged 65 years and
over, the drug overdose death rate increased from 2007
to 2017, by an average of 7.1% per year and 3.6% per year,
respectively. The age-adjusted drug overdose death rate for
females was 64% higher in 2017 than in 2007 (14.4 compared
with 8.8 deaths per 100,000). In 2017, drug overdose death
rates ranged from 5.5 per 100,000 among women aged 65
and over to 27.5 per 100,000 among women aged 45–54.
60
Male Female
50
�onDeaths per 100,000 popula
40
45–54
30
35–44
45–54
25–34
20
35–44
55–64
15–24
55–64
25–34
10
65 and over
15–24
65 and over
0
2007 2017 2007 2017
Figure 4. Drug overdose death rates among persons aged 15 years and over, by sex and age: United States, 2007–2017
NOTES: Drug overdose deaths are identified using International Classification of Diseases, 10th revision (ICD–10) underlying cause of death codes X40–X44 (unintentional drug
poisoning), X60–X64 (suicide by drug poisoning), X85 (homicide by drug poisoning), and Y10–Y14 (drug poisoning of undetermined intent). See data table for Figure 4.
SOURCE: NCHS, National Vital Statistics System (NVSS), Mortality. Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_004
On December 23, 2019, the text describing Figure 4 was corrected
to state that the drug overdose death rates are for all males and all
females, not for males and females aged 15 and over as had been
stated. The chart and data table for Figure 4 have not changed.

10 Health, United States, 2018
Health Status and Determinants
Teen Births
Teen births—births to women under age 20—carry
negative social and health consequences for the mother and
baby (13). Infants born to teen mothers are at higher risk
of low birth weight and preterm birth, which in turn, puts
them at risk of infant morbidity and infant mortality (14).
Additionally, babies born to teen mothers are more likely to
become teen mothers themselves (13,15).
In 2017, a total of 194,377 babies were born to teens
aged 15–19 years, for a birth rate of 18.8 per 1,000 teens,
down from 41.5 live births per 1,000 teens in 2007. Birth
rates decreased by an average of 4.9% per year from 2007
to 2009, and then decreased more rapidly by an average of
8.4% per year from 2009 to 2017. For non-Hispanic Asian or
Pacific Islander teens, the birth rate decreased by an average
of 8.9% per year from 2007 to 2013, and then decreased
more rapidly by an average of 12.0% per year from 2013 to
4.6 live births per 1,000 teens in 2017. Birth rates among
non-Hispanic white and non-Hispanic black teens aged
15–19 were stable from 2007 to 2009. From 2009 to 2017,
rates decreased by an average of 7.8% per year to 13.4 live
births per 1,000 for non-Hispanic white teens, while rates
decreased by an average of 9.0% per year to 27.6 live births
for non-Hispanic black teens. For Hispanic teens, the birth
rate decreased by an average of 9.3% per year from 2007 to
2017, from 75.3 to 28.9 per 1,000 teens. For non-Hispanic
American Indian or Alaska Native teens, the birth rate
decreased by an average of 7.3% per year from 2007 to 2017,
from 66.3 to 32.2 per 1,000 teens.
Throughout that period, non-Hispanic American Indian
or Alaska Native, non-Hispanic black, and Hispanic teens had
higher birth rates compared with non-Hispanic white and
non-Hispanic Asian or Pacific Islander teens. Non-Hispanic
Asian or Pacific Islander adolescents had lower birth rates
than all other race and Hispanic-origin groups from 2007 to
2017.
100
seared 15–19 y
80
Hispanic
emales ag
60
Black, not Hispanic
American Indian or Alaska
, not Hispanic
Live births per 1,000 f
Total
40
White, not Hispanic
20
Asian or Pacific Islander, not Hispanic
0
2007 2017
EĂƟǀĞ
Figure 5. Teen births among females aged 15–19 years, by race and Hispanic origin: United States, 2007–2017
NOTES: Some states reported multiple-race data. The multiple-race data for these states were bridged to the four single-race categories for comparability across the trend. See data
table for Figure 5.
SOURCE: NCHS, National Vital Statistics System (NVSS), Natality. Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_005

Health, United States, 2018 11
Health Status and Determinants
Preterm Singleton Births
Gestational age is an important predictor of an infant’s
survival and subsequent health (16–20). Preterm births,
defined as births delivered at less than 37 completed
weeks of gestation, is a leading cause of infant death in the
United States (Figure 2). As gestational age of the infant
increases, the risk of death decreases. Infants delivered at
less than 32 completed weeks of gestation (early preterm
births) are at the greatest risk of death during infancy,
compared with infants born with longer gestational ages (21).
Preterm births are more likely to occur in twin or higher-
order pregnancies, with early preterm birth occurring in
20% of twins, 68% of triplets, 92% of quadruplets, and 100%
of quintuplets and higher-order births, compared with 2%
of singleton (one fetus) births (22). To remove the effect
of multiple births on the likelihood of preterm birth, the
analysis is limited to singleton births.
The total percentage of singleton births that were
preterm decreased by an average of 1.4% per year, from
8.6% in 2007 to 7.8% in 2014, and then increased by an
average of 1.8% per year, from 2014 to 2017, reaching 8.1% in
2017. The increase in preterm births from 2014 to 2017 was
largely driven by an increase in late preterm births (those
occurring at 34–36 weeks of gestation), particularly births
that occurred at 36 weeks of gestation (23). The percentage
of births that were late preterm decreased by an average of
2.0% per year, from 6.4% in 2007 to 5.7% in 2013, and then
increased by an average of 1.4% per year, from 2013 to 2017,
reaching 6.0% in 2017. In 2017, a total of 8.1% of singleton
births occurred at less than 37 weeks of gestation: 6.0% at
34–36 weeks, 0.9% at 32–33 weeks, and 1.2% at less than 32
weeks.
In 2017, among each of the three gestational age groups,
a higher percentage of singleton births that were preterm
were to non-Hispanic black and non-Hispanic American
Indian or Alaska Native women than to non-Hispanic white,
non-Hispanic Asian or Pacific Islander, and Hispanic women.
The highest percentage of singleton births that were early
preterm (2.5%) were to non-Hispanic black women, while
the lowest percentage of singleton births that were early
preterm were to non-Hispanic white (0.9%) and non-Hispanic
Asian or Pacific Islander women (0.9%).
15
34–36 weeks
32–33 week
term
s
e
Less than 32 weeks
11.6
e prer
10.4
t w
Tot ek
e singleton births tha
10
al (less than 37 we s)
8.3
7.7
7.2
7.1
34–36 weeks
7.8
6.2
5
t of liv
5.5
5.5
1.3
cener
Less than 32 weeks
1.1
P
32–33 weeks
0.9
2.5
0.8
0.7
1.5
1.2
0.9
0.9
0
Black, not American Hispanic or Asian or White, not
2007 2017
Hispanic Indian or Pacific Islander, Hispanic
Alaska not Hispanic
not Hispanic
6.2
0.9
1.2
5.5
0.8
0.9
5.5
0.7
0.9
7.7
1.3
2.5
7.8
1.1
1.5
Figure 6. Preterm singleton births, by gestational age and race and Hispanic origin of mother: United States, 2007–2017
NOTES: Preterm singleton births are based on the obstetric estimate of gestational age and are for all singleton births. Singleton births refer to single births, in contrast with multiple
or higher order births. “Late preterm” births are defined as singleton births at 34–36 weeks of gestation; “moderate preterm” births are defined as singleton births occurring at
32–33 weeks of gestation; and “early preterm” births are defined as singleton births occurring at less than 32 weeks. Estimates may not sum to total percentage due to rounding.
Some states reported multiple-race data. The multiple-race data for these states were bridged to the four single-race categories for comparability across the trend. See data table for
Figure 6.
SOURCE: NCHS, National Vital Statistics Survey, Natality. Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_006
>ĂƟŶĂ
EĂƟǀĞ͕

12 Health, United States, 2018
Health Status and Determinants
Use of Tobacco Products
Cigarette smoking causes a number of diseases,
including coronary heart disease, stroke, chronic obstructive
pulmonary disease, and at least 12 types of cancer (24).
Cigarette smoking remains the leading preventable cause of
premature disease and death in the United States, with more
than 480,000 deaths each year attributed to smoking and
secondhand smoke exposure (24).
Overall, age-adjusted cigarette smoking prevalence
among adults aged 18 and over decreased by an average
of 0.8 percentage points per year from 2007 to 2017, from
19.7% to 14.1%. Among adults aged 18–44, current cigarette
smoking was stable from 2007 to 2009 and then decreased
an average of 1.0 percentage point per year from 2009 to
2017, from 23.4% to 14.6%. Among adults aged 45–64,
current cigarette smoking decreased from 2007 to 2017 by
an average of 0.6 percentage points per year, from 21.0%
to 16.5%. Among adults aged 65 and over, no clear trend
was observed in current cigarette smoking throughout the
period. From 2007 to 2017, prevalence of cigarette smoking
was lower among adults aged 65 and over than among
adults aged 18–44 and 45–64. In 2017, 16.5% of adults aged
45–64 were current cigarette smokers, twice as high as the
percentage of those aged 65 and over.
Among adolescents, the use of tobacco products
can cause lasting harm to the developing brain and lead
to sustained tobacco use in adulthood (24). Electronic
cigarettes, or e-cigarettes, are battery-powered tobacco
products that typically deliver nicotine in the form of an
aerosol. They were introduced in the United States in 2007,
and their use by adolescents has increased rapidly (25).
E-cigarette use is associated with an increased likelihood
of the use of other tobacco products, especially cigarettes,
cigars, and hookahs (25).
30
Current cigaree smoking among Tobacco use in the past 30 days
adults aged 18 and over among adolescents in grades 9–12
25
Any
18–44
24.2
tobacco
27.1
products
20
Electronic
1.5
Total
45–64
20.8
tcen
15.8
er
15
8.1
2011
P
2018
11.6
Cigars
7.6
10
Smokeless
7.9
65 and over
tobacco
5.9
5
4.1
Hookah
4.1
0
2007
2017
0 5 10 15 20 25 30
Percent
Figure 7. Cigarette smoking among adults aged 18 and over, by age and tobacco use among adolescents in grades 9–12, by
type of product: United States, 2007–2018
NOTES: Current cigarette smoking by adults is defined as smoking either every day or some days. Use of tobacco products by high school students in grades 9–12 is defined as having
used the product on one or more days during the past 30 days. Data on pipe tobacco can be found in the data table. See data table for Figure 7.
SOURCES: NCHS, National Health Interview Survey (NHIS) (panel 1); and CDC, National Youth Tobacco Survey (NYTS) (panel 2).
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_007
Among students in grades 9–12, the use of any tobacco
products in the past 30 days did not differ significantly from
2011 to 2018 (26). The use of e-cigarettes among students in
grades 9–12 increased from 1.5% in 2011 to 20.8% in 2018,
becoming the most commonly used tobacco product among
students in grades 9–12 in 2014 (26).
ĐŝŐĂƌĞƩĞƐ
ŝŐĂƌĞ Ʃ ĞƐ

Health, United States, 2018 13
Health Status and Determinants
Obesity
In children and adolescents, excess body weight is
associated with excess morbidity during childhood, as well
as obesity in adulthood (27,28). Children and adolescents
with obesity are at higher risk of having other chronic health
conditions, such as asthma, sleep apnea, joint problems, and
type 2 diabetes (29–31).
Adult obesity is also correlated with excess morbidity.
Obesity in adulthood is associated with hypertension,
high cholesterol levels, type 2 diabetes, and other health
conditions (32–34). In addition, obesity, particularly higher
levels of obesity (body mass index [BMI] greater than or
equal to 35.0), are associated with increased mortality (35).
From 1999–2000 to 2015–2016, obesity among males
aged 2–19 increased from 14.0% to 19.1%. During the same
period, obesity among females aged 2–19 years increased
from 13.8% to 17.8%. In 2015–2016, 18.5% of children and
adolescents in the United States aged 2–19 had obesity (36);
no difference was observed between the prevalence of
obesity for males and females aged 2–19 years.
From 1999–2000 to 2015–2016, the age-adjusted
prevalence of obesity among women increased from
33.3% to 41.2%. During the same period, the age-adjusted
prevalence of obesity among men increased from 27.4% to
38.1%. In 2015–2016, there was no statistical difference in
the age-adjusted prevalence of obesity for men and women
aged 20 and over.
Figure 8. Obesity among children and adolescents aged 2–19 years and adults aged 20 and over, by sex: United States,
1999–2000 through 2015–2016
NOTES: Obesity in youth is defined as body mass index (BMI) at or above the sex- and age-specific 95th percentile of the 2000 CDC Growth Charts. Adult obesity estimates are age
adjusted. Obesity in adults is defined as BMI greater than or equal to 30.0. Estimates are based on measured height and weight. See data table for Figure 8.
SOURCE: NCHS, National Health and Nutrition Examination Survey (NHANES). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_008
50 50
Children and adolescents aged 2–19 years Adults aged 20 and over
40 40
Women
ed)
30
t
30
cent
e adjus
Men
erP
t (ag
20
cen
20
Males
erP
Females
10 10
0 0
1999– 2015– 1999– 2015–
2000 2016 2000 2016

14 Health, United States, 2018
Health Status and Determinants
Current Asthma Among Children
Asthma is a chronic lung disease that inflames and
narrows the airways, causing recurring periods of wheezing,
chest tightness, shortness of breath, and coughing (37).
Children with asthma are at increased risk of emergency
department visits and hospitalizations (38,39). Death from
asthma attacks may also occur, although rarely (39). Those
with continued uncontrolled symptoms are at risk of activity
limitation, decreased quality of life, and developing chronic
obstructive pulmonary disease as adults (40).
From 2007 to 2017, current asthma prevalence among all
children under age 18 years decreased by an average of 0.1
percentage points per year, from 9.1% to 8.4%. From 2007 to
2017, the prevalence of current asthma in non-Hispanic white
and Hispanic children showed no clear trend. During the
same period, current asthma prevalence decreased among
non-Hispanic black children by an average of 0.3 percentage
points per year, from 15.4% to 12.6%. Non-Hispanic black
children had higher prevalence of current asthma compared
with Hispanic and non-Hispanic white children from 2007
to 2017. The prevalence of current asthma was 12.6% in
non-Hispanic black children and 7.7% in Hispanic and non-
Hispanic white children in 2017.
Figure 9. Current asthma among children under age 18 years, by race and Hispanic origin: United States, 2007–2017
NOTES: Current asthma is based on parent or knowledgeable adult responding yes to both questions, “Has a doctor or other health professional ever told you that your child had
asthma?” and “Does your child still have asthma?” See data table for Figure 9.
SOURCE: NCHS, National Health Interview Survey (NHIS). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_009
20
15
Black, not Hispanic
cent
10
erP
Total
Hispanic
White, not Hispanic
5
0
2007 2017

Health, United States, 2018 15
Health Status and Determinants
Diabetes
Diabetes is a chronic disease that affects the body’s
ability to produce and use insulin, a hormone that helps
maintain blood sugar levels (41). Individuals with diabetes
may have high blood sugar levels, which can lead to long-
term complications including heart disease, vision loss, and
kidney disease (42). In 2017, diabetes was the seventh leading
cause of death in the United States (5).
Among those with diabetes, some have not received
a diagnosis from a doctor or health care professional
(undiagnosed diabetes). Having undiagnosed diabetes
may delay diabetes management and treatment that are
necessary to avoid long-term complications.
The age-adjusted prevalence of total diabetes
(diagnosed and undiagnosed) among adults aged 20 and over
increased from 10.0% in 1999–2000 to 14.7% in 2015–2016.
The increase in total diabetes among adults from 1999–2000
to 2015–2016 was driven by an increase in physician-
diagnosed diabetes during the same period. Among adults
aged 20 and over, the age-adjusted prevalence of physician-
diagnosed diabetes rose from 6.2% in 1999–2000 to 10.0% in
2015–2016, while no clear trend was observed for the age-
adjusted prevalence of undiagnosed diabetes throughout this
period (4.7% in 2015–2016).
Older adults are more likely than younger adults to have
diabetes. In 2015–2016, 28.2% of adults aged 65 and over,
21.9% of adults aged 45–64, and 5.6% of adults aged 20–44
had total diabetes. The difference in total diabetes by age
was greater in 2015–2016 than in 1999–2000. In 1999–2000,
the prevalence of total diabetes among adults aged 65 and
over was 13.6 percentage points higher than the prevalence
among adults aged 20–44; in 2015–2016, this difference was
22.6 percentage points. In 1999–2000, the prevalence of
total diabetes among adults aged 45–64 was 10.4 percentage
points higher than the prevalence among adults aged
20–44; in 2015–2016, this difference was 16.3 percentage
points. Increases in total diabetes among adults aged 45–64
and adults aged 65 and over in this period were driven by
increases in physician-diagnosed diabetes; the prevalence of
undiagnosed diabetes for both older age groups remained
similar. Among adults aged 20–44, the prevalence of both
physician-diagnosed diabetes and undiagnosed diabetes
remained similar in 1999–2000 and 2015–2016.
Figure 10. Diabetes prevalence among adults aged 20 and over, by diagnosis status and age: United States, 1999–2000
through 2015–2016
* Estimate is considered unreliable based on the new multistep NCHS data presentation standards for proportions. The absolute confidence interval width of the estimate is
0.05–0.30 and the relative confidence interval width is greater than 130%. The estimate has undergone statistical review. For more information see: Parker JD, Talih M, Malec DJ, et
al. National Center for Health Statistics Data Presentation Standards for Proportions. NCHS. Vital Health Stat 2(175). 2017.
NOTES: Undiagnosed diabetes is fasting plasma glucose of at least 126 mg/dL or a hemoglobin A1c of at least 6.5% and no reported physician diagnosis. The forward adjustment
method was incorporated into the fasting plasma glucose values from 1999–2000 to 2013–2014 to ensure comparability with 2015–2016 data. For more information, see Appendix II,
Diabetes. Estimates may not sum to total percentage due to rounding. See data table for Figure 10.
SOURCE: NCHS, National Health and Nutrition Examination Survey (NHANES). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_010
25
Diabetes prevalence by diagnosis status, Diabetes prevalence by age,
1999–2000 through 2015–2016
Age (years)
1999–2000 and 2015–2016
20–44
1.6 2.7
20
Undiagnosed
Physician
1999–2000
4.3
diagnosed
2015–2016
e adjusted)
5.6
15
2.4
45–64
Total
t (ag
1999–2000 14.7
cen
10
er
Physician diagnosed
2015–2016
21.9
P
65 and
over
5
1999–2000
17.9
Undiagnosed
2015–2016
28.2
0
1999–
2015–
0 10 20 30 40 50 60
2000
2016
Percent
6.3
7.0
*5.4
7.1
8.3
14.9
12.5
21.1
3.2

16 Health, United States, 2018
Health Status and Determinants
Hypertension
Hypertension is a risk factor for cardiovascular
disease, stroke, kidney disease, and other health conditions
(43,44). Hypertension and cigarette smoking are the
leading preventable causes of cardiovascular deaths in
the United States (45,46). A meta-analysis of randomized
controlled trials of treatment of high blood pressure
found that stroke, heart disease, heart failure, deaths
from cardiovascular disease, and all-cause mortality are
decreased by lowering high blood pressure to normal levels
(47). Conversely, those with uncontrolled hypertension
have been shown to have increased all-cause mortality,
as well as mortality related to heart, cardiovascular, and
cerebrovascular disease (48).
Hypertension was defined as having measured high
blood pressure (systolic pressure of greater than or equal to
140 mm Hg or diastolic pressure of greater than or equal to
90 mm Hg) or currently taking antihypertensive medication.
From 1999–2000 to 2015–2016, the age-adjusted prevalence
of hypertension among men and women aged 20 and over
showed no clear trend. In 2015–2016, the age-adjusted
prevalence of hypertension among men was 31.3% and
among women was 28.7%. The age-adjusted percentage of
high blood pressure among men aged 20 and over decreased
from 19.6% to 17.5% from 1999–2000 to 2015–2016. The
age-adjusted percentage of high blood pressure among
women aged 20 and over decreased from 21.1% to 12.3%
from 1999–2000 to 2009–2010, and then showed no clear
trend through 2015–2016 (13.6%). From 1999–2000 to
2003–2004, the age-adjusted percentage of men and women
with high blood pressure was not different, while from
2005–2006 to 2015–2016, high blood pressure was generally
higher among men than women.
In 2015–2016, the likelihood of uncontrolled high
blood pressure (high blood pressure among those with
hypertension) differed by sex and age group. Among
men with hypertension, 73.1% of those aged 20–44 had
uncontrolled high blood pressure, compared with 50.1% of
those aged 45–64 and 51.7% of those aged 65 and over. In
contrast, uncontrolled high blood pressure was more likely
among women with hypertension aged 65 and over (55.8%)
compared with women aged 20–44 (37.9%) and aged 45–64
(42.1%). While the percentage of uncontrolled high blood
pressure was similar for men and women with hypertension
aged 45–64 and 65 and over, men aged 20–44 with
hypertension were more likely to have uncontrolled high
blood pressure (73.1%) than women aged 20–44 (37.9%).
Figure 11. Hypertension and uncontrolled high blood pressure among adults aged 20 and over, by sex and age: United States,
1999–2000 through 2015–2016
NOTES: High blood pressure was defined as having measured high blood pressure, regardless of medication use. Hypertension was defined as having measured high blood pressure
(systolic pressure of greater than or equal to 140 mm Hg or diastolic pressure of greater than or equal to 90 mm Hg) or currently taking antihypertensive medication. Uncontrolled
high blood pressure is high blood pressure among those with hypertension. Overall estimates are age adjusted; age-specific estimates are crude. See data table for Figure 11.
SOURCE: NCHS, National Health and Nutrition Examination Survey (NHANES). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_011
50
100
Uncontrolled high blood pressure among those with
hypertension, by sex and age (years): 2015–2016
40
80
73.1
20–44 45–64 65 and over
Hypertension–Men
ed)e adjust
30
60
55.8
Hypertension–Women
51.7
cent
50.1
t (ag
erP
42.1
cen
20
40
37.9
er
High blood pressure–Men
P
High blood pressure–Women
10
20
0
0
Men Women
1999– 2015–
2000 2016

Health, United States, 2018 17
Health Status and Determinants
Functional Limitation
Limitations in functioning may be a result of physical
or mental impairments and can result in lower levels of
educational attainment, employment, and participation in
other daily activities (49). Functional limitation is defined
by the reported level of difficulty (no difficulty, some
difficulty, a lot of difficulty, or cannot do at all/unable to do)
in six core functioning domains: seeing, hearing, mobility,
communication, cognition, and self-care. Adults who
reported having “some difficulty” or “a lot of difficulty or
cannot do at all” to at least one domain were classified as
having difficulty in functioning.
The age-adjusted percentage of adults aged 18–64 who
reported having “a lot of difficulty or cannot do at all” in at
least one of the functional domains increased by an average
of 0.3 percentage points per year from 2010 to 2014, and
then decreased by an average of 0.3 percentage points per
year from 2014 to 2017. From 2010 to 2017, the age-adjusted
percentage of adults aged 18–64 who reported having
“some difficulty” in at least one domain, but not reporting “a
lot of difficulty or cannot do at all” in any domain increased
by an average of 0.3 percentage points per year. From 2010
to 2017, adults aged 18–64 were less likely to report having
any level of difficulty than adults aged 65 and over. In 2017,
the percentage of adults aged 18–64 who reported having
difficulty was 33.7%, with 27.8% reporting “some difficulty”
and another 5.9% reporting “a lot of difficulty or cannot do
at all.”
From 2010 to 2017, the age-adjusted percentage of
adults aged 65 and over who reported “some difficulty” or
“a lot of difficulty or cannot do at all” showed no clear trend.
In 2017, the percentage of adults aged 65 and over who
reported having difficulty was 61.1%, with 41.6% reporting
“some difficulty” and an additional 19.5% reporting “a lot of
difficulty or cannot do at all.”
18–64 65 and over
100
No difficulty
80
tribu�on
No difficulty
60
t dis
Some difficulty
cen
40
erP
20
Some difficulty
A lot of difficulty or cannot do at all
A lot of difficulty or cannot do at all
0
2010 2017 2010 2017
Figure 12. Functional limitation among adults aged 18 and over, by age and level of difficulty: United States, 2010–2017
NOTES: Functional limitation is defined by the reported level of difficulty in six domains of functioning: seeing (even if wearing glasses), hearing (even if wearing hearing aids),
mobility (walking or climbing stairs), communication (understanding or being understood by others), cognition (remembering or concentrating), and self-care (such as washing all
over or dressing). Adults who respond “a lot of difficulty” or “cannot do at all/unable to do” to at least one domain are classified in the “a lot of difficulty or cannot do at all” category.
Of those remaining, adults who respond “some difficulty” to at least one domain were classified in the “some difficulty” category and adults who respond “no difficulty” to all the
questions are classified in the “no difficulty” category. Estimates are age adjusted and may not sum to total percentage due to rounding. See data table for Figure 12.
SOURCE: NCHS, National Health Interview Survey (NHIS). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_012
Some difficulty
A lot of difficulty or cannot do at all

18 Health, United States, 2018
Health Care Access and Utilization
Vaccination Coverage Among Children Aged 19–35 Months
During the 20th century, the introduction of several
vaccines led to substantial achievements in the control of
infectious diseases (50). Childhood immunization prevents an
estimated 40,000 deaths and 20 million cases of disease in
each birth cohort (51).
Vaccination coverage is defined as the estimated
percentage of people who have received specific
vaccines. For children aged 19–35 months, a series of
vaccinations is recommended by the Advisory Committee
on Immunization Practices (52). A summary indicator
called the “combined 7-vaccine series (4:3:1:3*:3:1:4)”
indicates whether children met the recommendations for
7 vaccinations: 4 or more doses of either the diphtheria,
tetanus toxoids, and pertussis vaccine (DTP), the diphtheria
and tetanus toxoids vaccine (DT), and the diphtheria,
tetanus toxoids, and acellular pertussis vaccine (DTaP); 3 or
more doses of any poliovirus vaccine; 1 or more doses of a
measles-containing vaccine (MCV); 3 or more doses or 4 or
more doses of Haemophilus influenzae type b vaccine (Hib)
depending on Hib vaccine product type (full series Hib); 3
or more doses of hepatitis B vaccine; 1 or more doses of
varicella vaccine; and 4 or more doses of pneumococcal
conjugate vaccine.
In 2017, 70.4% of children aged 19–35 months had
received the combined 7-vaccine series, up from 56.6% in
2010 (data table for Figure 13). Non-Hispanic black children
were less likely to have received the combined 7-vaccine
series (66.5%) than non-Hispanic white children (71.5%).
Vaccination coverage for children in other race and Hispanic-
origin groups did not differ significantly from vaccination
coverage for non-Hispanic white children. Children aged
19–35 months living in nonmetropolitan statistical area
(MSA) (66.8%) were less likely to have received the combined
7-vaccine series compared with those living in MSA principal
cities (71.9%).
Vaccination coverage varied by insurance status.
Children aged 19–35 months who were uninsured (48.5%)
were less likely to have received the combined 7-vaccine
series than children who were covered by private health
insurance (76.0%) or Medicaid (66.5%). For children aged
19–35 months who were insured, combined 7-vaccine
series coverage was higher among those with private health
insurance (76.0%) than those with Medicaid (66.5%).
Total
70.4
Race and Hispanic origin
White, not Hispanic
71.5
Black, not Hispanic
66.5
Asian, not Hispanic
72.4
American Indian or Alaska
65.9
not Hispanic
Hispanic
70.4
MSA status
MSA principal city
71.9
MSA nonprincipal city
69.8
Non-MSA
66.8
Health insurance status
Private
76.0
Medicaid
66.5
Uninsured
48.5
0 20 40 60 80 100
Percent
Figure 13. Vaccination coverage for combined series among children aged 19–35 months, by selected characteristics:
United States, 2017
NOTES: MSA is metropolitan statistical area. See Appendix II, Vaccination. See data table for Figure 13.
SOURCE: National Center for Immunization and Respiratory Diseases (NCIRD), National Immunization Survey-Child (NIS-Child).
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_013
EĂƟǀĞ͕

Health, United States, 2018 19
Health Care Access and Utilization
Prescription Drugs
For millions of Americans, prescription drugs have
saved lives, controlled disease, and prevented or delayed
the onset of chronic disease and disability (53–57). The
increasing use of prescription drugs is driven by several
factors: an aging population with chronic conditions, the
development of new and innovative prescription drugs, and
changes in prescription drug coverage (e.g., the Medicare
Part D program) (58,59). The increased use of prescription
drugs has raised concerns about misuse. For example,
antibiotics are still prescribed to treat viral infections,
even though they are ineffective for this purpose (60,61),
and there is concern about adverse events resulting from
inappropriate prescribing to adults aged 65 and over (62,63).
Although opioid drugs may be a component of effective pain
management, emergency department visits for adverse drug
events are increasing among adults aged 50 and over (9,64)
(Figure 4).
The age-adjusted percentage of Americans taking 5
or more prescription drugs in the past 30 days increased
from 6.5% in 1999–2000 to 10.0% in 2003–2004, and then
was stable through 2015–2016 (11.0%). The age-adjusted
percentage of Americans who took 1–4 prescription drugs
in the past 30 days decreased from 37.5% in 1999–2000
to 34.4% in 2015–2016. The age-adjusted percentage of
Americans who took no prescription drugs in the past
30 days decreased from 56.0% in 1999–2000 to 52.1% in
2007–2008, and then increased to 54.7% in 2015–2016.
In 2015–2016, increasing age was associated with
prescription drug use. Nearly 80% of children under age 18
years compared with 12.5% of adults aged 65 and over had
not taken prescription drugs in the past 30 days. Among
children, 20.3% took 1–4 prescription drugs in the past
month. Among adults, the percentage taking 5 or more drugs
in the past 30 days increased with age from 3.9% of those
aged 18–44, 19.1% of those aged 45–64, to 39.8% of those
aged 65 and over.
Figure 14. Prescription drug use in the past 30 days, by number of drugs taken and age: United States, 1999–2000 through
2015–2016
NOTES: Respondent-reported use of prescription drugs in the past 30 days. See Appendix II, Drug. See data table for Figure 14.
SOURCE: NCHS, National Health and Nutrition Examination Survey (NHANES). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_014
2015–2016
100 100
3.9
5 or more drugs
0.7
20.3
19.1
5 or more
80 80
31.4
39.8
drugs
1–4 drugs
ed)e adjust
60 60
cent
48.3
t (ag
erP
cen
40 40
79.0
er
47.7
1–4 drugs
P
64.7
No drugs
20 20
32.6
12.5
No drugs
0 0
Under 18 18–44 45–64 65 and over
1999–2000 2015–2016

20 Health, United States, 2018
Health Care Access and Utilization
Unmet Need Due to Cost
Failure to obtain needed health care may lead to delays
in diagnosis or treatment and poorer health outcomes (65).
Underuse of medications is associated with poorer health,
increased cardiovascular events, and increased use of health
care services (66,67).
From 2007 to 2017, adults aged 18–64 with lower
incomes were more likely to delay or not receive needed
medical care due to cost than those with higher incomes.
Among those living below the poverty level, the percentage
with unmet medical need due to cost was 16.2% in 2017,
4.6 percentage points lower than in 2007. The percentage
increased from 2007 to 2011, and then decreased through
2017. For those living at 100%–199% of the poverty level,
15.3% had unmet medical need in 2017, 4.6 percentage
points lower than in 2007. The percentage increased from
2007 to 2010, and then decreased through 2017. Among
adults living at 200%–399% of the poverty level, 11.6%
had unmet medical need in 2017, 1.4 percentage points
lower than in 2007. The percentage increased from 2007
to 2009, decreased from 2009 to 2015, and then increased
again through 2017. Among adults at or above 400% of the
poverty level, 5.1% had unmet medical need in 2017, similar
to the percentage in 2007. During the period, the percentage
increased from 2007 to 2009, decreased from 2009 to 2014,
and increased through 2017.
From 2007 to 2017, adults aged 18–64 with lower
incomes were more likely to not receive needed prescription
drugs due to cost than those with higher incomes. Among
those living below the poverty level, the percentage who
had unmet prescription drug need was 11.9% in 2017, 6.9
percentage points lower than in 2007. The percentage
increased from 2007 to 2010, and then decreased through
2017. For adults living at 100%–199% of the poverty level,
the percentage who did not receive needed prescription
drugs was 11.6% in 2017, 5.6 percentage points lower than
in 2007. The percentage decreased from 2007 to 2017. For
adults living at 200%–399% of the poverty level, 7.0% had
unmet prescription need in 2017, 3.6 percentage points
lower than in 2007. The percentage increased from 2007 to
2009, decreased from 2009 to 2014, and then was stable
through 2017. Among adults at or above 400% of the poverty
level, 2.7% had unmet prescription need in 2017, similar
to the percentage in 2007, although some decreases were
observed from 2007 to 2017.
30
Delay or nonreceipt of needed medical care Nonreceipt of needed drugs
Below 100%
Below 100%
20
t
100%–199%
100%–199%
cenerP
200%–399%
10
200%–399%
At or above 400%
At or above 400%
0
2007 2017
2007 2017
Figure 15. Delay or nonreceipt of needed medical care and nonreceipt of needed prescription drugs in the past 12 months
due to cost among adults aged 18–64, by percent of poverty level: United States, 2007–2017
NOTE: See data table for Figure 15.
SOURCE: NCHS, National Health Interview Survey (NHIS). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_015
ƉƌĞƐĐƌŝƉƟŽŶ

Health, United States, 2018 21
Health Care Resources
Dentists
The health of the teeth, mouth, and surrounding skull
and facial structures are essential to a person’s overall health
and well-being (68). Professional dental treatment and
preventive services are key to preventing tooth decay, gum
disease, and other oral diseases (68–71).
Despite having 198,517 professionally active dentists
in the United States in 2017 (72), the Health Resources and
Services Administration (HRSA) notes that as of June 30,
2019, over 53 million Americans live in areas designated as
having a shortage of dental health professionals (73). Having
a sufficient number and adequate distribution of dental care
providers is critical to ensuring the population has access to
needed dental care. Even when the overall supply of dentists
is adequate for the population size, the distribution may
be inadequate relative to the need among disadvantaged
populations or in certain geographic areas (74). For example,
persons with low income or those living a greater distance
from the dentist are less likely to receive dental care (75,76),
possibly because of the supply and accessibility of dentists.
The number of professionally active dentists per
100,000 resident population in the United States was 58.47
in 2007 and 60.95 in 2017, an increase of 4.2% (72). By state,
the supply of dentists per 100,000 resident population was
lowest in Alabama (40.43), Arkansas (41.67), and Mississippi
(42.86), and highest in Alaska (79.48), Massachusetts (82.66),
and Washington, D.C. (103.89) in 2017. In general, the
southern states had the fewest professionally active dentists
per population, while the Mid-Atlantic and Pacific states had
the most.
OR
CA
AZ
AK
HI
NM
TX
LA
MS
AL
GA
OH
FL
AR
MO
TN
KY
NE
OK
KS
NV
UT
CO
WA
ID
MT
ND
WY
SD
WI
MI
ME
NH
MA
CT
RI
NJ
DE
VT
NY
PA
WV
VA
MD
NC
SC
IN
IL
MN
IA
DC
40.43–51.54
51.55–64.16
64.17–82.66
82.67–103.89
U.S. Total: 60.95
Rate
Figure 16. Number of dentists per 100,000 resident population, by state: United States, 2017
NOTES: Data for the map are displayed by a modified Jenks classification for the 50 U.S. states and D.C., which creates categories that minimize within-group variation and maximize
between-group variation. Data include professionally active dentists only. Data on the number of dentists per 100,000 civilian population are calculated using 2010-based postcensal
estimates. See data table for Figure 16.
SOURCE: American Dental Association, Health Policy Institute. Supply of Dentists in the US: 2001–2017. (Copyright 2017 American Dental Association. Reprinted with permission. All
rights reserved.) Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_016

22 Health, United States, 2018
Health Care Resources
Long-Term Care Services
Long-term care services fill a crucial role by delivering
needed health care, personal care, housing, and supportive
services to those with chronic conditions and disabilities—
particularly to older adults with age-related conditions
(77,78). These services are provided in several different
settings, including the home and other residential care
settings, the community, and institutions. Providers of
long-term care services include adult day services centers;
home health agencies; residential care communities such as
assisted living settings; in-home or in-facility hospice care
organizations; and nursing homes (77–80).
Among adults aged 65 and over, home health care
services were the most-used long-term care services in
2015–2016, with 3.7 million users, a decrease from 3.9
million users in 2011–2012. Hospice services were the next
most commonly used by this age group, with 1.3 million
hospice patients, 15% more users than in 2011–2012. In
2015–2016, there were 1.2 million nursing home residents,
4% higher than in 2011–2012. The number of residential care
community residents increased 14% from 2011–2012 to 0.8
million residents in 2015–2016. The number of participants
in adult day services among adults aged 65 and over was
almost 0.2 million in both 2011–2012 and 2015–2016.
The majority of long-term care services users in 2015–
2016 were aged 65 and over. This includes 94.5% of hospice
patients, 93.4% of residential care residents, 83.5% of nursing
home residents, 81.9% of home health patients, and 62.6%
of participants in adult day services centers. About one-half
of the residential care community (52.1%) and hospice users
(47.8%) were aged 85 and over. The proportion of users aged
85 and over in the other sectors varied: 38.6% of nursing
home residents, 25.2% of home health patients, and 16.3%
of participants in adult day services centers.
Adults aged 65 and over, by type of service
Nursing
2011–2012
homes
1.2
56.7
2015–2016
40
44.9
0.7
46.7
0.8
41.3
Under
20
37.4
age 65
Adult day
0.2
services
centers
0.2
18.1
16.5
5.5
6.6
0
Home Hospices Nursing Adult day
0 1 2 3 4 5
health homes care services
Number of users (millions)
agencies centers
Adults aged 65 and over, by type of service Use of long-term care service, by age (years): 2015–2016
100
Home
85 and
3.9
16.3
health
over
agencies
3.7
25.2
80
38.6
47.8
52.1
1.2
Hospices
1.3
1.1
60
46.3
56.7
18.1
65–84
46.7
5.5
25.2
47.8
16.3
38.6
52.1
46.3
44.9
41.3
37.4
16.5
6.6
Figure 17. Use of long-term care services, by type of service and age: United States, 2011–2012 and 2015–2016
NOTES: Number of users were rounded to the nearest 100. Percentages were based on the unrounded numbers and may not sum to 100 because of rounding. People may use more
than one service per year, and were counted in each service used. See data table for Figure 17.
SOURCE: NCHS, National Study of Long-Term Care Providers (NSLTCP). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_017
ZĞƐŝĚĞŶƟĂů
ĐŽŵŵƵŶŝƟĞƐ
ƚƌŝďƵƟŽŶƚĚŝƐĐĞŶĞƌW
ZĞƐŝĚĞŶƟĂů
care
ĐŽŵŵƵŶŝƟĞƐ

Health, United States, 2018 23
Health Care Expenditures and Payers
Personal Health Care Expenditures
Health care spending accounted for almost 18% of the
United States economy in 2017 (81,82). National health
expenditures measure annual spending for health care in the
United States, presented by type of good or service, sources
of funding, and type of sponsor. Expenditures for personal
health care (PHC) include goods and services relating directly
to patient care, such as hospital care, physicians’ services,
dentists’ services, drugs, eyeglasses, and nursing home care.
In 2017, PHC expenditures comprised 85% of national health
care expenditures (81).
From 2007 to 2017, total PHC expenditures grew from
$1.92 trillion to $2.96 trillion, an average annual growth of
4.4% (83). The average annual growth in PHC expenditures
was 6.5% for Medicaid (federal), 4.9% for Medicare, 4.4% for
Medicaid (state and local), 4.5% for private health insurance,
and 2.3% for out-of-pocket spending (data table for
Figure 18). In 2017, private health insurance ($1.0 trillion) was
the largest source of PHC spending, followed by Medicare
($660.0 billion), total Medicaid ($521.3 billion) and out-of-
pocket spending ($365.5 billion).
In 2017, spending for hospital care was the largest
proportion of PHC spending (38.6%), followed by physician
and clinical services (23.4%), prescription drugs (11.3%),
nursing care facilities and continuing care retirement
communities (5.6%), dental care (4.4%), and home health
care (3.3%). All other types of expenditures, such as other
health residential and personal care, durable medical
equipment, and other nondurable medical products,
accounted for the remaining 13.4% of PHC spending. From
2007 to 2017, the proportion of PHC spending decreased
for prescription drugs, nursing care facilities and continuing
care retirement communities, dental care, and physician
and clinical services, while increasing for hospitals and home
health care.
Source of funds Type of expenditure
1,200
100
13.2 13.4
Other
3.0
3.3
Home health care
1,000
80
5.1
4.4
Dental
6.5 5.6
Nursing care facili�es and
con�nuing care re�rement
Dollar amount in billions
11.3
communi�es
800
600
40
400
Percent distribu�on
12.3
Private
Prescrip�on drugs
60
23.4
Physician and clinical
23.8
Medicare
Medicaid (total)
Out of pocket
Hospital
Medicaid (federal)
20
200
36.1
38.6
Medicaid (state)
0 0
2007 2017
2007 2017
(Total: $1,918 (Total: $2,961
billion) billion)
Figure 18. Personal health care expenditures, by source of funds and type of expenditure: United States, 2007–2017
NOTES: Personal health care expenditures are outlays for goods and services relating directly to patient care. Personal health care expenditures are in current dollars and are not
adjusted for inflation. See data table for Figure 18.
SOURCE: Centers for Medicare & Medicaid Services, National Health Expenditure Accounts (NHEA).
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_018

24 Health, United States, 2018
Health Care Expenditures and Payers
Health Insurance Coverage Among Children
Children and adolescents need regular and ongoing
health care to provide routine preventive care, such as
age-appropriate vaccinations and screenings for health
conditions, injury care, health and developmental guidance,
and treatment for acute and chronic conditions (84).
Historically, children have been more likely than adults
(Figure 20) to have health insurance coverage primarily
because they have been more likely to qualify for Medicaid
(85) or be covered by the Children’s Health Insurance
Program (CHIP) (86). Children with health insurance are more
likely to have access to health care, a usual source of care,
and a recent health care visit than those who are uninsured
(87).
The percentage of children under age 18 years who were
uninsured decreased by an average of 0.5 percentage points
per year from 2007 to 2015, and then was stable through
2017 (5.0%). In 2018, 5.2% of children were uninsured.
Medicaid coverage of children, which includes other state-
sponsored health programs and CHIP, increased by an
average of 2.3 percentage points per year from 2007 to the
early 2010s, and then was stable through 2017 (36.7%). In
2018, 36.0% of children were covered by Medicaid (88).
The percentage of children with private health insurance
coverage decreased by an average of 1.7 percentage points
per year from 2007 to the early 2010s, and then increased
by an average of 0.3 percentage points per year to 55.2% in
2017. In 2018, 54.7% of children had private coverage.
In 2017, Hispanic children (7.7%) were more likely
to lack health insurance than non-Hispanic white (4.1%),
non-Hispanic black (4.0%), and non-Hispanic Asian (3.8%)
children. In 2017, non-Hispanic white (69.0%) and non-
Hispanic Asian (70.8%) children were approximately twice as
likely to have private health insurance compared with non-
Hispanic black (36.3%) and Hispanic (34.8%) children. Non-
Hispanic black (56.1%) and Hispanic (55.1%) children were
twice as likely to have Medicaid coverage as non-Hispanic
white (23.8%) and non-Hispanic Asian (23.6%) children.
Figure 19. Health insurance coverage among children under age 18 years, by type of coverage and race and Hispanic origin:
United States, 2007–2018 (preliminary data)
NOTES: Estimates for 2018 are preliminary and are shown with a dashed line (88). Health insurance categories are mutually exclusive. A small percentage of children are covered by
Medicare, military plans, or other plans. Estimates for this group are not presented. See data table for Figure 19.
SOURCE: NCHS, National Health Interview Survey (NHIS). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_019
2017
100
White Black Asian Hispanic
only, not only, not only, not
Hispanic Hispanic Hispanic
80
70.8
69.0
60
56.1
t
55.1
Private
cenerP
40
36.3
34.8
Medicaid
23.8
23.6
20
Uninsured
7.7
4.1
4.0
3.8
0
Uninsured Medicaid Private
2007 2018

Health, United States, 2018 25
Health Care Expenditures and Payers
Health Insurance Coverage Among Adults Aged 18–64
Health insurance aids access to the health care system.
Research suggests that many health outcomes are better
for those with health insurance, especially among those
with chronic illnesses such as congestive heart disease and
hypertension (89,90). Adults who are uninsured are more
likely to delay or not receive needed medical care due to cost
than those with health insurance (91).
The percentage of adults aged 18–64 who were
uninsured increased by an average of almost 0.5 percentage
points per year from 2007 to the early 2010s, then decreased
by an average of 3.0 percentage points per year to 2015,
and then showed no clear trend through 2017 (12.8%). In
2018, 13.3% of adults were uninsured (88). The percentage
of adults aged 18–64 with private health insurance coverage
decreased by an average of 1.3 percentage points per year
from 2007 to the early 2010s, and then increased by an
average of 1.1 percentage points per year to 69.6% in 2017.
In 2018, 68.9% of adults had private coverage (88). Medicaid
coverage increased an average of 0.6 percentage points per
year from 2007 to 13.2% in 2017. In 2018, 12.8% of adults
were covered by Medicaid.
In 2017, 27.5% of Hispanic adults aged 18–64 were
uninsured, a higher percentage than for non-Hispanic Asian
(7.4%), non-Hispanic white (8.5%), and non-Hispanic black
(14.0%) adults aged 18–64. Non-Hispanic white (77.5%)
and non-Hispanic Asian adults (77.6%) in this age group
were more likely to have private health insurance coverage,
compared with 50.5% of Hispanic adults and 57.5% of non-
Hispanic black adults. In 2017, non-Hispanic white (9.4%) and
non-Hispanic Asian (12.2%) adults were less likely to have
Medicaid coverage than non-Hispanic black (22.3%) and
Hispanic adults (18.9%).
Figure 20. Health insurance coverage among adults aged 18–64, by type of coverage and race and Hispanic origin:
United States, 2007–2018 (preliminary data)
NOTES: Estimates for 2018 are preliminary and are shown with a dashed line (88). Health insurance categories are mutually exclusive. A small percentage of persons are covered by
Medicare, military plans, or other plans. Estimates for this group are not presented. See data table for Figure 20.
SOURCE: NCHS, National Health Interview Survey (NHIS). Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_20
2017
100
White Black Asian Hispanic
only, not only, not only, not
Hispanic Hispanic Hispanic
80
77.5
77.6
Private
60
57.5
cent
50.5
erP
40
27.5
Uninsured
22.3
18.9
20
14.0
12.2
Medicaid
8.5
9.4
7.4
0
Uninsured Medicaid Private
2007 2018

26 Health, United States, 2018
Chartbook Data Tables
Data table for Figure 1. Life expectancy at birth, by sex and race and Hispanic origin: United States, 2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_001
Life expectancy at birth, by sex: 2014, 2015, 2016, and 2017
Year Total
Sex
Male Female
Life expectancy at birth, in years
2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.9 76.5 81.3
2015
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.7 76.3 81.1
2016
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.7 76.2 81.1
2017
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.6 76.1 81.1
Life expectancy at birth, by race and Hispanic origin: 2007–2017
Year All races
Race and Hispanic origin
2
Hispanic or
Latino
3
Not Hispanic or Latino
White
Black or
African American
Both sexes Life expectancy at birth, in years
2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.1 80.7 78.4 73.5
2008 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.2 80.8 78.4 73.9
2009 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.5 81.1 78.7 74.4
2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.7 81.7 78.8 74.7
2011 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.7 81.8 78.7 75.0
2012 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.8 81.9 78.9 75.1
2013 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.8 81.9 78.8 75.1
2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.9 82.1 78.8 75.3
2015
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.7 81.9 78.7 75.1
2016
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.7 81.8 78.6 74.9
2017
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 78.6 81.8 78.5 74.9
1
Life expectancy estimates for 2015 and 2016 were revised using updated Medicare data; therefore, these values may differ from previous editions of Health, United States. Life
expectancy estimates for 2017 use preliminary Medicare data.
2
Starting with 2003 data, some states reported multiple-race data for births and deaths according to the 1997 OMB standards. The multiple-race data for these states were
bridged to the four single-race categories of the 1977 OMB standards, for comparability across the trend. See Appendix II, Hispanic origin; Race.
3
Persons of Hispanic origin may be of any race. See Appendix II, Hispanic origin. Life expectancies for the Hispanic population are adjusted for underreporting of Hispanic
ethnicity on the death certificate, but are not adjusted to account for the potential effects of return migration. To address the effects of age misstatement at the oldest ages,
the probability of death for Hispanic persons aged 80 and over is estimated as a function of non-Hispanic white mortality with the use of the Brass relational logit model. See
Appendix II, Race, for a discussion of sources of bias in death rates by race and Hispanic origin.
NOTES: Populations for computing life expectancy for 2007–2009 were based on revised intercensal population estimates of the U.S. resident population. Populations
for computing life expectancy for 2010 were based on 2010 census counts. Life expectancy for 2011 and beyond was computed using 2010-based postcensal estimates.
See Appendix I, Population Census and Population Estimates. In 2008, the life table methodology was revised. Estimates for 2007 and onwards were revised based on the
methodology used in the 2008 life table report. Life expectancy for 2001–2017, except as noted in footnote 1, was calculated using data from Medicare to supplement vital
statistics and census data. Starting with Health, United States, 2016, life expectancy estimates for 2010–2015 were revised to take into account updated race and Hispanic-origin
classification ratios. See Arias E, Heron M, Hakes JK. The validity of race and Hispanic-origin reporting on death certificates in the United States: An update. NCHS. Vital Health
Stat 2(172). 2016. Available from: https://www.cdc.gov/nchs/data/series/sr_02/sr02_172.pdf. Life expectancy is not currently available for persons of other racial and ethnic
groups. See Appendix II, Life expectancy.
SOURCE: NCHS, National Vital Statistics System, Mortality. See Appendix I, National Vital Statistics System (NVSS).

Health, United States, 2018 27
Data table for Figure 2. Infant mortality rates, by race and Hispanic origin of mother and leading causes of death:
United States, 2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_002
Infant mortality rates, by race and Hispanic origin, 2007–2017
Year All mothers
Race and Hispanic origin
1
Hispanic or
Latina
Not Hispanic or Latina
White
Black or
African American
Asian or
Pacific
Islander
American
Indian or
Alaska Native
Infant deaths per 1,000 live births
2
2007 . . . . . . . . . . . . . . . . . . . . . . . 6.75 5.51 5.63 13.31 4.60 9.37
2008 . . . . . . . . . . . . . . . . . . . . . . . 6.61 5.59 5.53 12.67 4.39 8.67
2009 . . . . . . . . . . . . . . . . . . . . . . . 6.39 5.29 5.33 12.40 4.27 9.17
2010 . . . . . . . . . . . . . . . . . . . . . . . 6.14 5.25 5.18 11.46 4.18 8.64
2011 . . . . . . . . . . . . . . . . . . . . . . . 6.07 5.15 5.07 11.45 4.18 8.52
2012 . . . . . . . . . . . . . . . . . . . . . . . 5.98 5.11 5.04 11.19 3.96 8.73
2013 . . . . . . . . . . . . . . . . . . . . . . . 5.96 5.00 5.06 11.11 3.90 7.72
2014 . . . . . . . . . . . . . . . . . . . . . . . 5.82 5.01 4.89 10.93 3.68 7.66
2015 . . . . . . . . . . . . . . . . . . . . . . . 5.90 4.96 4.90 11.25 4.08 8.58
2016 . . . . . . . . . . . . . . . . . . . . . . . 5.87 4.96 4.87 11.21 3.83 8.81
2017 . . . . . . . . . . . . . . . . . . . . . . . 5.79 5.10 4.69 10.88 4.03 8.90
Standard error
2007 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.14 0.14 0.47
2008 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.15 0.14 0.45
2009 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.14 0.13 0.47
2010 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.14 0.13 0.47
2011 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.08 0.05 0.14 0.13 0.47
2012 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.08 0.05 0.14 0.12 0.48
2013 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.14 0.12 0.45
2014 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.14 0.12 0.45
2015 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.14 0.12 0.48
2016 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.07 0.05 0.14 0.12 0.50
2017 . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.08 0.05 0.14 0.12 0.51
See footnotes at end of table.

28 Health, United States, 2018
Data table for Figure 2. Infant mortality rates, by race and Hispanic origin of mother and leading causes of death:
United States, 2007–2017—Con.
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_002
Infant mortality rates, by leading causes of death: 2007–2017
Year
Leading causes of death
3
Congenital
malformations
Preterm births and
low birthweight
Sudden infant
death syndrome
Maternal complications
of pregnancy
Unintentional
injuries (accidents)
Infant deaths per 100,000 live births
2
2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . 134.9 112.7 57.0 41.1 29.7
2008 . . . . . . . . . . . . . . . . . . . . . . . . . . . 133.7 112.0 55.3 41.8 30.9
2009 . . . . . . . . . . . . . . . . . . . . . . . . . . . 129.7 109.6 54.0 39.1 28.4
2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . 127.9 103.8 51.5 39.1 27.7
2011 . . . . . . . . . . . . . . . . . . . . . . . . . . . 126.9 104.1 48.2 40.4 29.5
2012 . . . . . . . . . . . . . . . . . . . . . . . . . . . 125.7 106.6 42.4 38.4 29.4
2013 . . . . . . . . . . . . . . . . . . . . . . . . . . . 121.5 107.1 39.7 40.6 29.3
2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . 119.2 104.6 38.6 39.6 29.2
2015 . . . . . . . . . . . . . . . . . . . . . . . . . . . 121.8 102.7 39.4 38.4 32.4
2016 . . . . . . . . . . . . . . . . . . . . . . . . . . . 122.2 99.5 38.0 35.7 30.8
2017 . . . . . . . . . . . . . . . . . . . . . . . . . . . 119.2 97.5 35.3 37.2 34.1
Standard error
2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.77 1.62 1.15 0.98 0.83
2008 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.78 1.62 1.14 0.99 0.85
2009 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.77 1.63 1.14 0.97 0.83
2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.79 1.61 1.13 0.99 0.83
2011 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.79 1.62 1.10 1.01 0.86
2012 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.78 1.64 1.04 0.99 0.86
2013 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.76 1.65 1.00 1.02 0.86
2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.73 1.62 0.98 1.00 0.86
2015 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.75 1.61 1.00 0.98 0.90
2016 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.76 1.59 0.98 0.95 0.88
2017 . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.76 1.59 0.96 0.98 0.94
1
Starting with 2003 data, some states reported multiple-race data for births and deaths according to the 1997 OMB standards. The multiple-race data for these states were
bridged to the four single-race categories of the 1977 OMB standards, for comparability across the trend. Persons of Hispanic origin may be of any race. See Appendix I,
Population Census and Population Estimates; Appendix II, Hispanic origin; Race.
2
Infants are defined as under 1 year of age. Rates are based on the number of deaths from the mortality file and the number of births from the natality file.
3
Deaths are identified using International Classification of Diseases, 10th revision (ICD–10). The codes were: Congenital malformations, deformations and chromosomal
abnormalities (Q00–Q99); Disorders related to preterm births (short gestation) and low birthweight, not elsewhere classified (P07); Sudden infant death syndrome (R95);
Newborn affected by maternal complications of pregnancy of pregnancy (P01); and Accidents (unintentional injuries) (V01–X59). The cause of death, newborn affected by
maternal complications of pregnancy, includes any of the following conditions: incompetent cervix, premature rupture of membranes, ectopic pregnancy, malpresentation
before labor, amniotic fluid disorders, multiple pregnancy, maternal death, and other unspecified maternal complications. See Appendix II, Cause of death; Table IV.
NOTES: Infant mortality rates by race and Hispanic origin are from the Linked Birth/Infant Death data set, for which the most recent data year available is 2017. Age-adjusted
rates are calculated using the year 2000 standard population with unrounded population numbers. See Appendix II, Cause of death; Table IV; Hispanic origin; Race.
SOURCE: NCHS, National Vital Statistics System, Linked Birth/Infant Death Data Set. See Appendix I, National Vital Statistics System (NVSS).

Health, United States, 2018 29
Data table for Figure 3. Age-adjusted death rates for selected causes of death for all ages, by sex: United States, 2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_003
Sex and year All causes
Cause of death
1
Heart disease Cancer
Unintentional
injuries
2
CLRD
3
Stroke
4
Diabetes
5
Alzheimer’s
disease
All persons Age-adjusted deaths per 100,000 population
6
2007 . . . . . . . . . . . . . . . . . . 775.3 196.1 179.3 40.4 41.4 43.5 22.8 23.8
2008 . . . . . . . . . . . . . . . . . . 774.9 192.1 176.4 39.2 44.7 42.1 22.0 25.8
2009 . . . . . . . . . . . . . . . . . . 749.6 182.8 173.5 37.5 42.7 39.6 21.0 24.2
2010 . . . . . . . . . . . . . . . . . . 747.0 179.1 172.8 38.0 42.2 39.1 20.8 25.1
2011 . . . . . . . . . . . . . . . . . . 741.3 173.7 169.0 39.1 42.5 37.9 21.6 24.7
2012 . . . . . . . . . . . . . . . . . . 732.8 170.5 166.5 39.1 41.5 36.9 21.2 23.8
2013 . . . . . . . . . . . . . . . . . . 731.9 169.8 163.2 39.4 42.1 36.2 21.2 23.5
2014 . . . . . . . . . . . . . . . . . . 724.6 167.0 161.2 40.5 40.5 36.5 20.9 25.4
2015 . . . . . . . . . . . . . . . . . . 733.1 168.5 158.5 43.2 41.6 37.6 21.3 29.4
2016 . . . . . . . . . . . . . . . . . . 728.8 165.5 155.8 47.4 40.6 37.3 21.0 30.3
2017 . . . . . . . . . . . . . . . . . . 731.9 165.0 152.5 49.4 40.9 37.6 21.5 31.0
Male
2007 . . . . . . . . . . . . . . . . . . 922.9 243.7 218.8 55.9 48.8 43.7 26.6 19.5
2008 . . . . . . . . . . . . . . . . . . 918.8 238.5 214.9 54.3 52.3 42.2 25.9 21.3
2009 . . . . . . . . . . . . . . . . . . 890.9 229.4 210.9 51.4 49.5 39.9 25.0 20.2
2010 . . . . . . . . . . . . . . . . . . 887.1 225.1 209.9 51.5 48.7 39.3 24.9 21.0
2011 . . . . . . . . . . . . . . . . . . 875.3 218.1 204.0 52.8 48.6 37.9 26.0 20.4
2012 . . . . . . . . . . . . . . . . . . 865.1 214.7 200.3 52.6 47.2 37.1 25.5 19.8
2013 . . . . . . . . . . . . . . . . . . 863.6 214.5 196.0 53.1 47.5 36.7 25.6 19.3
2014 . . . . . . . . . . . . . . . . . . 855.1 210.9 192.9 54.6 45.4 36.9 25.6 20.6
2015 . . . . . . . . . . . . . . . . . . 863.2 211.8 189.2 58.7 46.0 37.8 26.2 23.7
2016 . . . . . . . . . . . . . . . . . . 861.0 209.1 185.4 65.0 45.1 37.5 26.0 24.3
2017 . . . . . . . . . . . . . . . . . . 864.5 209.0 181.1 67.8 45.0 38.0 26.8 24.9
Female
2007 . . . . . . . . . . . . . . . . . . 658.1 159.0 152.3 26.1 36.6 42.7 19.8 26.2
2008 . . . . . . . . . . . . . . . . . . 659.9 155.9 149.6 25.4 39.8 41.4 19.1 28.2
2009 . . . . . . . . . . . . . . . . . . 636.8 146.6 147.4 24.8 38.3 38.8 17.9 26.3
2010 . . . . . . . . . . . . . . . . . . 634.9 143.3 146.7 25.6 38.0 38.3 17.6 27.3
2011 . . . . . . . . . . . . . . . . . . 632.4 138.7 144.0 26.5 38.5 37.2 18.2 27.1
2012 . . . . . . . . . . . . . . . . . . 624.7 135.5 142.1 26.4 37.8 36.1 17.7 26.1
2013 . . . . . . . . . . . . . . . . . . 623.5 134.3 139.5 26.6 38.5 35.2 17.6 25.9
2014 . . . . . . . . . . . . . . . . . . 616.7 131.8 138.1 27.3 37.1 35.6 17.2 28.3
2015 . . . . . . . . . . . . . . . . . . 624.2 133.6 135.9 28.7 38.6 36.9 17.3 32.8
2016 . . . . . . . . . . . . . . . . . . 617.5 130.4 134.0 30.8 37.4 36.5 16.9 33.9
2017 . . . . . . . . . . . . . . . . . . 619.7 129.6 131.4 32.0 38.1 36.6 17.1 34.8
See footnotes at end of table.

30 Health, United States, 2018
Data table for Figure 3. Age-adjusted death rates for selected causes of death for all ages, by sex: United States,
2007–2017—Con.
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_003
Sex and year All causes
Cause of death
1
Heart
disease Cancer
Unintentional
injuries
2
CLRD
3
Stroke
4
Diabetes
5
Alzheimer’s
disease
All persons Standard error
2007 . . . . . . . . . . . . . . . . . . 0.50 0.25 0.24 0.12 0.12 0.12 0.09 0.09
2008 . . . . . . . . . . . . . . . . . . 0.50 0.25 0.24 0.11 0.12 0.12 0.08 0.09
2009 . . . . . . . . . . . . . . . . . . 0.48 0.24 0.23 0.11 0.12 0.11 0.08 0.09
2010 . . . . . . . . . . . . . . . . . . 0.48 0.23 0.23 0.11 0.11 0.11 0.08 0.09
2011 . . . . . . . . . . . . . . . . . . 0.47 0.23 0.22 0.11 0.11 0.11 0.08 0.09
2012 . . . . . . . . . . . . . . . . . . 0.46 0.22 0.22 0.11 0.11 0.10 0.08 0.08
2013 . . . . . . . . . . . . . . . . . . 0.46 0.22 0.22 0.11 0.11 0.10 0.08 0.08
2014 . . . . . . . . . . . . . . . . . . 0.45 0.22 0.21 0.11 0.11 0.10 0.08 0.08
2015 . . . . . . . . . . . . . . . . . . 0.45 0.21 0.21 0.11 0.11 0.10 0.08 0.09
2016 . . . . . . . . . . . . . . . . . . 0.45 0.21 0.20 0.12 0.10 0.10 0.08 0.09
2017 . . . . . . . . . . . . . . . . . . 0.44 0.21 0.20 0.12 0.10 0.10 0.08 0.09
Male
2007 . . . . . . . . . . . . . . . . . . 0.86 0.45 0.41 0.20 0.20 0.19 0.14 0.13
2008 . . . . . . . . . . . . . . . . . . 0.84 0.43 0.40 0.20 0.20 0.18 0.14 0.14
2009 . . . . . . . . . . . . . . . . . . 0.82 0.42 0.39 0.19 0.20 0.18 0.14 0.13
2010 . . . . . . . . . . . . . . . . . . 0.81 0.41 0.39 0.19 0.19 0.17 0.13 0.13
2011 . . . . . . . . . . . . . . . . . . 0.79 0.40 0.38 0.19 0.19 0.17 0.14 0.13
2012 . . . . . . . . . . . . . . . . . . 0.78 0.39 0.37 0.19 0.18 0.16 0.13 0.12
2013 . . . . . . . . . . . . . . . . . . 0.77 0.38 0.36 0.19 0.18 0.16 0.13 0.12
2014 . . . . . . . . . . . . . . . . . . 0.75 0.38 0.35 0.19 0.18 0.16 0.13 0.12
2015 . . . . . . . . . . . . . . . . . . 0.75 0.37 0.34 0.20 0.17 0.16 0.13 0.13
2016 . . . . . . . . . . . . . . . . . . 0.74 0.37 0.34 0.21 0.17 0.16 0.13 0.13
2017 . . . . . . . . . . . . . . . . . . 0.73 0.36 0.33 0.21 0.17 0.16 0.13 0.13
Female
2007 . . . . . . . . . . . . . . . . . . 0.60 0.29 0.30 0.13 0.14 0.15 0.11 0.11
2008 . . . . . . . . . . . . . . . . . . 0.60 0.29 0.29 0.12 0.15 0.15 0.10 0.12
2009 . . . . . . . . . . . . . . . . . . 0.59 0.27 0.29 0.12 0.14 0.14 0.10 0.11
2010 . . . . . . . . . . . . . . . . . . 0.58 0.27 0.28 0.12 0.14 0.14 0.10 0.11
2011 . . . . . . . . . . . . . . . . . . 0.57 0.26 0.28 0.12 0.14 0.14 0.10 0.11
2012 . . . . . . . . . . . . . . . . . . 0.57 0.26 0.27 0.12 0.14 0.13 0.10 0.11
2013 . . . . . . . . . . . . . . . . . . 0.56 0.25 0.27 0.12 0.14 0.13 0.09 0.11
2014 . . . . . . . . . . . . . . . . . . 0.55 0.25 0.27 0.13 0.14 0.13 0.09 0.11
2015 . . . . . . . . . . . . . . . . . . 0.55 0.25 0.26 0.13 0.14 0.13 0.09 0.12
2016 . . . . . . . . . . . . . . . . . . 0.55 0.24 0.26 0.13 0.13 0.13 0.09 0.12
2017 . . . . . . . . . . . . . . . . . . 0.54 0.24 0.25 0.13 0.13 0.13 0.09 0.12
1
Underlying causes of death are based on the International Classification of Diseases, 10th revision (ICD–10).
2
Unintentional injuries is another term for accidents.
3
CLRD is chronic lower respiratory disease.
4
Stroke is another term for cerebrovascular disease.
5
Starting with 2011 data, the rules for selecting renal failure as the underlying cause of death were changed, resulting in an increase in the number of deaths for Diabetes
mellitus. Therefore, data for diabetes before and after 2011 are not directly comparable. For more information, see Technical Notes in Deaths: Final data for 2011, available
from: https://www.cdc.gov/nchs/data/nvsr/nvsr63/nvsr63_03.pdf.
6
Estimates are age adjusted to the year 2000 standard population with unrounded population numbers. See Appendix II, Age adjustment.
NOTE: See Appendix II, Cause of death; Cause-of-death ranking; Table IV.
SOURCE: NCHS, National Vital Statistics System, Mortality. See Appendix I, National Vital Statistics System (NVSS).

Health, United States, 2018 31
Data table for Figure 4. Drug overdose death rates, by sex and age: United States, 2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_004
Sex and year
All ages Age group (years)
Total
(age adjusted)
1
Total
(crude) 15–24 25–34 35–44 45–54 55–64
65 and
over
All persons Deaths per 100,000 population
2007 . . . . . . . . . . . . . . . . . . . . 11.9 12.0 8.2 16.8 21.4 25.1 12.2 3.8
2008 . . . . . . . . . . . . . . . . . . . . 11.9 12.0 8.0 16.8 21.1 25.2 12.9 4.1
2009 . . . . . . . . . . . . . . . . . . . . 11.9 12.1 7.7 17.2 20.5 25.4 13.7 4.3
2010 . . . . . . . . . . . . . . . . . . . . 12.3 12.4 8.2 18.4 20.8 25.1 15.0 4.3
2011 . . . . . . . . . . . . . . . . . . . . 13.2 13.3 8.6 20.2 22.5 26.7 15.9 4.6
2012 . . . . . . . . . . . . . . . . . . . . 13.1 13.2 8.0 20.1 22.1 26.9 16.6 4.9
2013 . . . . . . . . . . . . . . . . . . . . 13.8 13.9 8.3 20.9 23.0 27. 5 19.2 5.2
2014 . . . . . . . . . . . . . . . . . . . . 14.7 14.8 8.6 23.1 25.0 28.2 20.3 5.6
2015 . . . . . . . . . . . . . . . . . . . . 16.3 16.3 9.7 26.9 28.3 30.0 21.8 5.8
2016 . . . . . . . . . . . . . . . . . . . . 19.8 19.7 12.4 34.6 35.0 34.5 25.6 6.2
2017 . . . . . . . . . . . . . . . . . . . . 21.7 21.6 12.6 38.4 39.0 37.7 28.0 6.9
Male
2007 . . . . . . . . . . . . . . . . . . . . 14.9 15.1 12.0 23.4 26.7 29.2 14.0 4.0
2008 . . . . . . . . . . . . . . . . . . . . 14.9 15.0 11.9 23.6 25.6 29.6 14.8 4.2
2009 . . . . . . . . . . . . . . . . . . . . 14.8 15.0 11.3 24.0 25.2 29.1 16.0 4.4
2010 . . . . . . . . . . . . . . . . . . . . 15.0 15.2 11.6 25.0 24.9 28.5 17.3 4.3
2011 . . . . . . . . . . . . . . . . . . . . 16.1 16.3 12.4 27. 5 26.8 30.4 18.5 4.7
2012 . . . . . . . . . . . . . . . . . . . . 16.1 16.3 11.4 27.0 27.1 30.4 19.4 5.2
2013 . . . . . . . . . . . . . . . . . . . . 17.0 17.2 11.7 28.6 28.1 31.5 22.7 5.9
2014 . . . . . . . . . . . . . . . . . . . . 18.3 18.4 12.1 31.9 30.8 32.9 23.5 6.0
2015 . . . . . . . . . . . . . . . . . . . . 20.8 20.8 13.3 37.9 36.3 35.3 26.2 6.8
2016 . . . . . . . . . . . . . . . . . . . . 26.2 26.1 17.5 48.9 46.9 42.5 32.2 7.6
2017 . . . . . . . . . . . . . . . . . . . . 29.1 29.0 17.1 54.3 53.0 48.3 36.2 8.7
Female
2007 . . . . . . . . . . . . . . . . . . . . 8.8 9.0 4.2 10.1 16.1 21.0 10.5 3.6
2008 . . . . . . . . . . . . . . . . . . . . 8.9 9.0 4.0 9.9 16.5 21.0 11.1 4.0
2009 . . . . . . . . . . . . . . . . . . . . 9.1 9.2 4.1 10.4 16.0 21.8 11.6 4.3
2010 . . . . . . . . . . . . . . . . . . . . 9.6 9.8 4.6 11.9 16.8 21.8 12.9 4.3
2011 . . . . . . . . . . . . . . . . . . . . 10.2 10.3 4.6 12.8 18.2 23.1 13.5 4.5
2012 . . . . . . . . . . . . . . . . . . . . 10.2 10.3 4.4 13.1 17.1 23.4 14.0 4.6
2013 . . . . . . . . . . . . . . . . . . . . 10.6 10.7 4.8 13.0 18.0 23.6 15.9 4.8
2014 . . . . . . . . . . . . . . . . . . . . 11.1 11.3 5.0 14.1 19.2 23.7 17.2 5.2
2015 . . . . . . . . . . . . . . . . . . . . 11.8 11.9 5.9 15.7 20.5 24.9 17.6 5.0
2016 . . . . . . . . . . . . . . . . . . . . 13.4 13.5 7.0 19.9 23.3 26.7 19.5 5.1
2017 . . . . . . . . . . . . . . . . . . . . 14.4 14.3 7.9 22.0 25.1 27.5 20.3 5.5
See footnotes at end of table.

32 Health, United States, 2018
Data table for Figure 4. Drug overdose death rates, by sex and age: United States, 2007–2017—Con.
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_004
Sex and year
All ages Age group (years)
Total
(age adjusted)
1
Total
(crude) 15–24 25–34 35–44 45–54 55–64
65 and
over
All persons Standard error
2007 . . . . . . . . . . . . . . . . . . . . 0.06 0.06 0.14 0.21 0.22 0.24 0.19 0.10
2008 . . . . . . . . . . . . . . . . . . . . 0.06 0.06 0.14 0.20 0.22 0.24 0.19 0.10
2009 . . . . . . . . . . . . . . . . . . . . 0.06 0.06 0.13 0.21 0.22 0.24 0.20 0.10
2010 . . . . . . . . . . . . . . . . . . . . 0.06 0.06 0.14 0.21 0.23 0.24 0.20 0.10
2011 . . . . . . . . . . . . . . . . . . . . 0.07 0.07 0.14 0.22 0.24 0.24 0.20 0.11
2012 . . . . . . . . . . . . . . . . . . . . 0.07 0.06 0.13 0.22 0.23 0.25 0.21 0.11
2013 . . . . . . . . . . . . . . . . . . . . 0.07 0.07 0.14 0.22 0.24 0.25 0.22 0.11
2014 . . . . . . . . . . . . . . . . . . . . 0.07 0.07 0.14 0.23 0.25 0.25 0.22 0.11
2015 . . . . . . . . . . . . . . . . . . . . 0.07 0.07 0.15 0.25 0.26 0.26 0.23 0.11
2016 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.17 0.28 0.29 0.28 0.25 0.11
2017 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.17 0.29 0.31 0.30 0.26 0.12
Male
2007 . . . . . . . . . . . . . . . . . . . . 0.10 0.10 0.23 0.34 0.35 0.37 0.30 0.16
2008 . . . . . . . . . . . . . . . . . . . . 0.10 0.10 0.23 0.34 0.35 0.37 0.30 0.16
2009 . . . . . . . . . . . . . . . . . . . . 0.10 0.10 0.22 0.34 0.35 0.36 0.31 0.16
2010 . . . . . . . . . . . . . . . . . . . . 0.10 0.10 0.23 0.35 0.35 0.36 0.31 0.16
2011 . . . . . . . . . . . . . . . . . . . . 0.10 0.10 0.23 0.36 0.36 0.37 0.32 0.16
2012 . . . . . . . . . . . . . . . . . . . . 0.10 0.10 0.23 0.36 0.37 0.37 0.32 0.17
2013 . . . . . . . . . . . . . . . . . . . . 0.11 0.11 0.23 0.36 0.37 0.38 0.35 0.17
2014 . . . . . . . . . . . . . . . . . . . . 0.11 0.11 0.23 0.38 0.39 0.39 0.35 0.17
2015 . . . . . . . . . . . . . . . . . . . . 0.12 0.11 0.24 0.41 0.42 0.41 0.36 0.18
2016 . . . . . . . . . . . . . . . . . . . . 0.13 0.13 0.28 0.47 0.48 0.45 0.40 0.19
2017 . . . . . . . . . . . . . . . . . . . . 0.14 0.13 0.28 0.49 0.51 0.48 0.42 0.20
Female
2007 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.14 0.23 0.27 0.31 0.25 0.13
2008 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.14 0.22 0.28 0.31 0.25 0.13
2009 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.14 0.23 0.28 0.31 0.25 0.14
2010 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.15 0.24 0.29 0.31 0.26 0.14
2011 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.15 0.25 0.30 0.32 0.26 0.14
2012 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.14 0.25 0.29 0.32 0.27 0.14
2013 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.15 0.25 0.30 0.33 0.28 0.14
2014 . . . . . . . . . . . . . . . . . . . . 0.08 0.08 0.15 0.26 0.31 0.33 0.29 0.14
2015 . . . . . . . . . . . . . . . . . . . . 0.09 0.09 0.17 0.27 0.32 0.34 0.29 0.14
2016 . . . . . . . . . . . . . . . . . . . . 0.09 0.09 0.18 0.30 0.34 0.35 0.30 0.14
2017 . . . . . . . . . . . . . . . . . . . . 0.10 0.09 0.19 0.31 0.35 0.36 0.31 0.14
1
Estimates are age adjusted to the year 2000 standard population with unrounded population numbers. See Appendix II, Age adjustment.
NOTES: Drug overdose deaths are identified using International Classification of Diseases, 10th revision (ICD–10) underlying cause of death codes X40–X44 (unintentional drug
poisoning), X60–X64 (suicide by drug poisoning), X85 (homicide by drug poisoning), and Y10–Y14 (drug poisoning of undetermined intent). See Appendix II, Cause of death;
Table IV.
SOURCE: NCHS, National Vital Statistics System, Mortality. See Appendix I, National Vital Statistics System (NVSS).

Health, United States, 2018 33
Data table for Figure 5. Teen births among females aged 15–19 years, by race and Hispanic origin: United States, 2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_005
Year Total
Race and Hispanic origin of mother
1
Hispanic or Latina
Not Hispanic or Latina
White only
Black or
African American
only
Asian or
Pacific
Islander only
American
Indian or Alaska
Native only
Live births per 1,000 females aged 15–19 years
2007 . . . . . . . . . . . . . . . . . . . . . . . . . 41.5 75.3 27.2 62.0 13.4 66.3
2008 . . . . . . . . . . . . . . . . . . . . . . . . . 40.2 70.3 26.7 60.4 12.4 65.0
2009 . . . . . . . . . . . . . . . . . . . . . . . . . 37.9 63.6 25.7 56.8 11.3 62.0
2010 . . . . . . . . . . . . . . . . . . . . . . . . . 34.2 55.7 23.5 51.5 9.9 55.5
2011 . . . . . . . . . . . . . . . . . . . . . . . . . 31.3 49.6 21.7 47.3 9.0 52.6
2012 . . . . . . . . . . . . . . . . . . . . . . . . . 29.4 46.3 20.5 43.9 8.5 51.2
2013 . . . . . . . . . . . . . . . . . . . . . . . . . 26.5 41.7 18.6 39.0 7.8 44.9
2014 . . . . . . . . . . . . . . . . . . . . . . . . . 24.2 38.0 17.3 34.9 6.8 39.3
2015 . . . . . . . . . . . . . . . . . . . . . . . . . 22.3 34.9 16.0 31.8 6.0 37.6
2016 . . . . . . . . . . . . . . . . . . . . . . . . . 20.3 31.9 14.4 29.3 5.2 34.7
2017 . . . . . . . . . . . . . . . . . . . . . . . . . 18.8 28.9 13.4 27.6 4.6 32.2
Standard error
2007 . . . . . . . . . . . . . . . . . . . . . . . . . 0.06 0.20 0.07 0.19 0.16 0.75
2008 . . . . . . . . . . . . . . . . . . . . . . . . . 0.06 0.18 0.06 0.19 0.16 0.74
2009 . . . . . . . . . . . . . . . . . . . . . . . . . 0.06 0.17 0.06 0.18 0.15 0.73
2010 . . . . . . . . . . . . . . . . . . . . . . . . . 0.06 0.16 0.06 0.17 0.14 0.70
2011 . . . . . . . . . . . . . . . . . . . . . . . . . 0.05 0.15 0.06 0.17 0.13 0.69
2012 . . . . . . . . . . . . . . . . . . . . . . . . . 0.05 0.14 0.06 0.16 0.13 0.69
2013 . . . . . . . . . . . . . . . . . . . . . . . . . 0.05 0.14 0.06 0.16 0.12 0.65
2014 . . . . . . . . . . . . . . . . . . . . . . . . . 0.05 0.13 0.05 0.15 0.11 0.61
2015 . . . . . . . . . . . . . . . . . . . . . . . . . 0.05 0.12 0.05 0.14 0.10 0.60
2016 . . . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.12 0.05 0.14 0.09 0.58
2017 . . . . . . . . . . . . . . . . . . . . . . . . . 0.04 0.11 0.05 0.13 0.09 0.56
1
Starting with 2003 data, some states reported multiple-race data for births and deaths according to the 1997 OMB standards. The multiple-race data for these states were
bridged to the four single-race categories of the 1977 OMB standards, for comparability across the trend. Persons of Hispanic origin may be of any race. See Appendix I,
Population Census and Population Estimates; Appendix II, Hispanic origin; Race.
SOURCE: NCHS, National Vital Statistics System, Natality. See Appendix I, National Vital Statistics System (NVSS).
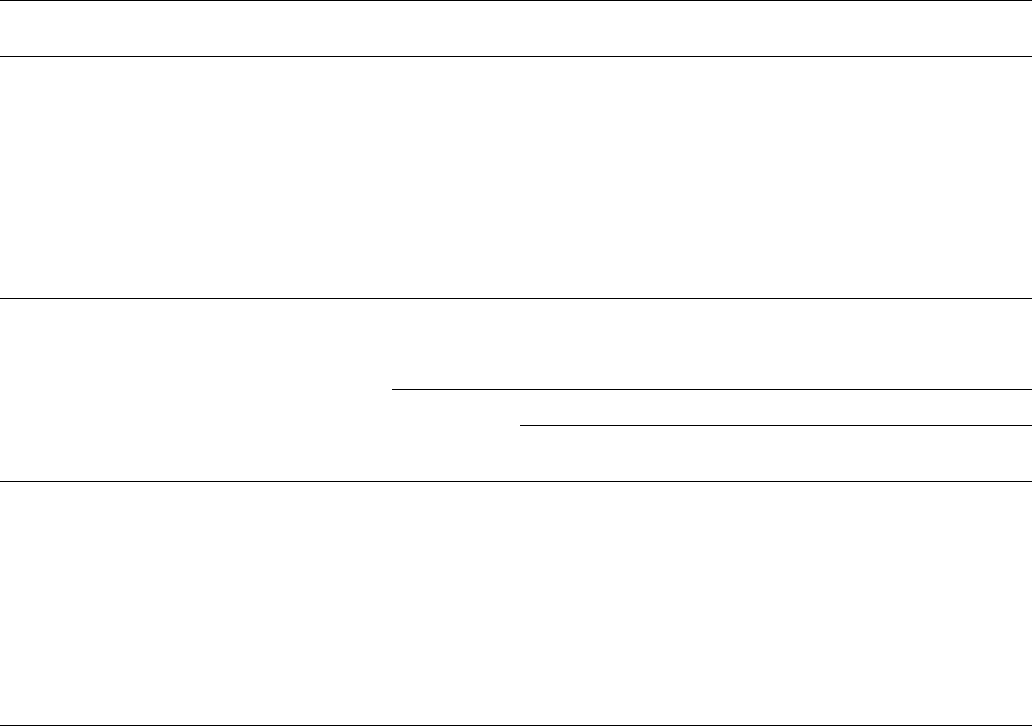
34 Health, United States, 2018
Data table for Figure 6. Preterm singleton births, by gestational age and race and Hispanic origin of mother: United States,
2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_006
Preterm singleton births, by gestational age, 2007–2017
Preterm singleton births by
gestational age, in weeks
1
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017
Percent of live singleton births that were preterm
Total (less than 37) . . . . . . . . . . . . . . 8.6 8.5 8.2 8.1 8.0 8.0 7.8 7.7 7.8 8.0 8.1
34–36 . . . . . . . . . . . . . . . . . . . . . . . 6.4 6.3 6.1 6.0 5.9 5.8 5.7 5.7 5.7 5.9 6.0
32–33 . . . . . . . . . . . . . . . . . . . . . . . 0.9 0.9 0.9 0.9 0.9 0.9 0.9 0.8 0.9 0.9 0.9
Less than 32 . . . . . . . . . . . . . . . . . . 1.3 1.3 1.3 1.3 1.3 1.3 1.2 1.2 1.2 1.2 1.2
Standard error
Total (less than 37) . . . . . . . . . . . . . . 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01
34–36 . . . . . . . . . . . . . . . . . . . . . . . 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01
32–33 . . . . . . . . . . . . . . . . . . . . . . . 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00
Less than 32 . . . . . . . . . . . . . . . . . . 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01 0.01
Preterm singleton births, by gestational age and race and Hispanic origin of mother, 2017
Preterm singleton births by
gestational age and race and
Hispanic origin, in weeks
1
Total
3
Race and Hispanic origin of mother
2
Hispanic or
Latina
Not Hispanic or Latina
White only
Black or African
American only
Asian or Pacific
Islander only
American Indian or
Alaska Native only
Percent of live singleton births that were preterm
4
Total (less than 37) . . . . . . . . . . . . . . . . . 8.1 8.3 7.1 11.6 7.2 10.4
34–36 . . . . . . . . . . . . . . . . . . . . . . . . . . 6.0 6.2 5.5 7.7 5.5 7.8
32–33 . . . . . . . . . . . . . . . . . . . . . . . . . . 0.9 0.9 0.7 1.3 0.8 1.1
Less than 32 . . . . . . . . . . . . . . . . . . . . . 1.2 1.2 0.9 2.5 0.9 1.5
Standard error
Total (less than 37) . . . . . . . . . . . . . . . . . 0.01 0.03 0.02 0.04 0.05 0.17
34–36 . . . . . . . . . . . . . . . . . . . . . . . . . . 0.01 0.03 0.02 0.04 0.04 0.15
32–33 . . . . . . . . . . . . . . . . . . . . . . . . . . 0.00 0.01 0.01 0.02 0.02 0.06
Less than 32 . . . . . . . . . . . . . . . . . . . . . 0.01 0.01 0.01 0.02 0.02 0.07
0.00 Quantity more than zero but less than 0.005
1
Preterm births are based on the obstetric estimate of gestational age and are for all singleton births. Singleton births refer to single births, in contrast with multiple or higher
order births. Estimates for the percentage of live singleton births that occurred less than 37 weeks of gestation may not sum to total percentage due to rounding. For more
information on the obstetric estimates, see Appendix II, Gestation and Martin JA, Osterman MJK, Kirmeyer SE, Gregory ECW. Measuring gestational age in vital statistics data:
Transitioning to the obstetric estimate. National vital statistics reports; vol 64 no 5. Hyattsville, MD: NCHS. 2015. Available from: https://www.cdc.gov/nchs/data/nvsr/nvsr64/
nvsr64_05.pdf.
2
Persons of Hispanic origin may be of any race. Starting with 2003 data, some states reported multiple-race data for births and deaths according to the 1997 OMB standards.
The multiple-race data for these states were bridged to the four single-race categories of the 1977 OMB standards, for comparability across the trend. See Appendix II, Hispanic
origin; Race.
3
Includes all preterm births not shown separately.
4
Estimates may not sum to total percentage due to rounding.
SOURCE: NCHS, National Vital Statistics System, Natality. See Appendix I, National Vital Statistics System (NVSS).

Health, United States, 2018 35
Data table for Figure 7. Cigarette smoking among adults aged 18 and over by age, and tobacco use among adolescents in
grades 9–12 by type of product: United States, 2007–2018
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_007
Current cigarette smoking among adults aged 18 and over, by age: 2007–2017
Year
18 and over 18–44 45–64 65 and over
Percent
(age adjusted)
1
SE
Percent
(crude) SE Percent SE Percent SE Percent SE
2007 . . . . . . . . . . 19.7 0.4 19.8 0.4 22.6 0.6 21.0 0.6 8.3 0.5
2008 . . . . . . . . . . 20.6 0.4 20.6 0.4 23.1 0.6 22.6 0.6 9.3 0.5
2009 . . . . . . . . . . 20.6 0.4 20.6 0.4 23.4 0.5 21.9 0.6 9.5 0.5
2010 . . . . . . . . . . 19.3 0.3 19.3 0.3 21.5 0.5 21.1 0.5 9.5 0.5
2011 . . . . . . . . . . 19.0 0.3 19.0 0.3 21.2 0.5 21.4 0.5 7.9 0.4
2012 . . . . . . . . . . 18.2 0.3 18.1 0.3 20.4 0.5 19.5 0.5 8.9 0.4
2013 . . . . . . . . . . 17.9 0.3 17.8 0.3 19.7 0.5 19.9 0.5 8.8 0.4
2014 . . . . . . . . . . 17.0 0.3 16.8 0.3 19.1 0.5 18.0 0.5 8.5 0.4
2015 . . . . . . . . . . 15.3 0.3 15.1 0.3 16.5 0.5 17.0 0.5 8.4 0.4
2016 . . . . . . . . . . 15.7 0.3 15.5 0.3 16.4 0.5 18.0 0.5 8.8 0.4
2017 . . . . . . . . . . 14.1 0.3 14.0 0.3 14.6 0.4 16.5 0.5 8.2 0.4
Tobacco use in the past 30 days among adolescents in grades 9–12, by type of product: 2011–2018
Year
Any tobacco
products
2,3
Electronic
cigarettes
4
Cigarettes
4
Cigars
4
Smokeless
tobacco
4,5
Hookah
4
Pipe
tobacco
4
Percent
2011 . . . . . . . . . . . . . . . . . . . . . . . 24.2 1.5 15.8 11.6 7.9 4.1 4.0
2012 . . . . . . . . . . . . . . . . . . . . . . . 23.3 2.8 14.0 12.6 7.3 5.4 4.5
2013 . . . . . . . . . . . . . . . . . . . . . . . 22.9 4.5 12.7 11.9 6.2 5.2 4.1
2014 . . . . . . . . . . . . . . . . . . . . . . . 24.6 13.4 9.2 8.2 6.3 9.4 1.5
2015 . . . . . . . . . . . . . . . . . . . . . . . 25.3 16.0 9.3 8.6 6.0 7.2 1.0
2016 . . . . . . . . . . . . . . . . . . . . . . . 20.2 11.3 8.0 7.7 5.8 4.8 1.4
2017 . . . . . . . . . . . . . . . . . . . . . . . 19.6 11.7 7.6 7.7 5.5 3.3 0.8
2018 . . . . . . . . . . . . . . . . . . . . . . . 27.1 20.8 8.1 7.6 5.9 4.1 1.1
Standard error
2011 . . . . . . . . . . . . . . . . . . . . . . . 1.2 0.2 1.1 0.6 0.8 0.4 0.3
2012 . . . . . . . . . . . . . . . . . . . . . . . 0.9 0.3 0.8 0.6 0.6 0.4 0.3
2013 . . . . . . . . . . . . . . . . . . . . . . . 0.9 0.4 0.7 0.6 0.7 0.4 0.3
2014 . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.2 0.6 0.5 0.6 0.6 0.2
2015 . . . . . . . . . . . . . . . . . . . . . . . 1.1 1.0 0.8 0.5 0.7 0.5 0.2
2016 . . . . . . . . . . . . . . . . . . . . . . . 1.0 0.8 0.7 0.6 0.6 0.4 0.1
2017 . . . . . . . . . . . . . . . . . . . . . . . 1.3 1.1 0.6 0.6 0.7 0.3 0.1
2018 . . . . . . . . . . . . . . . . . . . . . . . 0.9 1.0 0.6 0.5 0.5 0.3 0.1
See footnotes at end of table.

36 Health, United States, 2018
Data table for Figure 7. Cigarette smoking among adults aged 18 and over by age, and tobacco use among adolescents in
grades 9–12 by type of product: United States, 2007–2018—Con.
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_007
1
Estimates are age adjusted to the year 2000 standard population using five age groups: 18–24, 25–34, 35–44, 45–64, and 65 and over. Age-adjusted estimates in this table may
differ from other age-adjusted estimates based on the same data and presented elsewhere if different age groups are used in the adjustment procedure. See Appendix II, Age
adjustment.
2
Any tobacco product use is defined as use of any tobacco product (electronic cigarettes, cigarettes, cigars/cigarillos/little cigars, smokeless tobacco [includes chewing tobacco/
snuff/dip, snus, and dissolvable tobacco], hookah, pipe tobacco, and bidis) on at least one day in the past 30 days.
3
In 2018, bidis was assessed by the question, “In the past 30 days, which of the following tobacco products have you used on at least one day?” and the response option, “Bidis
(small brown cigarettes wrapped in a leaf ).” Prevalence estimates are not provided for bidis individually; however, use of bidis is captured in the composite measure “any
tobacco product.”
4
In 2018, past 30-day use of electronic cigarettes was determined by asking, “During the past 30 days, on how many days did you use electronic cigarettes or e-cigarettes?”
Electronic cigarettes, or e-cigarettes, are battery-powered tobacco products that typically deliver nicotine in the form of an aerosol. Past 30-day use of cigarettes was
determined by asking, “During the past 30 days, on how many days did you smoke cigarettes?” Past 30-day use of cigars was determined by asking, “During the past 30 days, on
how many days did you smoke cigars, cigarillos, or little cigars?” Smokeless tobacco was defined as use of chewing tobacco, snuff, dip, snus, and dissolvable tobacco products.
Past 30-day use of smokeless tobacco was determined by asking the following question regarding chewing tobacco, snuff, and dip: “During the past 30 days, on how many days
did you use chewing tobacco, snuff, or dip?,” and the following question for use of snus and dissolvable tobacco products: “In the past 30 days, which of the following products
did you use on at least one day: Snus, such as Camel, Marlboro, or General Snus;” Dissolvable tobacco products such as Ariva, Stonewall, Camel orbs, Camel sticks, Marlboro
sticks, or Camel strips?” Responses from these questions were combined to derive overall smokeless tobacco use. Past 30-day use of hookah was determined by asking, “During
the past 30 days, on how many days did you smoke tobacco in a hookah or waterpipe?” Past 30-day use of pipe tobacco was determined by asking, “In the past 30 days, which of
the following products have you used on at least one day: and the response option, “Pipes filled with tobacco (not waterpipe)?”
5
Beginning in 2015, the definition of smokeless tobacco included chewing tobacco/snuff/dip, snus, and dissolvable tobacco products due to a limited sample size for individual
products (snus, dissolvable). This definition of smokeless tobacco was applied across all years presented here (2011–2018) for comparability purposes. Previously published
reports using 2014 and earlier NYTS data used a definition of smokeless tobacco that included only chewing tobacco, snuff, and dip; therefore, estimates from those reports
may not be comparable to those presented here.
NOTES: SE is standard error. Data are for the civilian noninstitutionalized population. Current cigarette smoking by adults is defined as smoking either every day or some days.
Use of tobacco products by students in grades 9–12 is defined as having used the product on one or more days during the past 30 days. See Appendix II, Tobacco use.
SOURCES: NCHS, National Health Interview Survey and CDC, National Youth Tobacco Survey. See Appendix I, National Health Interview Survey (NHIS) and National Youth
Tobacco Survey (NYTS).

Health, United States, 2018 37
Data table for Figure 8. Obesity among children and adolescents aged 2–19 years and adults aged 20 and over by sex:
United States, 1999–2000 through 2015–2016
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_008
Obesity among children and adolescents aged 2–19 years, by sex: 1999–2000 through 2015–2016
Year
Total Male Female
Percent SE Percent SE Percent SE
1999–2000 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13.9 0.9 14.0 1.2 13.8 1.1
2001–2002 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15.4 0.9 16.4 1.0 14.3 1.3
2003–2004 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17.1 1.3 18.2 1.5 16.0 1.4
2005–2006 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15.5 1.3 15.9 1.5 15.0 1.5
2007–2008 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16.8 1.3 17.7 1.4 15.9 1.5
2009–2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16.9 0.7 18.6 1.1 15.0 0.8
2011–2012 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16.9 1.0 16.7 1.4 17.2 1.2
2013–2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17.2 1.1 17.2 1.3 17.1 1.6
2015–2016 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18.5 1.3 19.1 1.7 17.8 1.2
Obesity among adults aged 20 and over, by sex: 1999–2000 through 2015–2016
Year
Total Men Women
Percent SE Percent SE Percent SE
1999–2000 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30.5 1.5 27.4 1.5 33.3 1.7
2001–2002 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30.5 1.2 27.6 1.0 33.1 1.6
2003–2004 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32.3 1.2 31.3 1.4 33.2 1.7
2005–2006 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34.4 1.4 33.4 2.0 35.4 1.5
2007–2008 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33.7 1.1 32.1 1.4 35.3 1.1
2009–2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35.7 0.9 35.6 1.8 35.7 0.9
2011–2012 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34.9 1.3 33.5 1.4 36.1 1.6
2013–2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37.8 0.9 35.5 1.0 40.1 1.3
2015–2016 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39.7 1.6 38.1 2.3 41.2 1.5
NOTES: SE is standard error. Data are for the civilian noninstitutionalized population. Body mass index (BMI) is based on measured weight and height. BMI equals weight in
kilograms divided by height in meters squared. Estimates exclude pregnant females. Data on both age and height were collected during a standardized physical examination
conducted in mobile examination centers. Height is measured without shoes. Child obesity estimates are not age adjusted. Obesity in youth is defined as BMI at or above the
sex- and age-specific 95th percentile of the 2000 CDC Growth Charts. For more information, see Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et
al. 2000 CDC Growth Charts for the United States: Methods and development. Vital Health Stat 11(246). 2002. Available from: https://www.cdc.gov/nchs/data/series/sr_11/
sr11_246.pdf. For youth estimates, the NHANES variable Body Mass Index is used to assign persons to BMI categories. Age of youth (in months) is collected at the time of
examination. Adult obesity estimates are age adjusted to the year 2000 standard population using five age groups: 20–34, 35–44, 45–54, 55–64, and 65 and over. Age-adjusted
estimates in this table may differ from other age-adjusted estimates based on the same data and presented elsewhere if different age groups are used in the adjustment
procedure. Obesity in adulthood is defined as BMI greater than or equal to 30.0. For adult estimates, the NHANES variable Body Mass Index is rounded to one decimal place
then used to assign persons to BMI categories. Age of adults (in years) is collected at the time of screening. Data for additional years are available. See the Excel spreadsheet on
the Health, United States website at: https://www.cdc.gov/nchs/hus.htm. See Appendix II, Body mass index (BMI).
SOURCE: NCHS, National Health and Nutrition Examination Survey. See Appendix I, National Health and Nutrition Examination Survey (NHANES).

38 Health, United States, 2018
Data table for Figure 9. Current asthma among children under age 18 years, by race and Hispanic origin: United States,
2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_009
Year
Total
1
Race and Hispanic origin
Hispanic
Not Hispanic or Latino
White only Black only
Percent SE Percent SE Percent SE Percent SE
2007 . . . . . . . . . . . . . . . . . . . . . . 9.1 0.4 9.3 0.7 7.3 0.5 15.4 1.1
2008 . . . . . . . . . . . . . . . . . . . . . . 9.4 0.4 6.7 0.6 8.8 0.5 15.7 1.2
2009 . . . . . . . . . . . . . . . . . . . . . . 9.6 0.4 7.7 0.6 8.5 0.5 17.0 1.3
2010 . . . . . . . . . . . . . . . . . . . . . . 9.4 0.3 8.1 0.6 8.2 0.5 15.9 1.0
2011 . . . . . . . . . . . . . . . . . . . . . . 9.5 0.3 9.6 0.6 7.8 0.4 16.3 1.1
2012 . . . . . . . . . . . . . . . . . . . . . . 9.3 0.3 8.8 0.6 7.9 0.4 16.0 1.0
2013 . . . . . . . . . . . . . . . . . . . . . . 8.3 0.3 7.4 0.5 7.5 0.5 13.4 0.9
2014 . . . . . . . . . . . . . . . . . . . . . . 8.6 0.3 8.5 0.6 7.6 0.5 13.4 1.0
2015 . . . . . . . . . . . . . . . . . . . . . . 8.4 0.3 8.0 0.5 7.4 0.5 13.4 1.0
2016 . . . . . . . . . . . . . . . . . . . . . . 8.3 0.3 6.7 0.6 7.1 0.4 15.7 1.3
2017 . . . . . . . . . . . . . . . . . . . . . . 8.4 0.4 7.7 0.7 7.7 0.5 12.6 1.3
1
Includes all other races not shown separately.
NOTES: SE is standard error. Data are for the civilian noninstitutionalized population. Based on parent or knowledgeable adult responding yes to both questions, “Has a doctor
or other health professional ever told you that your child had asthma?” and “Does your child still have asthma?” Adults of Hispanic origin may be of any race. Race-specific
estimates are tabulated according to the 1997 Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity. The single-race categories plus multiple-
race category shown in the table conform to the 1997 Standards. Starting with 2003 data, race responses of other race and unspecified multiple race were treated as missing,
and then race was imputed if these were the only race responses. Almost all persons with a race response of other race were of Hispanic origin. See Appendix II, Hispanic origin;
Race.
SOURCE: NCHS, National Health Interview Survey. See Appendix I, National Health Interview Survey (NHIS).

Health, United States, 2018 39
Data table for Figure 10. Diabetes prevalence among adults aged 20 and over, by diagnosis status and age, United States,
1999–2000 through 2015–2016
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_010
Year
Age adjusted
1
Crude
Total
diabetes
Physician-
diagnosed
diabetes
2
Undiagnosed
diabetes
3
Total
diabetes
Physician-
diagnosed
diabetes
2
Undiagnosed
diabetes
3
Percent of adults
1999–2000 . . . . . . . . . . . . . . . . . . . . . . . 10.0 6.2 3.8 9.6 5.9 3.6
2001–2002 . . . . . . . . . . . . . . . . . . . . . . . 11.6 6.9 4.7 11.2 6.7 4.5
2003–2004 . . . . . . . . . . . . . . . . . . . . . . . 11.8 7.8 4.0 11.8 7.8 4.0
2005–2006 . . . . . . . . . . . . . . . . . . . . . . . 11.5 7.5 4.0 11.9 7.9 4.0
2007–2008 . . . . . . . . . . . . . . . . . . . . . . . 12.6 8.2 4.4 13.0 8.6 4.5
2009–2010 . . . . . . . . . . . . . . . . . . . . . . . 12.5 8.0 4.5 13.2 8.5 4.7
2011–2012 . . . . . . . . . . . . . . . . . . . . . . . 12.7 8.7 3.9 13.4 9.2 4.1
2013–2014 . . . . . . . . . . . . . . . . . . . . . . . 13.1 9.3 3.8 14.0 10.0 4.0
2015–2016 . . . . . . . . . . . . . . . . . . . . . . . 14.7 10.0 4.7 16.0 11.0 5.0
Standard error
1999–2000 . . . . . . . . . . . . . . . . . . . . . . . 1.1 1.0 0.5 1.1 0.9 0.6
2001–2002 . . . . . . . . . . . . . . . . . . . . . . . 0.9 0.7 0.4 0.9 0.7 0.4
2003–2004 . . . . . . . . . . . . . . . . . . . . . . . 1.0 0.7 0.6 0.9 0.8 0.6
2005–2006 . . . . . . . . . . . . . . . . . . . . . . . 0.9 0.7 0.6 1.1 0.7 0.7
2007–2008 . . . . . . . . . . . . . . . . . . . . . . . 0.8 0.6 0.4 0.8 0.7 0.4
2009–2010 . . . . . . . . . . . . . . . . . . . . . . . 1.0 0.8 0.4 1.0 0.8 0.4
2011–2012 . . . . . . . . . . . . . . . . . . . . . . . 1.1 0.9 0.6 1.3 1.1 0.6
2013–2014 . . . . . . . . . . . . . . . . . . . . . . . 0.8 0.7 0.3 1.0 0.9 0.4
2015–2016 . . . . . . . . . . . . . . . . . . . . . . . 1.0 0.8 0.7 1.1 0.9 0.7
Age
1999–2000 2015–2016
Total
diabetes
Physician-
diagnosed
diabetes
2
Undiagnosed
diabetes
3
Total
diabetes
Physician-
diagnosed
diabetes
2
Undiagnosed
diabetes
3
Percent of adults
20–44 years . . . . . . . . . . . . . . . . . . . . . . 4.3 2.7 1.6 5.6 3.2 2.4
45–64 years . . . . . . . . . . . . . . . . . . . . . . 14.7 8.3 6.3 21.9 14.9 7.0
65 years and over . . . . . . . . . . . . . . . . . 17.9 12.5 *5.4 28.2 21.1 7.1
Standard error
20–44 years . . . . . . . . . . . . . . . . . . . . . . 1.0 0.8 0.9 1.0 0.6 0.6
45–64 years . . . . . . . . . . . . . . . . . . . . . . 1.6 1.5 0.9 2.2 1.6 1.6
65 years and over . . . . . . . . . . . . . . . . . 3.1 2.6 *1.6 2.0 2.2 1.0
* Estimate is considered unreliable based on the multistep National Center for Health Statistics data presentation standards for proportions. The absolute confidence interval
width of the estimate is 0.05–0.30 and the relative confidence interval width is greater than 130%. The estimate has undergone statistical review. For more information see:
Parker JD, Talih M, Malec DJ, Beresovsky V, Carroll M, Gonzalez Jr JF, et al. National Center for Health Statistics Data Presentation Standards for Proportions. National Center for
Health Statistics. Vital Health Stat 2(175). 2017. Also see Appendix II, Data presentation standards for proportions.
1
Estimates are age adjusted to the year 2000 standard population using three age groups: 20–44, 45–64, and 65 and over. Age-adjusted estimates in this table may differ from
other age-adjusted estimates based on the same data and presented elsewhere if different age groups are used in the adjustment procedure. See Appendix II, Age adjustment.
2
Physician-diagnosed diabetes was obtained by self-report and excludes women who reported having diabetes during pregnancy.
3
Undiagnosed diabetes is defined as a fasting plasma glucose (FPG) of at least 126 mg/dL or a hemoglobin A1c of at least 6.5% and no reported physician diagnosis. Pregnant
females are excluded. Participants had fasted for at least 8 hours and less than 24 hours. Periodically, the location of and instruments used in laboratory testing changed
from previous years. In these instances, the National Health and Nutrition Examination Survey (NHANES) conducted crossover studies to evaluate their impact on laboratory
measurements, including measurements of FPG and A1c. Based on their studies, NHANES recommended adjustments to the FPG data. The forward adjustment method was
incorporated into the data presented here. For more information, see the 2015–2016 documentation (https://wwwn.cdc.gov/Nchs/Nhanes/2015-2016/GLU_I.htm), the 2007–
2008 documentation (https://wwwn.cdc.gov/Nchs/Nhanes/2007-2008/GLU_E.htm), and the 2005–2006 documentation (https://wwwn.cdc.gov/nchs/nhanes/2005-2006/
GLU_D.htm). See Appendix II, Diabetes.
NOTES: Data are for the civilian noninstitutionalized population. Excludes pregnant women. Fasting weights were used to obtain estimates of total, physician-diagnosed,
and undiagnosed diabetes prevalence. Estimates in this figure may differ from other estimates based on the same data and presented elsewhere if different weights, age
adjustment groups, definitions, or trend adjustments are used. See Appendix II, Diabetes.
SOURCE: NCHS, National Health and Nutrition Examination Survey. See Appendix I, National Health and Nutrition Examination Survey (NHANES).
ootnotes at end of table.

40 Health, United States, 2018
Data table for Figure 11. Hypertension and uncontrolled high blood pressure among adults aged 20 and over, by sex and
age: United States, 1999–2000 through 2015–2016
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_011
Hypertension and high blood pressure among adults aged 20 and over, by sex: 1999–2000 through 2015–2016
Characteristic
1999–
2000
2001–
2002
2003–
2004
2005–
2006
2007–
2008
2009–
2010
2011–
2012
2013–
2014
2015–
2016
Hypertension
1
Percent
Age adjusted
2
Both sexes . . . . . . . . . . . . . . . . . . . 30.0 29.7 32.1 30.5 31.2 30.0 30.0 30.8 30.2
Men . . . . . . . . . . . . . . . . . . . . . . . 29.5 28.1 32.5 31.3 31.9 30.8 30.3 31.7 31.3
Women . . . . . . . . . . . . . . . . . . . . 30.2 30.7 31.2 29.4 30.3 29.0 29.6 29.8 28.7
Standard error
Both sexes . . . . . . . . . . . . . . . . . . . 1.4 1.0 1.0 1.2 0.7 0.8 0.7 0.8 1.1
Men . . . . . . . . . . . . . . . . . . . . . . . 2.2 1.3 1.5 1.5 0.9 1.2 1.0 1.0 1.5
Women . . . . . . . . . . . . . . . . . . . . 1.0 1.0 1.2 1.0 0.8 0.9 1.0 1.1 1.2
Crude Percent
Both sexes . . . . . . . . . . . . . . . . . . . 28.9 28.9 32.5 31.7 32.6 31.9 32.5 33.5 33.2
Men . . . . . . . . . . . . . . . . . . . . . . . 27.5 26.3 31.6 30.9 31.9 31.5 31.8 33.3 32.9
Women . . . . . . . . . . . . . . . . . . . . 30.3 31.5 33.4 32.4 33.1 32.4 33.2 33.7 33.5
Standard error
Both sexes . . . . . . . . . . . . . . . . . . . 1.5 1.3 1.3 1.2 0.9 1.3 1.5 1.0 1.3
Men . . . . . . . . . . . . . . . . . . . . . . . 2.0 1.5 1.6 1.4 1.1 1.6 2.0 0.8 1.6
Women . . . . . . . . . . . . . . . . . . . . 1.6 1.4 1.5 1.3 1.3 1.3 1.3 1.5 1.3
High blood pressure
3
Percent
Age adjusted
2
Both sexes . . . . . . . . . . . . . . . . . . . 20.6 19.1 18.9 17.1 15.9 13.9 14.4 14.1 15.6
Men . . . . . . . . . . . . . . . . . . . . . . . 19.6 18.3 18.4 18.1 16.9 15.4 15.1 15.6 17.5
Women . . . . . . . . . . . . . . . . . . . . 21.1 19.4 19.0 15.7 14.8 12.3 13.4 12.6 13.6
Standard error
Both sexes . . . . . . . . . . . . . . . . . . . 1.3 0.7 1.1 0.9 0.5 0.6 0.8 0.9 0.8
Men . . . . . . . . . . . . . . . . . . . . . . . 1.8 0.9 1.6 1.2 0.8 0.6 0.8 1.3 1.2
Women . . . . . . . . . . . . . . . . . . . . 1.1 0.8 0.9 0.7 0.5 0.8 1.1 0.8 0.9
Crude Percent
Both sexes . . . . . . . . . . . . . . . . . . . 19.7 18.5 19.0 17.5 16.4 14.6 15.3 15.1 16.9
Men . . . . . . . . . . . . . . . . . . . . . . . 18.2 17.3 17.9 17.8 16.7 15.7 15.9 16.2 17.9
Women . . . . . . . . . . . . . . . . . . . . 21.1 19.7 20.0 17.2 16.2 13.5 14.8 14.1 16.0
Standard error
Both sexes . . . . . . . . . . . . . . . . . . . 1.3 0.8 1.3 0.8 0.4 0.6 0.9 0.9 0.9
Men . . . . . . . . . . . . . . . . . . . . . . . 1.6 0.9 1.7 1.1 0.6 0.6 1.0 1.3 1.2
Women . . . . . . . . . . . . . . . . . . . . 1.4 1.0 1.0 0.9 0.6 0.8 1.1 0.9 1.0
See footnotes at end of table.

Health, United States, 2018 41
Data table for Figure 11. Hypertension and uncontrolled high blood pressure among adults aged 20 and over, by sex and
age: United States, 1999–2000 through 2015–2016—Con.
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_011
Uncontrolled high blood pressure among those with hypertension, by sex and age: 2015–2016
Sex and age (years) Percent Standard error
Total
4
20–44 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59.8 3.1
45–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46.3 2.8
65 and over . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.2 3.1
Men
4
20–44 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 73.1 2.9
45–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50.1 4.0
65 and over . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.7 2.8
Women
4
20–44 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37.9 5.0
45–64 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42.1 3.4
65 and over . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.8 4.0
1
Hypertension is defined as having measured high blood pressure or currently taking antihypertensive medication. High blood pressure is defined as having measured systolic
pressure of greater than or equal to 140 mm Hg or diastolic pressure of greater than or equal to 90 mm Hg. Estimates exclude pregnant females. Those with high blood pressure
may also currently be taking antihypertensive medication for high blood pressure. Those currently taking antihypertensive medication may not have measured high blood
pressure but are still classified as having hypertension.
2
Estimates are age adjusted to the year 2000 standard population using five age groups: 20‒34, 35‒44, 45‒54, 55‒64, and 65 and over. See Appendix II, Age adjustment.
3
High blood pressure is defined as having measured systolic pressure of greater than or equal to 140 mm Hg or diastolic pressure of greater than or equal to 90 mm Hg.
Estimates exclude pregnant females. Those with high blood pressure may also currently be taking antihypertensive medication for high blood pressure.
4
Estimates are limited to those with hypertension. Hypertension is defined as having measured high blood pressure, currently taking antihypertensive medication, or both. High
blood pressure is defined as having measured systolic pressure of greater than or equal to 140 mm Hg or diastolic pressure of greater than or equal to 90 mm Hg. Uncontrolled
high blood pressure is high blood pressure among those with hypertension. Estimates exclude pregnant females. Those with high blood pressure may also currently be taking
antihypertensive medication for high blood pressure. Those currently taking antihypertensive medication may not have measured high blood pressure but are still classified as
having hypertension.
NOTES: Data are for the civilian noninstitutionalized population. In 2017, a revised set of practice guidelines for defining high blood pressure was released but has not been
widely adopted. Therefore, the high blood pressure cutoffs used to define hypertension and uncontrolled high blood pressure in Health, United States continue to use the
original definition of having measured systolic pressure of greater than or equal to 140 mm Hg or diastolic pressure of greater than or equal to 90 mm Hg. For more information,
including a comparison of high blood pressure estimates based on the current and revised definitions, see Appendix II, Hypertension; Table VI.
SOURCE: NCHS, National Health and Nutrition Examination Survey. See Appendix I, National Health and Nutrition Examination Survey (NHANES).

42 Health, United States, 2018
Data table for Figure 12. Functional limitation among adults aged 18 and over, by age and level of difficulty: United States,
2010–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_012
Functional limitation among adults aged 18-64, by level of difficulty: 2010–2017
Year
Level of difficulty
No difficulty Some difficulty A lot of difficulty or cannot do at all
Crude Age adjusted Crude Age adjusted Crude Age adjusted
Percent
2010 . . . . . . . . . . . . . . . . . . . . . . . . 67.2 68.2 26.7 26.1 6.2 5.7
2011 . . . . . . . . . . . . . . . . . . . . . . . . 72.5 73.6 21.5 20.9 6.0 5.5
2012 . . . . . . . . . . . . . . . . . . . . . . . . 66.1 67.6 28.2 27.1 5.7 5.3
2013 . . . . . . . . . . . . . . . . . . . . . . . . 63.5 64.9 29.7 28.9 6.8 6.2
2014 . . . . . . . . . . . . . . . . . . . . . . . . 63.9 65.2 28.9 28.1 7.2 6.7
2015 . . . . . . . . . . . . . . . . . . . . . . . . 67.3 68.7 26.1 25.1 6.6 6.1
2016 . . . . . . . . . . . . . . . . . . . . . . . . 67.3 68.3 26.5 25.9 6.2 5.8
2017 . . . . . . . . . . . . . . . . . . . . . . . . 66.3 67.6 27.8 26.9 5.9 5.5
Standard error
2010 . . . . . . . . . . . . . . . . . . . . . . . . 0.8 0.8 0.8 0.8 0.4 0.4
2011 . . . . . . . . . . . . . . . . . . . . . . . . 0.5 0.5 0.4 0.4 0.2 0.3
2012 . . . . . . . . . . . . . . . . . . . . . . . . 0.8 0.8 0.7 0.7 0.4 0.4
2013 . . . . . . . . . . . . . . . . . . . . . . . . 0.6 0.6 0.5 0.6 0.3 0.3
2014 . . . . . . . . . . . . . . . . . . . . . . . . 0.6 0.6 0.6 0.6 0.3 0.3
2015 . . . . . . . . . . . . . . . . . . . . . . . . 0.6 0.6 0.6 0.6 0.3 0.3
2016 . . . . . . . . . . . . . . . . . . . . . . . . 0.7 0.7 0.6 0.6 0.3 0.3
2017 . . . . . . . . . . . . . . . . . . . . . . . . 0.7 0.6 0.6 0.6 0.3 0.3
Functional limitation among adults aged 65 and over, by level of difficulty: 2010–2017
Year
Level of difficulty
No difficulty Some difficulty A lot of difficulty or cannot do at all
Crude Age adjusted Crude Age adjusted Crude Age adjusted
Percent
2010 . . . . . . . . . . . . . . . . . . . . . . . . 35.4 35.0 42.0 42.0 22.6 23.1
2011 . . . . . . . . . . . . . . . . . . . . . . . . 40.3 39.8 39.1 39.3 20.7 21.0
2012 . . . . . . . . . . . . . . . . . . . . . . . . 40.4 39.7 41.7 41.9 17.9 18.5
2013 . . . . . . . . . . . . . . . . . . . . . . . . 33.8 32.7 44.3 44.6 21.9 22.7
2014 . . . . . . . . . . . . . . . . . . . . . . . . 33.6 32.6 44.7 45.0 21.6 22.3
2015 . . . . . . . . . . . . . . . . . . . . . . . . 36.1 34.5 42.4 42.8 21.6 22.7
2016 . . . . . . . . . . . . . . . . . . . . . . . . 39.9 38.6 42.0 42.2 18.2 19.2
2017 . . . . . . . . . . . . . . . . . . . . . . . . 38.9 37.7 41.6 41.8 19.5 20.6
Standard error
2010 . . . . . . . . . . . . . . . . . . . . . . . . 1.7 1.6 1.7 1.7 1.4 1.4
2011 . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.0 1.0 1.0 0.9 0.9
2012 . . . . . . . . . . . . . . . . . . . . . . . . 1.5 1.5 1.4 1.4 1.1 1.1
2013 . . . . . . . . . . . . . . . . . . . . . . . . 1.0 0.9 1.1 1.1 0.9 0.9
2014 . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.0 1.0 1.0 0.9 0.9
2015 . . . . . . . . . . . . . . . . . . . . . . . . 1.1 1.0 1.1 1.1 0.9 1.0
2016 . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.0 1.0 1.0 0.7 0.7
2017 . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.0 1.0 1.0 0.8 0.9
NOTES: Data are for the civilian noninstitutionalized population. Functional limitation is defined by the reported level of difficulty in six functioning domains: seeing (even
if wearing glasses), hearing (even if wearing hearing aids), mobility (walking or climbing stairs), communication (understanding or being understood by others), cognition
(remembering or concentrating), and self-care (such as washing all over or dressing). Respondents with answers to one or more of the six questions were included in one of
three mutually exclusive categories. Those responding “A lot of difficulty” or “Cannot do at all/unable to do” to at least one question were classified in the “A lot of difficulty/
cannot do at all” category. Of the remaining, those responding “Some difficulty” to at least one question were classified in the “Some difficulty” category, and those responding
“No difficulty” to at least one question were classified in the “No difficulty” category. Those responding “Don’t know” or “Refused” to all six questions were excluded. During
2010–2017, 1%–8% of respondents were missing data and excluded. Estimates are age adjusted to the year 2000 standard population using five age groups: 18–44 years, 45–54
years, and 55–64 years for the 18–64 estimates and 65–74 years and 75 years and over for the 65 years and over estimates. Estimates may not sum to total percentage due to
rounding. See Appendix II, Age adjustment; Functional limitation.
SOURCE: NCHS, National Health Interview Survey. See Appendix I, National Health Interview Survey (NHIS).

Health, United States, 2018 43
Data table for Figure 13. Vaccination coverage for combined series (4:3:1:3*:3:1:4) among children aged 19–35 months, by
selected characteristics: United States, 2010 and 2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_013
Characteristic
2010 2017
Percent Standard error Percent Standard error
Total . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56.6 0.7 70.4 0.8
Race and Hispanic origin
White, not Hispanic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56.9 0.8 71.5 0.9
Black, not Hispanic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.5 1.8 66.5 2.2
Asian, not Hispanic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59.3 3.7 72.4 3.4
American Indian or Alaska Native, not Hispanic . . . . . . . . . . . . . . . . . . . 64.1 4.7 65.9 5.1
Hispanic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.5 1.6 70.4 1.8
Metropolitan statistical area (MSA)
Non-MSA . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.2 1.5 66.8 1.6
MSA, nonprincipal city . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57.7 1.1 69.8 1.2
MSA, principal city . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56.1 1.1 71.9 1.1
Health insurance coverage
Uninsured . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41.0 3.6 48.5 3.7
Medicaid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.6 1.1 66.5 1.2
Private . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.0 0.8 76.0 1.0
NOTES: Data are for the civilian noninstitutionalized population. The combined 7-vaccine series consists of 4 or more doses of either the diphtheria, tetanus toxoids, and
pertussis vaccine (DTP), the diphtheria and tetanus toxoids vaccine (DT), or the diphtheria, tetanus toxoids, and acellular pertussis vaccine (DTaP); 3 or more doses of any
poliovirus vaccine; 1 or more doses of a measles-containing vaccine (MCV); 3 or more doses or 4 or more doses of Haemophilus influenzae type b vaccine (Hib) depending on
Hib vaccine product type (full series Hib); 3 or more doses of hepatitis B vaccine; 1 or more doses of varicella vaccine; and 4 or more doses of pneumococcal conjugate vaccine
(PCV). Persons of Hispanic origin may be of any race. Starting with 2000 data, estimates were tabulated using the 1997 Revisions to the Standards for the Classification of Federal
Data on Race and Ethnicity. MSA status was grouped into three categories: MSA principal city, MSA non-principal city, and non-MSA. MSA and principal city were as defined
by the U.S. Census Bureau (https://www.census.gov/geo/reference/gtc/gtc_cbsa.html). Data from U.S. territories were not included in the national estimates. See Appendix II,
Vaccination.
SOURCE: National Center for Immunization and Respiratory Diseases (NCIRD), National Immunization Survey-Child (NIS-Child). See Appendix I, National Immunization Surveys
(NIS).

44 Health, United States, 2018
Data table for Figure 14. Prescription drug use in the past 30 days, by number of drugs taken and age: United States,
1999‒2000 through 2015‒2016
Excel and PowerPoint: http://www.cdc.gov/nchs/hus/contents2018.htm#Figure_014
Prescription drug use in the past 30 days, by number of drugs taken: 1999–2000 through 2015–2016
Number of prescription
drugs in the past 30 days
1999‒
2000
2001‒
2002
2003‒
2004
2005‒
2006
2007‒
2008
2009‒
2010
2011‒
2012
2013‒
2014
2015‒
2016
All ages, crude Percent
No drugs . . . . . . . . . . . . . . . . . . . . . . . . . 57.2 54.6 52.4 53.0 51.2 51.9 50.7 51.4 51.9
1‒4 drugs . . . . . . . . . . . . . . . . . . . . . . . . 36.8 37.6 37.4 36.8 37.9 37.8 38.2 35.9 35.6
5 or more drugs . . . . . . . . . . . . . . . . . . . 6.1 7.9 10.1 10.2 10.9 10.3 11.1 12.6 12.5
All ages, age adjusted
1
No drugs . . . . . . . . . . . . . . . . . . . . . . . . . 56.0 53.9 52.7 53.6 52.1 53.0 52.4 53.7 54.7
1–4 drugs . . . . . . . . . . . . . . . . . . . . . . . . 37.5 37.9 37.3 36.5 37.4 37.3 37.2 34.8 34.4
5 or more drugs . . . . . . . . . . . . . . . . . . . 6.5 8.3 10.0 9.9 10.5 9.8 10.4 11.5 11.0
All ages, crude Standard error
No drugs . . . . . . . . . . . . . . . . . . . . . . . . . 1.1 1.9 1.1 1.1 0.9 1.5 1.4 0.8 1.0
1‒4 drugs . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.6 0.7 0.6 0.6 1.2 1.0 0.8 1.0
5 or more drugs . . . . . . . . . . . . . . . . . . . 0.3 0.5 0.7 0.6 0.9 0.5 0.8 0.7 0.6
All ages, age adjusted
1
No drugs . . . . . . . . . . . . . . . . . . . . . . . . . 1.0 1.4 0.9 0.7 0.8 1.2 1.0 0.6 0.8
1‒4 drugs . . . . . . . . . . . . . . . . . . . . . . . . 0.9 1.3 0.7 0.5 0.7 1.0 0.9 0.8 0.8
5 or more drugs . . . . . . . . . . . . . . . . . . . 0.3 0.5 0.5 0.3 0.7 0.4 0.5 0.6 0.5
Prescription drug use in the past 30 days, by age and number of drugs taken in the past 30 days: 2015‒2016
Number of prescription
drugs in the past 30 days
Under 18 18‒44 45‒64 65 and over
Percent SE Percent SE Percent SE Percent SE
No drugs . . . . . . . . . . . . . . . . . . . . . . . . . 79.0 1.0 64.7 1.5 32.6 1.8 12.5 1.2
At least one drug . . . . . . . . . . . . . . . . . . 21.0 1.0 35.3 1.5 67.4 1.8 87.5 1.2
1–4 drugs . . . . . . . . . . . . . . . . . . . . . . . . 20.3 0.9 31.4 1.3 48.3 2.7 47.7 2.3
5 or more drugs . . . . . . . . . . . . . . . . . . . 0.7 0.3 3.9 0.4 19.1 1.4 39.8 2.0
1
Estimates are age adjusted to the year 2000 standard population using four age groups: under 18, 18‒44, 45‒64, and 65 and over. See Appendix II, Age adjustment.
NOTES: SE is standard error. Data are for the civilian noninstitutionalized population. Prescription drug use in the past 30 days is respondent-reported. Prescriptions
administered in other health care settings, such as physician offices and hospital outpatient departments, are not collected. See Appendix II, Drug.
SOURCE: NCHS, National Health and Nutrition Examination Survey. See Appendix I, National Health and Nutrition Examination Survey (NHANES).

Health, United States, 2018 45
Data table for Figure 15. Delay or nonreceipt of needed medical care and nonreceipt of needed prescription drugs in the
past 12 months due to cost among adults aged 18–64, by percent of poverty level: United States, 2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_015
Delay or nonreceipt of needed medical care due to cost among adults aged 18–64
Year
Percent of poverty level
Below 100% 100%–199% 200%–399% At or above 400%
Percent SE Percent SE Percent SE Percent SE
2007 . . . . . . . . . . . . . . . . 20.8 0.8 19.9 0.6 13.0 0.4 5.3 0.2
2008 . . . . . . . . . . . . . . . . 21.9 0.8 22.5 0.7 15.0 0.5 6.7 0.3
2009 . . . . . . . . . . . . . . . . 24.8 0.8 24.0 0.6 16.8 0.5 7.2 0.3
2010 . . . . . . . . . . . . . . . . 23.4 0.7 24.0 0.6 15.2 0.4 6.8 0.2
2011 . . . . . . . . . . . . . . . . 24.1 0.7 23.5 0.6 14.2 0.4 5.5 0.2
2012 . . . . . . . . . . . . . . . . 22.4 0.6 22.3 0.5 13.2 0.3 5.3 0.2
2013 . . . . . . . . . . . . . . . . 21.8 0.6 20.3 0.6 12.5 0.3 5.1 0.2
2014 . . . . . . . . . . . . . . . . 20.2 0.6 17.9 0.5 11.5 0.4 4.3 0.2
2015 . . . . . . . . . . . . . . . . 16.6 0.6 15.9 0.5 10.8 0.4 4.2 0.2
2016 . . . . . . . . . . . . . . . . 15.2 0.6 16.3 0.5 10.6 0.4 4.9 0.2
2017 . . . . . . . . . . . . . . . . 16.2 0.6 15.3 0.5 11.6 0.4 5.1 0.2
Nonreceipt of needed prescription drugs due to cost among adults aged 18–64
Year
Percent of poverty level
Below 100% 100%–199% 200%–399% At or above 400%
Percent SE Percent SE Percent SE Percent SE
2007 . . . . . . . . . . . . . . . . 18.8 1.0 17.2 0.8 10.6 0.6 3.0 0.3
2008 . . . . . . . . . . . . . . . . 19.6 1.1 20.4 0.9 10.7 0.5 4.3 0.3
2009 . . . . . . . . . . . . . . . . 20.5 1.0 18.8 1.0 12.2 0.6 4.1 0.3
2010 . . . . . . . . . . . . . . . . 21.5 0.8 18.4 0.8 11.4 0.5 3.9 0.3
2011 . . . . . . . . . . . . . . . . 20.2 0.8 17.9 0.7 10.6 0.5 3.2 0.2
2012 . . . . . . . . . . . . . . . . 19.4 0.8 15.7 0.7 8.4 0.4 2.9 0.2
2013 . . . . . . . . . . . . . . . . 18.3 0.8 14.4 0.7 8.4 0.4 2.8 0.2
2014 . . . . . . . . . . . . . . . . 16.1 0.8 12.5 0.8 7.0 0.5 2.5 0.3
2015 . . . . . . . . . . . . . . . . 12.9 0.7 12.7 0.7 7.0 0.4 2.3 0.2
2016 . . . . . . . . . . . . . . . . 12.7 0.7 11.7 0.7 7.2 0.5 2.3 0.2
2017 . . . . . . . . . . . . . . . . 11.9 0.7 11.6 0.7 7.0 0.4 2.7 0.3
NOTES: SE is standard error. Data are for the civilian noninstitutionalized population. Delay or nonreceipt of needed medical care was based on responses to the questions,
“During the past 12 months was there any time when person needed medical care but did not get it because person couldn’t afford it?” and “During the past 12 months has
medical care been delayed because of worry about the cost?” Percent of poverty level is based on family income and family size and composition using U.S. Census Bureau
poverty thresholds. Missing family income data were imputed for 1997 and beyond. See Appendix II, Family income; Poverty; Table VII.
SOURCE: NCHS, National Health Interview Survey. See Appendix I, National Health Interview Survey (NHIS).

46 Health, United States, 2018
Data table for Figure 16. Number of dentists per 100,000 resident population, by state: United States, 2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_016
State
Number per
100,000 State
Number per
100,000
United States . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60.95 Missouri . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48.52
Alabama . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40.43 Montana . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.11
Alaska . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79.48 Nebraska . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64.16
Arizona . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.10 Nevada . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.07
Arkansas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41.67 New Hampshire . . . . . . . . . . . . . . . . . . . . . . . . . . 63.60
California . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77.49 New Jersey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 77.63
Colorado . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70.52 New Mexico . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.12
Connecticut . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74.38 New York . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74.45
Delaware . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44.08 North Carolina . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.37
District of Columbia . . . . . . . . . . . . . . . . . . . . . . 103.89 North Dakota . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57.85
Florida . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 51.54 Ohio . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52.69
Georgia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47.18 Oklahoma . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49.96
Hawaii . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 75.79 Oregon . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67.78
Idaho . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.28 Pennsylvania . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60.32
Illinois . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68.19 Rhode Island . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.64
Indiana . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47.71 South Carolina . . . . . . . . . . . . . . . . . . . . . . . . . . . 48.32
Iowa . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.04 South Dakota . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.47
Kansas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49.71 Tennessee . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49.43
Kentucky . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.77 Texas . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52.70
Louisiana . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48.54 Utah . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.22
Maine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52.47 Vermont . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57.88
Maryland . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70.40 Virginia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62.54
Massachusetts . . . . . . . . . . . . . . . . . . . . . . . . . . . 82.66 Washington . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70.88
Michigan . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61.16 West Virginia . . . . . . . . . . . . . . . . . . . . . . . . . . . . 47.86
Minnesota . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58.53 Wisconsin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58.20
Mississippi . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42.86 Wyoming . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.41
NOTES: Data on the number of dentists per 100,000 resident population are calculated using 2010-based postcensal estimates. Data include professionally active dentists only:
those whose primary occupation is private practice (full- or part-time), dental school/faculty staff member, armed forces, other federal services (i.e., Veterans’ Affairs, Public
Health Service), state or local government employee, hospital staff dentist, graduate student/intern/resident, or other health/dental organization staff member. Data for the
map are displayed by a modified Jenks classification for the 50 U.S. states and D.C., which creates categories that minimize within-group variation and maximize between-group
variation.
SOURCE: American Dental Association, Health Policy Institute. Supply of Dentists in the US: 2001–2017. (Copyright 2017 American Dental Association. Reprinted with
permission. All rights reserved.)

Health, United States, 2018 47
Data table for Figure 17. Use of long-term care services, by type of service and age: United States, 2011–2012 and
2015–2016
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_017
Use of long-term care services among adults aged 65 and over, by type of service: 2011–2012 and 2015–2016
Type of service 2011–2012 2015–2016 2011–2012 2015–2016
Number of users Standard error
Home health agencies
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3,905,700 3,651,400 92,970 88,018
Hospices
2
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,175,700 1,347,600 36,212 41,041
Nursing homes
3
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,123,800 1,166,400 5,917 6,021
Residential care communities
4
. . . . . . . . . . . . . . . . . . . . . . . . 665,800 757,900 9,065 8,301
Adult day services centers
5
. . . . . . . . . . . . . . . . . . . . . . . . . . . 173,400 179,200 2,438 2,859
Use of long-term care services, by age and type of service: 2015–2016
Type of service Under age 65 65–84 85 and over All ages
Percent distribution
Home health agencies
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18.1 56.7 25.2 100.0
Hospices
2
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.5 46.7 47.8 100.0
Nursing homes
3
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16.5 44.9 38.6 100.0
Residential care communities
4
. . . . . . . . . . . . . . . . . . . . . . . . 6.6 41.3 52.1 100.0
Adult day services centers
5
. . . . . . . . . . . . . . . . . . . . . . . . . . . 37.4 46.3 16.3 100.0
Standard error
Home health agencies
1
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.2 0.1 0.2
Hospices
2
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.1 0.2 0.8
Nursing homes
3
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 0.1 0.1 0.2
Residential care communities
4
. . . . . . . . . . . . . . . . . . . . . . . . 0.3 0.6 0.7
Adult day services centers
5
. . . . . . . . . . . . . . . . . . . . . . . . . . . 0.6 0.4 0.3
1
Outcome-Based Quality Improvement data were merged with Certification And Survey Provider Enhanced Reports (CASPER). Estimates are for home health patients whose
episode of care ended anytime in 2015.
2
Institutional Provider and Beneficiary Summary data were merged with CASPER. Estimates are for hospice patients receiving care anytime in 2015.
3
Minimum Data Set Active Resident Episode Table data were merged with CASPER. Estimates are for nursing home services users on any given day in 2016.
4
Residential care communities include assisted living and similar facilities. Estimates are for users of the service on any given day in 2016.
5
Adult day services centers include facilities self-identified as adult day care, adult day services, or adult day health services centers. Estimates are for users of the service on
any given day in 2016.
NOTES: Denominators used to calculate percentages of use by age for adult day services centers, nursing homes, and residential care communities were the number of current
users for each type of service. For home health agency and hospices, denominators were the number of patients who received care from Medicare-certified facilities at any
time during the year. Percentages were based on the unrounded numbers. Number of users were rounded to the nearest 100. People may use more than one service per year,
and were counted in each service used. Statistical testing was conducted on unrounded estimates. Two main sources of data were used for the estimates: administrative data
from the Centers for Medicare & Medicaid Services (CMS) on nursing homes, home health agencies, and hospices; and cross-sectional, nationally representative, establishment-
based survey data from NCHS for assisted living and similar residential care communities and adult day services centers.
SOURCE: NCHS, National Study of Long-Term Care Providers. See Appendix I, National Study of Long-Term Care Providers (NSLTCP) .

48 Health, United States, 2018
Data table for Figure 18. Personal health care expenditures, by source of funds and type of expenditure: United States,
2007–2017
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_018
Personal health care expenditures, by source of funds: 2007–2017
Year
Personal
health care
expenditures
Source of funds
Private
health
insurance Medicare Medicaid (total)
Medicaid
(federal)
Medicaid
(state and local)
Out of
pocket
All other
sources of
funds
1
Amount in billions ($)
2007 . . . . . . . . . . . . . . . . . . . . . 1,918.4 671.4 408.7 301.1 171.9 129.3 290.0 247.2
2008 . . . . . . . . . . . . . . . . . . . . . 2,010.7 700.8 442.0 317.8 188.3 129.5 295.2 254.8
2009 . . . . . . . . . . . . . . . . . . . . . 2,114.6 734.7 470.3 346.2 230.6 115.6 293.8 269.6
2010 . . . . . . . . . . . . . . . . . . . . . 2,196.1 755.9 489.1 365.8 247.3 118.5 299.8 285.6
2011 . . . . . . . . . . . . . . . . . . . . . 2,274.1 787.1 512.1 373.9 228.2 145.7 310.0 291.1
2012 . . . . . . . . . . . . . . . . . . . . . 2,367.4 816.4 533.8 388.4 223.9 164.6 318.8 309.9
2013 . . . . . . . . . . . . . . . . . . . . . 2,438.0 831.3 554.6 405.9 234.4 171.5 325.9 320.4
2014 . . . . . . . . . . . . . . . . . . . . . 2,561.5 875.3 580.5 446.6 274.1 172.5 330.9 328.2
2015 . . . . . . . . . . . . . . . . . . . . . 2,717.8 944.2 607.3 484.1 304.5 179.7 340.9 341.2
2016 . . . . . . . . . . . . . . . . . . . . . 2,851.9 1,004.3 630.3 504.2 318.5 185.7 356.1 357.1
2017 . . . . . . . . . . . . . . . . . . . . . 2,961.0 1,039.8 660.0 521.3 323.1 198.2 365.5 374.4
Average annual percent change
2007–2017 . . . . . . . . . . . . . . . . 4.4 4.5 4.9 5.6 6.5 4.4 2.3 4.2
Personal health care expenditures, by type of expenditure: 2007 and 2017
Type of expenditure 2007 2017
Percent distribution
All types of expenditures . . . . . . . . . . . . . . . . . . 100.0 100.0
Hospital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36.1 38.6
Physician and clinical . . . . . . . . . . . . . . . . . . . . . 23.8 23.4
Prescription drugs . . . . . . . . . . . . . . . . . . . . . . . . 12.3 11.3
Dental . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.1 4.4
Nursing care facilities and
continuing care retirement communities . . . 6.5 5.6
Home health care . . . . . . . . . . . . . . . . . . . . . . . . 3.0 3.3
All other types of expenditures
2
. . . . . . . . . . . . 13.2 13.4
1
All other sources of funds include the Children’s Health Insurance Program (CHIP) including Medicaid CHIP expansions; other health insurance programs including Department
of Defense and Department of Veterans Affairs; and other third party payers and programs including worksite health care, other private revenues, Indian Health Service,
workers’ compensation, general assistance, maternal and child health, vocational rehabilitation, other federal programs, Substance Abuse and Mental Health Services
Administration, other state and local programs, and school health.
2
All other types of expenditures include other professional services; other health, residential, and personal care; and durable and other nondurable medical products.
NOTES: Personal health care expenditures are outlays for goods and services relating directly to patient care. Personal health care expenditures are in current dollars and are
not adjusted for inflation. Numbers may not add to totals because of rounding. See Appendix II, Health expenditures, national.
SOURCE: Centers for Medicare & Medicaid Services, National Health Expenditure Accounts. See Appendix I, National Health Expenditure Accounts (NHEA).
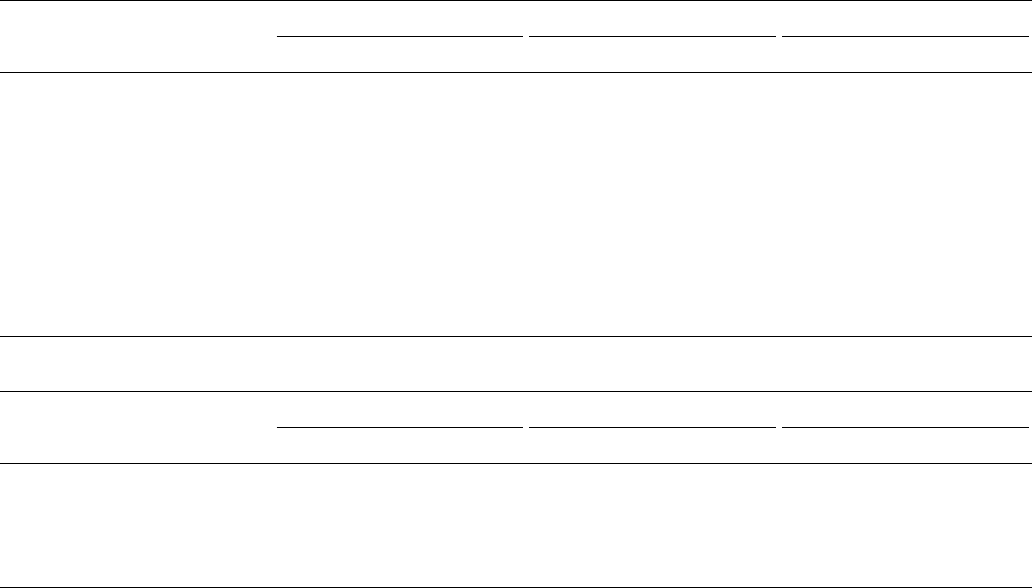
Health, United States, 2018 49
Data table for Figure 19. Health insurance coverage among children under age 18 years, by type of coverage and race and
Hispanic origin: United States, 2007–2018 (preliminary data)
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_019
Health insurance coverage, by type of coverage: 2007–2018
Year
Private
1
Medicaid
2
Uninsured
3
Percent SE Percent SE Percent SE
2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59.8 0.7 28.6 0.6 9.0 0.4
2008 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58.4 0.7 30.1 0.7 9.0 0.4
2009 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.8 0.8 33.1 0.7 8.2 0.4
2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.1 0.7 35.2 0.6 7.8 0.3
2011 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.7 0.7 37.0 0.7 7.0 0.3
2012 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.4 0.6 37.6 0.6 6.6 0.3
2013 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.2 0.7 37.7 0.6 6.6 0.3
2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.7 0.6 38.1 0.6 5.4 0.2
2015 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.6 0.7 38.7 0.7 4.5 0.2
2016 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.3 0.7 37.8 0.7 5.2 0.3
2017 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55.2 0.7 36.7 0.7 5.0 0.3
4
2018. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.7 0.8 36.0 0.8 5.2 0.3
Health insurance coverage, by race and ethnicity: 2017
Race and ethnicity
Private
1
Medicaid
2
Uninsured
3
Percent SE Percent SE Percent SE
Not Hispanic or Latino
White only . . . . . . . . . . . . . . . . . . . . . . . . 69.0 0.8 23.8 0.8 4.1 0.4
Black only . . . . . . . . . . . . . . . . . . . . . . . . . 36.3 1.8 56.1 1.9 4.0 0.8
Asian only . . . . . . . . . . . . . . . . . . . . . . . . . 70.8 2.6 23.6 2.4 3.8 0.8
Hispanic . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34.8 1.3 55.1 1.4 7.7 0.7
1
The private coverage category includes plans obtained through an employer, purchased directly, or purchased through the Health Insurance Marketplace or a state-based
exchange. The category excludes plans that paid for only one type of specialized service, such as accidents or dental care. Private health insurance includes managed care, such
as health maintenance organizations (HMOs).
2
The Medicaid coverage category includes children who had Medicaid or other state-sponsored health plans, including the Children’s Health Insurance Program (CHIP).
3
Children not covered by private insurance, Medicaid, CHIP, state-sponsored or other government-sponsored health plans (starting in 1997), Medicare, or military plans are
considered to have no health insurance coverage. Children with only Indian Health Service coverage are considered to have no health insurance coverage.
4
Preliminary data based on the National Health Interview Survey’s Early Release program. Estimates based on the preliminary file may differ from estimates based on the final
annual file and have larger standard errors associated with them than standard errors based on a final annual file. Available from: Cohen RA, Terlizzi EP, Martinez ME. Health
insurance coverage: Early release of estimates from the National Health Interview Survey, 2018. National Center for Health Statistics. May 2019. Available from: https://www.
cdc.gov/nchs/data/nhis/earlyrelease/insur201902.pdf and National Health Interview Survey, 2018 preliminary file. For more information, visit: https://www.cdc.gov/nchs/nhis.
htm.
NOTES: SE is standard error. Data are for the civilian noninstitutionalized population. Health insurance coverage is at the time of interview. Health insurance categories are
mutually exclusive. A small percentage of persons are covered by Medicare or other public plans, military plans, or other plans. Estimates for this group are not presented.
SOURCE: NCHS, National Health Interview Survey. See Appendix I, National Health Interview Survey (NHIS).

50 Health, United States, 2018
Data table for Figure 20. Health insurance coverage among adults aged 18–64, by type of coverage and race and Hispanic
origin: United States, 2007–2018 (preliminary data)
Excel and PowerPoint: https://www.cdc.gov/nchs/hus/contents2018.htm#Figure_20
Health insurance coverage, by type of coverage: 2007–2018
Year
Private
1
Medicaid
2
Uninsured
3
Percent SE Percent SE Percent SE
2007 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69.5 0.4 7.4 0.2 19.6 0.3
2008 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68.5 0.4 7.8 0.2 19.9 0.3
2009 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 66.2 0.4 8.6 0.2 21.2 0.3
2010 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64.7 0.4 9.0 0.2 22.3 0.3
2011 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65.0 0.4 9.5 0.2 21.2 0.3
2012 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65.1 0.4 9.8 0.2 20.9 0.3
2013 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65.1 0.4 10.0 0.2 20.5 0.3
2014 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67.4 0.4 11.8 0.2 16.3 0.3
2015 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69.7 0.4 12.9 0.3 13.0 0.2
2016 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69.9 0.4 13.6 0.3 12.2 0.3
2017 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69.6 0.4 13.2 0.3 12.8 0.3
4
2018. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68.9 0.5 12.8 0.3 13.3 0.4
Health insurance coverage, by race and ethnicity: 2017
Race and ethnicity
Private
1
Medicaid
2
Uninsured
3
Percent SE Percent SE Percent SE
Not Hispanic or Latino
White only . . . . . . . . . . . . . . . . . . . . . . . . 77.5 0.4 9.4 0.3 8.5 0.2
Black only . . . . . . . . . . . . . . . . . . . . . . . . . 57.5 1.0 22.3 0.9 14.0 0.6
Asian only . . . . . . . . . . . . . . . . . . . . . . . . . 77.6 1.3 12.2 1.0 7.4 0.7
Hispanic . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50.5 1.1 18.9 0.8 27.5 0.9
1
The private coverage category includes plans obtained through an employer, purchased directly, or purchased through the Health Insurance Marketplace or a state-based
exchange. The category excludes plans that paid for only one type of specialized service, such as accidents or dental care. Private health insurance includes managed care, such
as health maintenance organizations (HMOs).
2
The Medicaid coverage category includes adults who had Medicaid or other state-sponsored health plans.
3
Adults not covered by private insurance, Medicaid, state-sponsored or other government-sponsored health plans (starting in 1997), Medicare, or military plans are considered
to have no health insurance coverage. Adults with only Indian Health Service coverage are considered to have no health insurance coverage.
4
Preliminary data based on the National Health Interview Survey’s Early Release program. Estimates based on the preliminary file may differ from estimates based on the final
annual file and have larger standard errors associated with them than standard errors based on a final annual file. Available from: Cohen RA, Terlizzi EP, Martinez ME. Health
insurance coverage: Early release of estimates from the National Health Interview Survey, 2018 preliminary file. National Center for Health Statistics. May 2019. Available from:
https://www.cdc.gov/nchs/data/nhis/earlyrelease/insur201902.pdf and National Health Interview Survey, 2018. For more information, visit: https://www.cdc.gov/nchs/nhis.
htm.
NOTES: SE is standard error. Data are for the civilian noninstitutionalized population. Health insurance coverage is at the time of interview. Health insurance categories are
mutually exclusive. A small percentage of persons are covered by Medicare, military plans, or other plans. Estimates for this group are not presented.
SOURCE: NCHS, National Health Interview Survey. See Appendix I, National Health Interview Survey (NHIS).

Health, United States, 2018 51
Technical Notes
Data Sources
Data for the Health, United States, 2018, Chartbook
come from many surveys and data systems and cover a
broad range of years. Some analyses present estimates
for the most recent data year for topics of public health
interest, while other analyses present trends over 10 years,
ending with the most recent data available. When 10 years
of data are not available, the analyses cover a time period
as close as possible to 10 years given the constraints of
the data source. Detailed descriptions of the data sources
included in the Chartbook are provided in Appendix I. Data
Sources. Additional information clarifying and qualifying the
data is included in the data table notes and in Appendix II.
Definitions and Methods.
Data Presentation
Many measures in the Chartbook are shown for people
in specific age groups because of the strong effect of age on
most health outcomes. In some cases, age-adjusted rates
and age-adjusted percentages are computed to eliminate
differences in observed rates that result from age differences
in population composition (see Appendix II, Age adjustment).
Age-adjusted rates and age-adjusted percentages are noted
as such in the text; rates and percentages without this
notation are crude rates and percentages. For some charts,
data from multiple years are combined to increase the
sample size and the statistical reliability of the estimates.
Some charts present time trends; others focus on
differences in estimates among population subgroups for
the most recent time period available. Trends are generally
shown on a linear scale to emphasize absolute differences
over time. However, some trends are shown on the log scale
so that rates that differ substantially can be shown on the
same chart.
One chart presents geographic differences in health
resources by state. Data in the state map are categorized
using a modification of the Jenks natural breaks classification
method. The Jenks method clusters data into groups that
minimize the within-group variance and maximize the
between-group variance (92), but does not take standard
errors into account. The modification rounds the data values
in order to assist map reading by a general audience, such
that the upper value of each of the first three categories is
one-tenth below the first value in the next category.
Point estimates and standard errors for Chartbook
figures are available in the Chartbook data tables that follow
the figures. Chartbook data tables may include additional
data that are not found in the figure.
Statistical Reliability of Estimates
Estimates for the total population generally have
relatively small sampling errors and high precision, but
estimates for certain population subgroups may be based on
small numbers of respondents or events and have relatively
large sampling errors or low precision (93). Numbers of
deaths obtained from the National Vital Statistics System
(NVSS) used in the Chartbook represent complete counts and
are not subject to sampling error. They are, however, subject
to random variation, which means that the number of events
that actually occur in a given year may be considered as one
of a large series of possible results that could have arisen
under the same circumstances. When the number of events
and the probability of such an event are small, estimates may
be unreliable.
Estimates that are unreliable because of large sampling
errors, low precision, small denominators, or small numbers
of events have been noted with an asterisk. The criteria used
to designate or suppress statistically unreliable estimates are
indicated in the notes of the applicable tables or charts.
For National Center of Health Statistics (NCHS) surveys,
point estimates and their corresponding sampling variances
were calculated using the SUDAAN software package,
which takes into consideration the complex survey design
(94). Standard errors for other surveys or data sets were
computed using the methodology recommended by the
programs providing the data, or were provided directly by
those programs. In Health, United States, 2018, the reliability
of survey percentage estimates was assessed based on a
minimum denominator sample size and on the absolute and
relative width of the Clopper-Pearson confidence interval
(adapted for complex surveys by Korn and Graubard), which
determines if the estimate is unreliable and should be
suppressed (93).
In the online-only supplementary Trend Tables, this
approach has been applied specifically to estimates from
the National Health and Nutrition Examination Survey
(NHANES) beginning with the 2013–2014 cycle, and to
estimates from the National Health Interview Survey (NHIS)
beginning with 2016. The reliability of estimates for prior
years was evaluated based on relative standard errors. For
more information on each approach, see Appendix II, Data
presentation standards for proportions; Relative standard
error (RSE).
Statistical Testing
Statistical trends can be analyzed in many ways. The
approaches used in this Chartbook to analyze trends in
health measures over time depend primarily on the data
52 Health, United States, 2018
source (NCHS surveys, vital statistics, other data sources),
but also consider the type of dependent variable and the
number of data points (1). With sufficient data points,
statistical analyses can detect not only whether an increase
or decrease has occurred, but can determine if and when
there has been a change in trend. Some trends are analyzed
using the weighted least squares regression method in
the National Cancer Institute’s Joinpoint software version
4.6.0.0. (Joinpoint), which identifies the number and location
of joinpoints when changes in trend have occurred (95).
For more information on Joinpoint, see: http://surveillance.
cancer.gov/joinpoint.
Trends in survey data, including NHANES and NHIS
(Figures 8–11,12,14,15,19,20) are based on record-level
data. Trends are first assessed using polynomial regression
(SUDAAN PROC REGRESS). Linear, quadratic, and cubic trends
are tested in separate regression models covering the entire
period shown in the figure. Quadratic trends are tested with
both linear and quadratic terms in the model, and cubic
trends are tested with linear, quadratic, and cubic terms in
the model. If a cubic trend is statistically significant and the
analysis included at least 11 time points, Joinpoint software
is used to search for up to two inflection points with as
few as two observed time points allowed in the beginning,
middle, and ending line segments (not counting the inflection
points). If a quadratic trend is statistically significant and the
analysis included at least seven time points, Joinpoint is used
to search for an inflection point in the linear trend, with an
overall p-value of 0.05 and Grid search method. In analyses
with fewer than 10 time points, the Bayesian Information
Criterion (BIC) model is used. In analyses with 10 or more
time points, the permutation model is used. Difference
in slopes between the two segments on either side of an
inflection point is then assessed using piecewise linear
regression (SUDAAN PROC REGRESS). To conduct piecewise
linear regression of age-adjusted estimates, survey weights
are adjusted for age. If a quadratic trend is statistically
significant and the analysis included three to six time points,
pairwise differences between percentages are tested using
two-sided significance tests (z-tests) to obtain additional
information regarding changes in the trend.
Trend analyses of birth data, infant mortality, and
death rates using vital statistics data from NVSS (Figures
1–6) are based on aggregated point estimates and their
standard errors. Increases or decreases in the estimates
during the entire time period shown are assessed using
Joinpoint with an overall p-value of 0.05 and Grid search
method. In analyses with fewer than 10 time points, the
BIC model is used. In analyses with 10 or more time points,
the permutation model is used. The maximum number of
joinpoints searched for is limited to one because there are
no more than 11 time points in any analysis. As few as two
observed time points are allowed in beginning and ending
line segments (not counting the inflection points). Trend
analyses using Joinpoint are carried out on the log scale for
birth, infant mortality, and death rates so that results provide
estimates of average annual percent change.
For other data sources, either the difference between
two points is assessed for statistical significance using z-tests
or the statistical testing methods recommended by the data
systems are used. For analyses that show two time points,
the differences between the two points are assessed for
statistical significance at the 0.05 level using z-tests without
correction for multiple comparisons. For data sources with
no standard errors, relative differences greater than 10% are
generally discussed in the text.
Terms such as “similar,” “no difference,” “stable,” and
“no clear trend” indicate that the statistics being compared
are not significantly different or that the slope of the
trend line is not significantly different from zero. Unless
otherwise noted in the text, differences that are described
are statistically significant at the 0.05 level. However, lack of
comment regarding the difference between statistics does
not necessarily suggest that the difference was tested and
found not to be significant. Chartbook data tables include
point estimates and standard errors, when available, for
users who would like to perform additional statistical tests.
Statistical significance of differences or trends is partly
a function of sample size (the larger the sample, the smaller
the change that can be detected); statistical significance does
not always indicate public health significance (96). Moreover,
a small sample size may result in statistically nonsignificant
results despite the existence of potentially meaningful
differences (97).

Health, United States, 2018 53
References
1. Ingram DD, Malec DJ, Makuc DM, Kruszon-Moran D,
Gindi RM, Albert M, et al. National Center for Health
Statistics guidelines for analysis of trends. National
Center for Health Statistics. Vital Health Stat 2(179).
2018.
2. World Health Organization. Life expectancy. Global
Health Observatory (GHO) data. Available from: http://
www.who.int/gho/mortality_burden_disease/life_
tables/situation_trends_text/en/.
3. Xu JQ, Murphy SL, Kochanek KD, Bastian B, Arias E.
Deaths: Final data for 2016. Natl Vital Stat Rep; vol 67 no
5. Hyattsville, MD: National Center for Health Statistics.
2018.
4. Kochanek KD, Arias E, Anderson RN. How did cause of
death contribute to racial differences in life expectancy
in the United States in 2010? NCHS Data Brief, no 125.
Hyattsville, MD: National Center for Health Statistics.
2013.
5. Murphy SL, Xu JQ, Kochanek KD, Arias E. Mortality in the
United States, 2017. NCHS Data Brief, no 328. Hyattsville,
MD: National Center for Health Statistics. 2018.
6. Reidpath DD, Allotey P. Infant mortality rate as an
indicator of population health. J Epidemiol Community
Health 57(5):344–6. 2003.
7. Singh GK, van Dyck PC. Infant mortality in the
United States, 1935–2007: Over seven decades of
progress and disparities. Rockville, MD: Health Resources
and Services Administration, Maternal and Child Health
Bureau. 2010.
8. Hoyert DL. 75 years of mortality in the United States,
1935–2010. NCHS Data Brief, no 88. Hyattsville, MD:
National Center for Health Statistics. 2012.
9. Hedegaard H, Miniño AM, Warner M. Drug overdose
deaths in the United States, 1999–2017. NCHS Data
Brief, no 329. Hyattsville, MD: National Center for Health
Statistics. 2018.
10. Warner M, Chen LH, Makuc DM, Anderson RN, Miniño
AM. Drug poisoning deaths in the United States, 1980–
2008. NCHS Data Brief, no 81. Hyattsville, MD: National
Center for Health Statistics. 2011.
11. Spencer MR, Warner M, Bastian BA, Trinidad JP,
Hedegaard H. Drug overdose deaths involving fentanyl,
2011–2016. Natl Vital Stat Rep; vol 68 no 3. Hyattsville,
MD: National Center for Health Statistics. 2019.
12. Scholl L, Seth P, Kariisa M, Wilson N, Baldwin G. Drug and
opioid-involved overdose deaths - United States, 2013–
2017. MMWR Morb Mortal Wkly Rep 67(5152):1419–27.
2018.
13. Martinez G, Copen CE, Abma JC. Teenagers in the
United States: Sexual activity, contraceptive use, and
childbearing, 2006–2010 National Survey of Family
Growth. National Center for Health Statistics. Vital
Health Stat 23(31). 2011.
14. Ventura SJ, Hamilton BE, Mathews TJ. National and state
patterns of teen births in the United States, 1940–2013.
Natl Vital Stat Rep; vol 63 no 4. Hyattsville, MD: National
Center for Health Statistics. 2014.
15. Hoffman SD, Maynard RA. Kids having kids: The
economic and social costs of teenage pregnancy.
Washington, DC: Urban Institute Press. 2008.
16. Chang HH, Larson J, Blencowe H, Spong CY, Howson CP,
Cairns-Smith S, et al. Preventing preterm births: Analysis
of trends and potential reductions with interventions in
39 countries with very high human development index.
Lancet 381(9862):223–34. 2013.
17. Ancel PY, Goffinet F, EPIPAGE-2 Writing Group, Kuhn
P, Langer B, Matis J, et al. Survival and morbidity of
preterm children born at 22 through 34 weeks’ gestation
in France in 2011: Results of the EPIPAGE-2 cohort study.
JAMA Pediatr 169(3):230–8. 2015.
18. Adams JN, Feldman HM, Huffman LC, Loe IM. Sensory
processing in preterm preschoolers and its association
with executive function. Early Hum Dev 91(3):227–33.
2015.
19. Brown L, Burns YR, Watter P, Gibbons KS, Gray PH.
Motor performance, postural stability and behaviour of
non-disabled extremely preterm or extremely low birth
weight children at four to five years of age. Early Hum
Dev 91(5):309–15. 2015.
20. van der Pal-de Bruin KM, van der Pal SM, Verloove-
Vanhorick SP, Walther FJ. Profiling the preterm or VLBW
born adolescent; implications of the Dutch POPS cohort
follow-up studies. Early Hum Dev 91(2):97–102. 2015.
21. MacDorman MF, Mathews TJ. Understanding racial and
ethnic disparities in U.S. Infant mortality rates. NCHS
Data Brief, no 74. Hyattsville, MD: National Center for
Health Statistics. 2011.
22. Martin JA, Hamilton BE, Osterman MJK, Driscoll AK,
Drake P. Births: Final data for 2017. Natl Vital Stat Rep;
vol 67 no 8. Hyattsville, MD: National Center for Health
Statistics. 2018.
23. Martin JA, Osterman MJK. Describing the increase in
preterm births in the United States, 2014–2016. NCHS
Data Brief, no 312. Hyattsville, MD: National Center for
Health Statistics. 2018.
24. U.S. Department of Health and Human Services. The
health consequences of smoking—50 years of progress:
A report of the Surgeon General. Atlanta, GA: Office of
Surgeon General. 2014.
25. U.S. Department of Health and Human Services.
E-cigarette use among youth and young adults. Atlanta,
GA: Office of Surgeon General. 2016.
26. Gentzke AS, Creamer M, Cullen KA, Ambrose BK, Willis
G, Jamal A, King BA. Vital signs: Tobacco product use
among middle and high school students—United States,
2011–2018. MMWR Morb Mortal Wkly Rep 68(6):157–
64. 2019.
54 Health, United States, 2018
27. Singh AS, Mulder C, Twisk JW, van Mechelen W,
Chinapaw MJ. Tracking of childhood overweight into
adulthood: A systematic review of the literature. Obes
Rev 9(5):474–88. 2008.
28. Engeland A, Bjorge T, Tverdal A, Sogaard AJ. Obesity
in adolescence and adulthood and the risk of adult
mortality. Epidemiology 15(1):79–85. 2004.
29. May AL, Kuklina EV, Yoon PW. Prevalence of
cardiovascular disease risk factors among US
adolescents, 1999–2008. Pediatrics 129(6):1035–41.
2012.
30. Institute of Medicine. Accelerating progress in obesity
prevention: Solving the weight of the nation. Glickman
D, Parker L, Sim LJ, Del Valle Cook H, Miller EA, editors.
Washington, DC: National Academies Press. 2012.
31. Must A, Hollander SA, Economos CD. Childhood obesity:
A growing public health concern. Expert Rev Endocrinol
Metab 1(2):233–54. 2006.
32. Jensen MD, Ryan DH, Apovian CM, Ard JD, Comuzzie
AG, Donato KA, et al. 2013 AHA/ACC/TOS guideline for
the management of overweight and obesity in adults: A
report of the American College of Cardiology/American
Heart Association Task Force on Practice Guidelines and
The Obesity Society. Circulation 129(25 Suppl 2):S102–
38. 2014.
33. NHLBI Obesity Education Initiative Expert Panel on the
Identification, Evaluation, and Treatment of Overweight
and Obesity in Adults. Clinical guidelines on the
identification, evaluation, and treatment of overweight
and obesity in adults—The evidence report. NIH pub
no 98–4083. Bethesda, MD: National Heart, Lung, and
Blood Institute, National Institutes of Health. 1998.
34. National Heart, Lung, and Blood Institute. Managing
overweight and obesity in adults. Systematic evidence
review from the Obesity Expert Panel, 2013. Bethesda,
MD: 2013.
35. Flegal KM, Graubard BI, Williamson DF, Gail MH. Excess
deaths associated with underweight, overweight, and
obesity. JAMA 293(15):1861–7. 2005.
36. Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of
obesity among adults and youth: United States, 2015–
2016. NCHS Data Brief, no 288. Hyattsville, MD: National
Center for Health Statistics. 2017.
37. National Heart, Lung, and Blood Institute. Expert panel
report 3: Guidelines for the diagnosis and management
of asthma. NIH pub no 07–4051. Bethesda, MD: National
Institutes of Health. 2007.
38. Zahran HS, Bailey CM, Damon SA, Garbe PL, Breysse PN.
Vital signs: Asthma in children—United States, 2001–
2016. MMWR Morb Mortal Wkly Rep 67(5):149–55.
2018.
39. Akinbami LJ, Moorman JE, Liu X. Asthma prevalence,
health care use, and mortality: United States, 2005–
2009. Natl Vital Stat Rep; vol no 32. Hyattsville, MD:
National Center for Health Statistics. 2011.
40. Szefler SJ. Asthma across the lifespan: Time for a
paradigm shift. J Allergy Clin Immunol 142(3):773–80.
2018.
41. Henquin JC. Triggering and amplifying pathways of
regulation of insulin secretion by glucose. Diabetes
49(11):1751–60. 2000.
42. American Diabetes Association. Standards of medical
care in diabetes—2018. Diabetes Care 41 (suppl 1):S38–
50. 2018.
43. National Heart, Lung, and Blood Institute. The seventh
report of the Joint National Committee on Prevention,
Detection, Evaluation, and Treatment of High Blood
Pressure. Bethesda, MD: National Institutes of Health.
2004.
44. Whelton PK, Carey RM, Aronow WS, Casey DE, Jr.,
Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/
AAPA/ABC/ACPM/AGS/APHA/ASH/ASPC/NMA/PCNA
guideline for the prevention, detection, evaluation,
and management of high blood pressure in adults:
Executive summary: A report of the American College
of Cardiology/American Heart Association task force on
clinical practice guidelines. Hypertension 71(6):1269–
324. 2018.
45. Patel SA, Winkel M, Ali MK, Narayan KM, Mehta NK.
Cardiovascular mortality associated with 5 leading
risk factors: National and state preventable fractions
estimated from survey data. Ann Intern Med 163(4):245–
53. 2015.
46. Danaei G, Ding EL, Mozaffarian D, Taylor B, Rehm J,
Murray CJ, Ezzati M. The preventable causes of death
in the United States: Comparative risk assessment of
dietary, lifestyle, and metabolic risk factors. PLoS Med
6(4):e1000058. 2009.
47. Zanchetti A, Thomopoulos C, Parati G. Randomized
controlled trials of blood pressure lowering in
hypertension: A critical reappraisal. Circ Res
116(6):1058–73. 2015.
48. Zhou D, Xi B, Zhao M, Wang L, Veeranki S. Uncontrolled
hypertension increases risk of all-cause and
cardiovascular disease mortality in US adults: The
NHANES III Linked Mortality Study. Scientific Reports
8(9418). 2018.
49. World Health Organization. International classification of
functioning, disability, and health (ICF) [online]. Geneva,
Switzerland: World Health Organization. 2001.
50. Centers for Disease Control and Prevention. Ten great
public health achievements—United States, 2001–2010.
MMWR Morb Mortal Wkly Rep 60(19):619–23. 2011.
51. Zhou F, Shefer A, Wenger J, Messonnier M, Wang LY,
Lopez A, et al. Economic evaluation of the routine
childhood immunization program in the United States,
2009. Pediatrics 133(4):577–85. 2014.
52. Ezeanolue E, Harriman K, Hunter P, Kroger A, Pellegrini
C. General best practice guidelines for immunization.
Best practices guidance of the Advisory Committee on
Immunization Practices (ACIP). Atlanta, GA: Advisory
Committee on Immunization Practices, National Center
for Immunization and Respiratory Diseases. 2019.
Health, United States, 2018 55
53. Centers for Disease Control and Prevention.
Achievements in public health, 1900–1999: Control
of infectious diseases. MMWR Morb Mortal Wkly Rep
48(29):621–9. 1999.
54. Carey RM, Whelton PK, 2017 ACC/AHA Hypertension
Guideline Writing Committee. Prevention, detection,
evaluation, and management of high blood pressure
in adults: Synopsis of the 2017 American College of
Cardiology/American Heart Association Hypertension
Guideline. Ann Intern Med 168(5):351–8. 2018.
55. Stone NJ, Robinson JG, Lichtenstein AH, Bairey Merz CN,
Blum CB, Eckel RH, et al. 2013 ACC/AHA guideline on the
treatment of blood cholesterol to reduce atherosclerotic
cardiovascular risk in adults: A report of the American
College of Cardiology/American Heart Association Task
Force on Practice Guidelines. Circulation 129(25 Suppl
2):S1–45. 2014.
56. G.B.D. 2016 Disease and Injury Incidence and Prevalence
Collaborators. Global, regional, and national incidence,
prevalence, and years lived with disability for 328
diseases and injuries for 195 countries, 1990–2016: A
systematic analysis for the Global Burden of Disease
Study 2016. Lancet 390(10100):1211–59. 2017.
57. Howard DH, Chernew ME, Abdelgawad T, Smith
GL, Sollano J, Grabowski DC. New anticancer drugs
associated with large increases in costs and life
expectancy. Health Aff (Millwood) 35(9):1581–87. 2016.
58. Gellad WF, Donohue JM, Zhao X, Zhang Y, Banthin JS. The
financial burden from prescription drugs has declined
recently for the nonelderly, although it is still high for
many. Health Aff (Millwood) 31(2):408–16. 2012.
59. Mulcahy AW, Eibner C, Finegold K. Gaining coverage
through Medicaid or private insurance increased
prescription use and lowered out-of-pocket spending.
Health Aff (Millwood) 35(9):1725–33. 2016.
60. Shallcross LJ, Davies DS. GP antibiotic overuse and
microbial resistance. Br J Gen Pract 65(631):61–2. 2015.
61. Ackerman S, Gonzales R. The context of antibiotic
overuse. Ann Intern Med 157(3):211–2. 2012.
62. Bushardt RL, Massey EB, Simpson TW, Ariail JC, Simpson
KN. Polypharmacy: Misleading, but manageable. Clin
Interv Aging 3(2):383–9. 2008.
63. Shehab N, Lovegrove MC, Geller AI, Rose KO, Weidle
NJ, Budnitz DS. US emergency department visits for
outpatient adverse drug events, 2013–2014. JAMA
316(20):2115–25. 2016.
64. Jones CM, Mack KA, Paulozzi LJ. Pharmaceutical
overdose deaths, United States, 2010. JAMA 309(7):657–
9. 2013.
65. Institute of Medicine. Crossing the quality chasm: A new
health system for the 21st century. Washington, DC:
National Academies Press. 2001.
66. Mojtabai R, Olfson M. Medication costs, adherence, and
health outcomes among Medicare beneficiaries. Health
Aff (Millwood) 22(4):220–9. 2003.
67. Piette JD, Heisler M, Wagner TH. Cost-related medication
underuse among chronically ill adults: The treatments
people forgo, how often, and who is at risk. Am J Public
Health 94(10):1782–7. 2004.
68. U.S. Department of Health and Human Services. Oral
health in America: A report of the Surgeon General.
Rockville, MD: Office of the Surgeon General. 2000.
69. National Center for Chronic Disease Prevention and
Health Promotion. Oral health: Working to improve oral
health for all Americans. Atlanta, GA: Centers for Disease
Control and Prevention (CDC). 2016.
70. Dye B, Thornton-Evans G, Li X, Iafolla T. Dental caries
and tooth loss in adults in the United States, 2011–2012.
NCHS Data Brief, no 197. Hyattsville, MD: National
Center for Health Statistics. 2015.
71. Fleming E, Afful J. Prevalence of total and untreated
dental caries among youth: United States, 2015–2016.
NCHS Data Brief, no 307. Hyattsville, MD: National
Center for Health Statistics. 2018.
72. Health Policy Institute. Supply and profile of dentists:
Supply of dentists in the U.S.: 2001–2017. 2018. Available
from: https://www.ada.org/en/science-research/health-
policy-institute/data-center/supply-and-profile-of-
dentists.
73. Bureau of Health Workforce, Health Resources and
Services Administration. Third quarter of fiscal year 2019
designated HPSA quarterly summary. Rockville, MD: U.S.
Department of Health and Human Services. 2019.
74. Munson B, Vujicic M. Supply of full-time equivalent
dentists in the U.S. expected to increase steadily.
Chicago, IL: American Dental Association. 2018.
75. Wehby GL, Shane DM, Joshi A, Momany E, Chi DL, Kuthy
RA, Damiano PC. The effects of distance to dentists and
dentist supply on children’s use of dental care. Health
Serv Res 52(5):1817–34. 2017.
76. Edelstein BL, Chinn CH. Update on disparities in oral
health and access to dental care for America’s children.
Acad Pediatr 9(6):415–9. 2009.
77. Harris-Kojetin L, Sengupta M, Park-Lee E, Valverde R.
Long-term care services in the United States: 2013
overview. Vital Health Stat 3(37). 2013.
78. Harris-Kojetin L, Sengupta M, Park-Lee E, Valverde R,
Caffrey C, Rome V, Lendon J. Long-term care providers
and services users in the United States: Data from the
National Study of Long-Term Care Providers, 2013–2014.
Vital Health Stat 3(38). 2016.
79. McCormick JC, Chulis GS. MCBS highlights: Growth in
residential alternatives to nursing homes: 2001. Health
Care Finance Rev 24(4):143–50. 2003.
80. Harris-Kojetin L, Sengupta M, Lendon JP, Rome V,
Valverde R, Caffrey C. Long-term care providers and
services users in the United States, 2015–2016. Vital
Health Stat 3(43). 2019.
81. Martin AB, Hartman M, Washington B, Catlin A, The
National Health Expenditure Accounts Team. National
health care spending in 2017: Growth slows to post-
Great Recession rates; share of GDP stabilizes. Health Aff
(Millwood) 38(1):96–106. 2019.
56 Health, United States, 2018
82. Hartman M, Martin AB, Espinosa N, Catlin A, The
National Health Expenditure Accounts Team. National
health care spending in 2016: Spending and enrollment
growth slow after initial coverage expansions. Health Aff
(Millwood) 37(1):150–60. 2017.
83. National Health Statistics Group, National Health
Expenditure Accounts, National Health Expenditures
[Internet]. Available from: https://www.cms.gov/
Research-Statistics-Data-and-Systems/Statistics-
Trends-and-Reports/NationalHealthExpendData/
NationalHealthAccountsHistorical.html.
84. American Academy of Pediatrics. 2016 recommendations
for preventive pediatric health care. Pediatrics 137(1):
25–7. 2016.
85. Title XIX of the Social Security Act, 42 U.S.C. 1396 et seq.
86. Title XXI of the Social Security Act, 42 U.S.C. 1397aa–
1397mm.
87. Larson K, Cull WL, Racine AD, Olson LM. Trends in access
to health care services for US children: 2000–2014.
Pediatrics 138(6):1–9. 2016.
88. Cohen RA, Terlizzi EP, Martinez ME. Health insurance
coverage: Early release of estimates from the National
Health Interview Survey, 2018. National Center for
Health Statistics. 2019.
89. Institute of Medicine. America’s uninsured crisis:
Consequences for health and health care. Washington,
DC: National Academies Press. 2009.
90. McWilliams JM. Health consequences of uninsurance
among adults in the United States: Recent evidence and
implications. Milbank Q 87(2):443–94. 2009.
91. Cunningham PJ, Felland LE. Falling behind: Americans’
access to medical care deteriorates, 2003–2007. Track
Rep 19:1–5. 2008.
92. Brewer CA, Pickle L. Evaluation of methods for classifying
epidemiological data on choropleth maps in series. Ann
Assoc of Am Geogr 92(4):662–81. 2002.
93. Parker JD, Talih M, Malec DJ, Beresovsky V, Carroll M,
Gonzalez Jr JF, et al. National Center for Health Statistics
data presentation standards for proportions. National
Center for Health Statistics. Vital Health Stat 2(175).
2017.
94. RTI International. SUDAAN (Version 11.0) [Statistical
software]. 2012.
95. National Cancer Institute, Division of Cancer Control &
Population Sciences, Surveillance Research Program.
Joinpoint trend analysis software (Version 4.6.0.0)
[Statistical software]. 2018.
96. National Center for HIV/AIDS, Viral Hepatitis, STD, and
TB Prevention. Youth Risk Behavior Surveillance System
(YRBSS). Interpretation of YRBS trend data. Atlanta, GA:
Centers for Disease Control and Prevention. 2016.
97. Wasserstein RL, Lazar NA. The ASA’s statement on
p-values: Context, process, and purpose. The American
Statistician 70(2):129–33. 2016.
