
1 Salud America! https://salud-america.org/
Nov. 14, 2017
RESEARCH REVIEW
The State of Latino Early
Childhood Development:
A Research Review
Authors
• Amelie G. Ramirez, Dr.P.H., Director, Salud America!, Professor, Institute for Health
Promotion Research, UT Health San Antonio
• Kipling J. Gallion, M.A., Deputy Director, Salud America!, Professor, Institute for Health
Promotion Research, UT Health San Antonio
• Rosalie Aguilar, M.A., Deputy Director, Salud America!, Professor, Institute for Health
Promotion Research, UT Health San Antonio
• Jennifer Swanson, M.Ed., JS Medical Communications, L.L.C.
About this Research Review
This report is copyright 2017 RWJF, Route 1 and College Road, P.O. Box 2316, Princeton, NJ,
08543-2316, www.rwjf.org
.
Abstract
Many Latino children are at risk of not receiving the proper care, services, and environment they
need during their formative years to promote healthy development.
Traumatic early childhood experiences, poor nutrition, physical inactivity, low participation in
preschool programs and early education, complex family and maternal structures, and other
factors have been shown to affect or impair Latino children’s social and emotional development,
academic achievement, and overall health and wellbeing.
Culturally sensitive programs and policies are increasingly needed to address the issues that
hinder healthy early development in Latino children.
Waiting for kindergarten is too late, because 90 percent of brain development occurs by age 5.

2 Salud America! https://salud-america.org/
This research review summarizes the current literature on Latino child development and the
programs and policies for improving early childhood development in Latino children.
Introduction
Childhood development is a dynamic, interactive process that is not predetermined by genetics,
but is hindered by lack of proper care, services, and support. Proper childhood development is
critical because 90 percent of brain development occurs by age 5.
Latino childhood development is particularly important because Latinos make up 26 percent of
US children younger than 5. The Latino population is one of the fastest-growing U.S.
demographics, yet 12 million Latinos live below the poverty level.
1–3
As such, many Latino
children are at risk of not receiving the care and services they need during their formative years,
which may have negative effects on their early development and long-lasting consequences into
their adulthood. Less than half of kids from low-income families are starting kindergarten ready
to learn, compared to three-fourths of kids from middle-income families.
4
For example, although research has shown the many health, social and emotional, and
cognitive benefits of high-quality preschool programs, U.S. Latino children have the lowest
participation in these programs among the major racial and ethnic populations (Figure 1).
5,6
Less than half of Latino children are enrolled in any early learning program and for those who do
attend, program quality varies widely.
7
Poverty confounds participation in quality early learning
programs.
Figure 1. Preschool Participation Rates in the U.S., by Race/Ethnicity
5
Lack of participation in preschool programs, in combination with other factors such as infrequent
exposure to preliteracy activities at home, has led to reduced school readiness in Latino children

3 Salud America! https://salud-america.org/
that may result in poor long-term outcomes.
5,6
Lack of participation may stem from lack of
availability. In a study about the location of child centers across eight states, 42% of children
younger than 5 live in areas known as child care deserts, which either have no child care
centers or so few centers that there are more than three times as many children as there are
spaces in centers. The availability of child care centers is in a state of crisis for Latino families.
More information about families’ proximity to child care programs can inform local, state, and
federal efforts to increase access to early childhood programs.
Early childhood experiences in school and at home have the potential to shape child
development, both positively and negatively. Adverse childhood experiences (ACEs) are of
particular concern as they can lead to a multitude of issues that can affect individuals for a
lifetime. Many children, including Latino children, have been exposed to ACEs that have in
some way impaired their socioemotional development, academic achievement, and overall
health and wellbeing.
8,9
Other factors affect the healthy development of Latino children. Children living in underserved
areas have limited access to healthy food. Poor nutrition can lead to a host of issues including
poor physical health and cognitive difficulties. Limited access to fruits and vegetables, and
overconsumption of fast foods and unhealthy snacks, can lead to overweight and obesity—a
growing area of concern for Latino children
10
—that increases their risk of poor long-term
outcomes in many developmental areas including physical and mental health, education,
psychosocial functioning, and future socioeconomic status.
11
Despite the disparities mentioned above, many Latino children have been shown to have
healthy social and emotional development, and these qualities may help to attenuate some of
the negative effects of their disadvantages.
1,12
Therefore, preserving and improving upon these
socioemotional strengths is crucial for ensuring healthy early childhood development in Latino
children.
Moreover, more than 400,000 Latino children younger than 4 were not counted in the 2010 U.S
Census.
13
Ensuring Latinos are accurately counted in the 2020 Census is important for ensuring
equitable investment for healthy early childhood development in Latino children.
This research review summarizes the current literature on the issues mentioned above and the
programs and policies for improving these areas of early childhood development in Latino
children.
Methodology
For this research review, electronic searches of PubMed, Google, Google Scholar, and
government and organization websites were performed to identify literature that was relevant to
early childhood development in Latino children.
Combinations of the following MeSH terms were used: “Latino,” "Hispanic Americans"[Mesh],
"Mexican Americans"[Mesh], "Child"[Mesh], "Policy"[Mesh], "Public Policy"[Mesh], "Policy
Making"[Mesh], "Health Policy"[Mesh], "Infant"[Mesh], "Child, Preschool"[Mesh], "Growth and
Development"[Mesh], "Child Welfare"[Mesh], and "Infant Welfare"[Mesh]. Keywords included
adverse childhood experiences, Latino, Hispanic, American, children, social, emotional,
development, parenting practices, education, depression, school, preschool, Head Start, and
teachers.

4 Salud America! https://salud-america.org/
Included in this review were studies, expert commentaries, and policy statements addressing
important aspects of early childhood development in Latino children, including disparities versus
other races and ethnicities, factors associated with healthy and unhealthy development, and
practices, programs, and policies for improving early childhood development in this population.
Exclusion criteria included articles written in non-English language and studies conducted
outside the United States. No limits were placed on publication date, but because of the breadth
and depth of the topic, only the most recent and relevant literature was included. Older studies
were included if they were deemed exceptionally important and relevant to current times. From
the initial search results, titles and abstracts were reviewed for relevance and cross-checked
against inclusion/exclusion criteria. Full text was obtained for relevant articles meeting the
inclusion criteria. Additional literature was found through hand searches of the bibliographies of
articles captured through the initial electronic searches. Research on non-Latino children and
older Latino children was included if deemed exceptionally important and potentially relevant to
Latino children in some way.
Key Research Results
• Adverse childhood experiences (ACEs) interfere with healthy early childhood
development in Latino children. Programs and policies aimed at preventing ACEs and/or
mitigating their harmful effects may improve overall health and wellbeing in Latino
children.
• Latino children have limited access to healthy foods, which negatively affects overall
development and wellbeing. Improving access to healthy foods at home, at school, and
in the neighborhood/community may improve health, development, and wellbeing in
Latino children.
• Latino children also have limited access to active spaces—such as trails, parks, and
recreation facilities—that may prevent them from engaging in adequate levels of physical
activity for healthy development. Improving access to active spaces may improve
physical activity and health and wellbeing.
• Latino children have low participation in high-quality preschool programs and face
educational disadvantages when starting kindergarten.
• Latino families share many common values—such as familism and marianismo—that
may benefit Latino childhood development and influence early childhood development
programs.
• Early childhood development programs that have long-term benefits for other minority
and low-income children also likely benefit Latino children.
• Family-, preschool-, and community-based interventions may help to improve school
readiness and lead to better developmental outcomes for Latino children.
• Programs and policies providing maternal and breastfeeding support and family support
services promote healthy social and emotional development and overall wellbeing in
Latino children.

5 Salud America! https://salud-america.org/
Studies Supporting Key Research Results
Adverse childhood experiences (ACEs) interfere with healthy early childhood
development in Latino children. Programs and policies aimed at preventing ACEs and/or
mitigating their harmful effects may improve overall health and wellbeing in Latino
children.
Growing up feeling safe, secure, and loved is essential for the healthy development of all
children,
14
yet 70% of all children are exposed to adverse childhood experiences (ACEs) by age
6 that may have negative effects on many aspects of their developmental.
8,9,15
ACEs may
include parental domestic violence, substance abuse, mental illness, criminal justice
involvement, child abuse and/or neglect, poverty/homelessness, and parental death, among
others.
16
Multiple studies have shown that children exposed to ACEs are more likely to develop
physical, mental, behavioral, psychosocial, and/or cognitive issues than children who have not
been exposed to ACEs, and these effects can extend into adolescence and adulthood.
17–24
About 30 percent of Latino children in U.S.-native families reported two or more ACEs,
25
compared to 16 percent of Latino children in immigrant families. Unmeasured confounders may
buffer Latino children from exposure to ACEs in immigrant families, and/or negative effects of
unmeasured factors for Latino children in U.S.-native families. Also, questions about ACEs may
not capture the adverse experiences specific to immigrant families; in fact, it is possible that
adverse experiences and environments that are specific to the immigrant experience are not
reflected in traditional measures of ACE exposure. For both the native and immigrant groups,
parental divorce and economic hardship were the most prevalent ACE exposures. Poor
maternal mental health and single-woman family structure had the strongest associations with
ACE exposure in both groups. Similarly, in both groups, low-income or middle-income
households (≤200% of FPL or 201%–400%) were associated with twice the odds of exposure to
two or more ACEs compared with those from a high-income reference group.
Many studies have evaluated the multitude of effects of ACEs on Latino children specifically,
and these are categorized below by outcome measure.
Physical Health. The Hispanic Community Health Study/Study of Latinos (HCHS/SOL)
Sociocultural Ancillary Study evaluated ACEs in 5,117 Latino adolescents and adults (ages 18-
74) and found that 77.8% experienced at least one ACE, which stands in contrast to the 70% of
youth in general who are exposed to ACEs. The same study on Latino adolescents and adults
found that 28.7% experienced four ACEs or more.
26
Among the ACEs reported, the most
common were parental separation/divorce, emotional or physical abuse, and household
alcohol/drug abuse. After controlling for demographics and risk factors in this Latino population,
ACEs were found to be positively associated with multiple health-related conditions later in life,
including alcohol and tobacco use, coronary heart disease, chronic obstructive pulmonary
disease, and cancer. Although this study did not find an association between ACEs and asthma,
another study that used 2011 to 2012 data from the National Survey of Children’s Health (N =
92,472; ages 0-17; 10.3% Latino) reported a 4.46 times increase in lifetime asthma among
Latino children experiencing four ACEs compared with those experiencing no ACEs.
Importantly, white children experiencing four ACEs had only a 1.19 times increase in lifetime
asthma.
27
Another study that used data from the HCHS/SOL Sociocultural Ancillary Study found that
economic hardship during childhood was associated with shorter height among Latinos
regardless of birth place and with greater adiposity in U.S.-born Latinos only.
28
Short stature and
adiposity may lead to chronic health issues later in life, but this study did not assess for those

6 Salud America! https://salud-america.org/
associations in the adult participants. Further research is needed to understand the full effects
of childhood poverty on the development of chronic diseases in Latinos.
The Carolina Abecedarian Project (ABC) was designed as a social experiment to test if
stimulating the early care environment from birth to age 5 could prevent the development of mild
mental retardation in disadvantaged children.
29
Curriculum emphasized development of
language, emotional regulation, and cognitive skills, as well as caregiving, supervised play, two
meals, one snack, and primary pediatric care for the first five years of life. In their mid-30s,
participants had lower blood pressure, better lipid levels, and lower abdominal obesity. They
were less likely to have Metabolic Syndrome and had lower risk of experience Coronary Heart
Disease. Of participants and non-participants studied, those who are obese or severely obese in
their mid-30s are already on a trajectory of above-normal BMI in the first five years of their lives.
Children randomly assigned to stimulating early care from birth to age 5 had significantly lower
risk factors for cardiovascular and metabolic diseases in their mid-30s.
29
Mental Health. A study of data on youth from the Florida Department of Juvenile Justice (N =
64,329; 15.37% Latino) evaluated the effects of ACEs on suicide attempts, as mediated by
maladaptive behavior including personality development (aggression and impulsivity) and
problem behaviors (school difficulties and substance abuse).
30
Latino youth with higher ACE
scores were found to have significantly and directly increased odds of attempting suicide, as
well as school misconduct. Although Latino youth were less likely to experience ACEs and
attempt suicide than their white counterparts, they were more likely to have aggression, which
was a predictor of suicide. Efforts should be made to identify ACEs and
developmental/behavioral issues early to prevent potential suicidal behavior in Latinos and all
children.
Childhood maltreatment exposure was associated with mental health problems classified as
internalizing (anxiety, depression, withdrawal, somatic complaints) and externalizing
(delinquency, aggression) among Latino, non-Latino white, and black groups in one study of the
use of mental health services by children who had been exposed to some form of maltreatment
and were being investigated by child welfare services.
31
The study (N = 1,600; 19.3% Latino)
found that neither internalizing nor externalizing problems predicted the use of mental health
service in Latinos, which is contrary to previous findings suggesting that Latinos with
externalizing problems are just as likely to use mental health services as their white and black
counterparts.
32
The lack of significant association is potentially attributed to the smaller Latino
sample size in this study, as noted by the authors. However, other factors such as cultural and
family issues may dissuade Latino parents from following through on referrals made to mental
health services after their child’s exposure to maltreatment. Thus, additional research is needed
to identify the predictors of mental health service use among Latino youth and develop the
necessary assessment and counseling tools to identify at-risk Latino youth and get them the
mental health services they need to improve their mental health.
Read the full Salud America! research review on mental health and Latino children.
33
Substance Use/Abuse. A study of 1,259 Puerto Rican youth (10 or older at baseline) from the
South Bronx, New York and San Juan, Puerto Rico found that child maltreatment, parental
maladjustment, and sociocultural stressors increased the risk of early alcohol use (by age 14) in
this youth population.
34
Linear relationships were observed between the number of ACEs to
which a child was exposed and the risk of early drinking. Another study of 1,420 Latino
emerging adults in Southern California found that the presence of ACEs was significantly
associated with substance use or abuse, specifically cigarette, alcohol, marijuana, and hard

7 Salud America! https://salud-america.org/
drug use. As the number of ACEs increased, so did the substance use for all substances.
35
Depressive symptoms stemming from ACEs can also increase the risk of substance use/abuse,
so identifying and treating depression may help to reduce the substance use/abuse, although it
is likely that many factors are involved and further symptoms assessment and intervention may
be warranted.
36
Education/achievement. Children ages 3 to 5 who have had two or more ACEs are over four
times more likely to have trouble calming themselves down, be easily distracted, and have a
hard time making and keeping friends. More than three of four children ages 3-5 who have been
expelled from preschool also had ACEs.
37
A study of urban children (N = 1,007; 24% Latino) used data from the Fragile Families and Child
Wellbeing Study, a national urban birth cohort, to evaluate the effects of ACEs on kindergarten
outcomes.
20
Children exposed to three or more ACEs were more likely to have below-average
language and literacy skills, poor math and emergent literacy skills, attention problems, and
aggression in kindergarten. However, the data were not analyzed separately for Latinos.
Preventing ACEs and/or mitigating their harmful effects is critical for improving prospects for
early child development, and many programs and interventions have been implemented in this
regard.
The American Academy of Pediatrics (AAP) recommends early screening for developmental
and behavioral problems starting at age 9 months through 3 years.
38
The Birth to 5: Watch Me
Thrive! initiative is a federal effort to promote healthy child development through care
collaboration and a system-wide approach, and provides screening resources for families,
educators, and various healthcare providers (https://www.acf.hhs.gov/ecd/child-health-
development/watch-me-thrive).
39
Home visits have been also shown to help prevent ACEs by providing parents and caregivers
with the necessary support, knowledge, and tools to promote a healthy, nurturing home
environment for their children.
40
Proactively building trust, security, and resilience in families can
help children process and overcome the effects of ACEs should they occur. Home visitors
educate expecting and new parents about nutrition, sleep habits, and health care, do family and
child assessments to screen for ACEs (e.g., through family map inventories [FMIs],
41
and make
referrals to programs such as WIC, Medicaid, heat and housing programs, and domestic
violence services, as needed, to help them build a stable and healthy family. Moreover,
culturally-appropriate home visits that engage family and community members are especially
important for improving outcomes in Latino youth who may have mental health issues stemming
from ACEs or other reasons. For example, Project Wings Home Visits, a home visit program
aimed at improving mental health awareness among Latinos has shown progress in reducing
mental health issues in Latino youth.
42
Family-based home visit programs are especially
important for Latino families, as multiple family members may be living in the home and can play
an important role in promoting a healthy environment for Latino youth.
The pediatric medical home model, promoted by the AAP, has been studied as a potential
intervention to mitigate the harmful effects of ACEs. The medical home model is a continuous
and comprehensive approach to healthcare from infancy through young adulthood. In a study
using data from the 2011-12 National Survey of Children’s Health, children were evaluated for
physical and psychological health, social activities, educational achievement, ACE exposure
and medical home access.
43

8 Salud America! https://salud-america.org/
Children were considered to have a medical home if they met the following criteria:
• Having a personal doctor or nurse
• Having a usual source for sick and well care
• Receiving family-centered care
• Getting referrals for specialty care when needed
• Having effective care coordination when needed
Medical home access was associated with greater wellbeing in children. Among children ages
6-11 who had experienced ACEs, access to a medical home resulted in higher levels of
wellbeing compared with no access to a medical home, suggesting that medical homes may
contribute to early ACE prevention, identification, and intervention. Importantly, children in
minority groups and those living in poverty or without insurance are less likely to have a medical
home than their white, more affluent, and insured counterparts,
44
so strategies for improving
access to a medical home in Latino children falling into these categories may be warranted.
Supportive relationships and teaching resilience skills can mitigate the effects of ACEs. Children
ages 6-17 who have had two or more ACEs but learned to stay calm and in control when faced
with challenges are over three times more likely to be engaged in school compared to peers
who have not learned these skills.
37
Other interventions for preventing, identifying and/or addressing ACEs may include screening
for ACEs during primary care visits and child welfare assessments, early care and education
(ECE), mindfulness-based, mind-body approaches, parent-child psychotherapy, and family
resilience programs, and quality and affordable childcare, among others.
40,45–51
ECE programs
and systems, for example, can provide trauma-informed care (TIC), which supports children’s
recovery and resilience using evidence-based approaches. A report by Child Trends identified
emerging TIC approaches: integrating trauma-informed strategies into existing ECE programs to
support children in those programs who have experienced trauma, building partnerships and
connections between ECE and community service providers to facilitate screenings of and
service provision to children and families; implementing professional standards and training for
infant and early childhood mental health consultants that emphasize TIC, and supporting the
professional development and training of the ECE workforce in working with and supporting
young children who have experienced trauma.
52
Regardless of the intervention used, cultural
sensitivity and relevance is important for addressing ACE issues that are specific to Latinos.
53
Latino children have limited access to healthy foods, which negatively affects overall
development and wellbeing. Improving access to healthy foods at home, at school, and
in the neighborhood/community may improve health, development, and wellbeing in
Latino children.
Pediatric obesity is an important public health issue. Targeted efforts to curb child obesity rates
are necessary, especially among Latino children, as this sub-group is more likely to become
overweight before entering elementary school than children of other ethnic groups.
11
Obesity in
Latino children increases health risk factors and can also impact school performance.
11,54
A main contributor of overweight and obesity in Latino children may be their limited access to
healthy food. See the full Salud America! research review on Latino children and healthy food
access here.
10
Some recent study results appear mixed on this issue. Although fast-food consumption does
occur in Latino children, one study found that their caloric intake from fast food was comparable

9 Salud America! https://salud-america.org/
or lower than in other racial and ethnic groups, except for Asians.
55
Another study found that
soda and unhealthy snacks were commonly available in Latino households, but so were fresh
fruits and vegetables, and Latino preschool children also consumed fruits and vegetables more
frequently than black children.
56
These findings are somewhat contrary to those of another study
of primarily Latino and black children living in rural, low-income families in the Southeast US that
found lower consumption of fruits among Latinos compared with black children.
57
Many factors
appear to contribute to intake of fruits and vegetables, as another study of older Latino children
(ages 10-14) found that few of the participating children (N = 181) met the dietary
recommendations regard fruit and vegetable consumption and other nutritious food.
58
Access to
culturally-relevant healthy foods is also a factor. In a study of grocery stores in Latino and black
neighborhoods, most stores carried fewer than 50% of fruits and vegetables that were
considered culturally specific and commonly eaten by these populations.
59
Poverty and food
insecurity may play a contributing role as well,
60
as may parenting issues such as stress and
depression that may affect parental feeding practices.
61
Other issues such as cultural beliefs may influence the types of foods eaten. Many Latinos
believe they are lactose-intolerant and often avoid dairy products to reinforce this belief;
however, this culturally-specific eating preference may lead to deficiencies in micronutrients
such as calcium, potassium, and vitamin D. Optimal levels of these micronutrients are thought
to reduce the risk of heart disease, metabolic syndrome, and type 2 diabetes.
62
Because poor nutrition and obesity in Latino children is due to complex sociocultural reasons, a
broad approach to improving eating habits may be effective, especially when it includes
extended family networks, school, and community activities.
63
Addressing parent feeding
practices is necessary to empower Latino parents to offer healthier food choices at meal times
and snacks in the home environment. Parents should be encouraged to eat family meals
together to model healthy eating habits and to avoid TV during meals.
56
Early care and education (ECE) is an emerging setting for obesity-prevention via healthy
lifestyles. The use of ECE facilities—including child care centers, day care homes, Head Start
programs, preschool and pre-kindergarten programs—has become a norm in the U.S.
64
A
successful program, Color Me Healthy, demonstrated positive health outcomes in young
children as they learned about healthy eating and exercise in active ways, including interaction
with peers and parents. Additional programs that have been successful include Brocodile the
Crocodile, Eat Well Play Hard, and Hip Hop to Health, Jr.
65
Any program implemented,
however, should be modified as needed for cultural relevancy.
63
Several organizations play a central role in improving healthy eating in Latino children, including
schools, WIC, Head Start early child care programs, and churches. Community programs are
also effective. LA Sprouts, a 12-week hands-on nutrition/cooking and gardening curriculum was
pilot-tested with 104 Latino children (59% obese), with a control group, to increase knowledge
and skills on gardening, nutrition, and cooking.
66
The curriculum was developed to be culturally-
and age-appropriate for urban, Latino upper elementary children. At the end of the pilot test,
intervention children had significantly lower diastolic blood pressure and greater fiber intake
compared with controls; those who were overweight at baseline also had decreases in BMI and
weight gain compared with controls who were overweight. Another pilot study (led by a Salud
America! grantee) tested a community-based garden, nutrition, and cooking program, Growing
Healthy Kids, with a 60-percent Latino cohort of 120 children and their families. The study found
that 17% of overweight/obese children achieved an improved BMI classification. According to
parents’ reports, children ate two more servings of fruit per week and almost five more servings
of vegetables per week.

10 Salud America! https://salud-america.org/
At the federal level, funding is allocated to schools to offer healthy breakfasts and lunches to
children who are on free or reduced meals, in which Latinos are more likely to qualify for than
white children. States with stronger nutrition standards are better able to reduce obesity among
children in free and reduced lunch programs. More innovative programs to improve nutrition in
schools include better vending machine choices and more nutritious a la carte items.
67
Other
federally-funded programs—such as Supplemental Nutrition Assistance Program (SNAP),
Supplemental Nutrition Program for Women, Infants, and Children (WIC), Summer Food
Service, Head Start, and Child and Adult Care Food Program (CACFP)—may also help to
improve nutrition and access to healthy food in Latino children (see
https://www.nutrition.gov/food-assistance-programs
for more information);
68
importantly,
however, undocumented immigrant Latinos would not qualify for these programs and may need
help from other sources, such as emergency food assistance programs.
69
Latino children have limited access to active spaces—such as trails, parks, and
recreation facilities—that may prevent them from engaging in adequate levels of physical
activity for healthy development. Improving access to active spaces that promote
physical activity may improve health and wellbeing.
Many studies have found that U.S. Latino children have inadequate access to active spaces.
70–
75
One study of three diverse U.S. regions found that only 19 percent of Latino neighborhoods
had recreational facilities, compared with 62 percent of white neighborhoods.
76
Similar results
were found when looking specifically at neighborhood socioeconomic level, where children of
racial/ethnic minorities living in poverty had less access to active spaces than children living in
more advantaged neighborhoods.
77
Interestingly, national data found that Latino neighborhoods
were actually closer to parks but farther from green spaces than non-Latino neighborhoods,
78
so
more research may be needed to determine if and how the type of active space influences
physical activity levels.
Inadequate access to physical activity sites has been linked to low levels of physical activity
among Latino children.
79,80
In one study of children (66% Latino) living in East Harlem, NY,
nearly 80 percent of the Latino participants had no access to active spaces, and those living in
areas with fewer active sites spent less time engaging in physical activity. Therefore, increasing
access to active spaces in underserved areas may help to promote physical activity among
youth living there.
79,81,82
The Healthy People initiative developed by the U.S. Department of Health and Human Services
aims to increase youth access to active spaces by improving the built environment (e.g., adding
sidewalks, bike lanes, trails, and parks) and increasing access to physical activity facilities.
83
Other initiatives are underway in a number of U.S. cities, many of which have predominantly
Latino communities. These include shared and open use policies, where schools and other
entities partner to share school recreational facilities with the public; outdoor learning
environments or green schoolyards, where early care facilities and schools include gardens and
natural elements in the playscape; Open Streets programs, where streets are closed to
motorized traffic allowing for safe use by residents for walking, bike riding, etc; “rails-to-trails”
projects, where inactive railroad tracks are converted into bike paths and parks in a number of
U.S. cities; opens space plans, which aim to improve access to trails and green space;
Complete Streets policies, which call for roadways to be safe and convenient for people of all
ages, whether walking, biking, driving, or riding transit; Vision Zero strategies,
84
which aim to
eliminate traffic fatalities and serious injuries; and other initiatives.
71,85–90

11 Salud America! https://salud-america.org/
The design and development of communities can make it easier or more difficult for families to
be active on a daily basis. The National Physical Activity Plan highlights several methods to
increase families’ opportunities for incidental physical activity:
91
• Effective land use policies can put common destinations with walking and biking
connections near where families live, to increase active transportation as well as access
to vital community services.
• Community planners can integrate considerations for non-motorized travel and public
health into formalized planning processes, such as master plans, comprehensive plans,
zoning code updates, housing and commercial developments, metropolitan planning
organizations' (MPO) transportation improvement project lists, trail plans, and regional
transportation plans, with specific focus on improving environments in low-income
communities.
• Transportation spending can be reformed to tie it to larger goals for health, safety,
equity, and the environment—rather than to a focus only on traffic volumes and speeds.
Healthcare providers also play in important role in promoting physical activity. There is little
research on how effective physical activity counseling and prescriptions are to increase physical
activity levels among Latinos, but some studies show that asking patients about physical
activities levels is associated with weight loss, improved glucose control in diabetic patients and
increased physical activity among cancer survivors.
92
Additionally, physicians who are physically
active themselves are more likely to counsel more frequently and more effectively about the
importance of physical activity to their patients.
93,94
The National Physical Activity Plan highlights
the need for healthcare systems to integrate physical activity as a patient “vital sign” into
electronic health records for all healthcare providers to assess and discuss physical activity with
their patients.
91,92
Tobacco use, for example, was adopted as a vital sign 60 years ago. After
smoking, physical inactivity is the leading risk factor for predicting if a person will die early.
95
Healthcare systems should also support the capacity of school-based health clinics and early
learning programs to promote physical activity. Additionally, schools, childcare centers, and
early childhood facilities can adopt standards to ensure children are appropriately physically
active and to develop outdoor learning models to integrate physical activity, natural settings, and
education.
See the full Salud America! research review on Latino children and active spaces here.
89
Latino children have low participation in high-quality preschool programs and face
educational disadvantages when starting kindergarten.
Although Latino children may be of similar weight at birth and equally able to thrive in the first 2
years of life compared with white children,
96
their ability to reason and remember tasks
(cognitive processing skills), verbally communicate, and identify letters, numbers, and shapes
(preliteracy skills) lessens significantly by age 24 months, and these disparities appear even
more prevalent in Mexican-American children than in other Latino subgroups.
1
In general, a 15- to 25-percentage point gap exists for Latino children relative to their white
peers.
97
Children who start behind in kindergarten often stay behind. See more in the full Salud
America! research review on building support for Latino families.
98
Causes for cognitive, preliteracy, and oral communication gaps in Latino children are
multifactorial. Among the most common are poor education, large family sizes, low employment
or having multiple jobs, and depression among Latina mothers. These factors have been

12 Salud America! https://salud-america.org/
suggested to reduce the likelihood that Latino parents would engage their children in preliteracy
activities or read books to them, both very important activities leading to literacy and school
readiness.
1,99,100
Although most Latino parents are bilingual or can speak English fairly well,
some do not have a good command of the English language, which may decrease their
likelihood of reading or telling stories to their children in English, compared with white
parents.
100,101
Additionally, cultural beliefs that teachers are the experts in these areas, coupled
with limited parental education, may deter Latino parents from engaging their child in preliteracy
activities.
Participation in preschool programs is also suboptimal in Latino children and is a main
contributor to poor school readiness.
5,6
In recent years, several programs have been set forth to
improve kindergarten readiness and create a trajectory of academic achievement, employment,
and increased earnings for disadvantaged Latino children.
In the United States, almost 70% of 4-year-old children go to early learning centers.
102
However, nearly six of every 10 4-year olds are not enrolled in publicly funded preschool
programs, and even fewer are enrolled in the highest-quality programs. Participation is
particularly low for Latino children, at 40% compared to 53% of white children. Participation is
also low for low-income children, at 41% compared to 61% of their more affluent peers.
7
Lack of participation in early care and education programs may stem from lack of availability. In
a study about the location of child centers across eight states, 42% of children younger than age
5 live in areas known as child care deserts, which either have no child care centers or so few
centers that there are more than three times as many children as there are spaces in centers.
103
The availability of child care centers is in a state of crisis for Latino families. Several elements
are critical for the ideal child care center:
• High-quality early childhood education centers should be more affordable and accessible
to low-income Latinos, with higher density in Latino neighborhoods.
104
• Early childhood education centers should offer services from birth through age 5 to allow
single-site care of all children within one family, and continuity of cognitive assessments
and interventions.
104
• The location and design of early learning centers can support active transport and
increased student physical activity throughout the school day.
91
• Students who have access to nature at school engaged in physical activity 10 times
longer than those students who had limited access to nature at school.
105
Outdoor
learning environments and green schoolyards, for example, can boost student’s
academic performance, physical activity, mental health, and different types of play,
which are critical for development.
• The American Academy of Pediatrics (AAP) states that unstructured free play is
essential for children’s emotional development and can protect against stress, anxiety
and depression in children.
106
More information about families’ proximity to child care programs can inform local, state and
federal efforts to increase access to early childhood programs, especially given the financial
impact of early care and education programs. Only 14% of public education dollars are spent on
early childhood education, yet for every $1 spent expanding early learning, society receives a
return on investment of $7 or more based on increased school and career achievement, as well
as reduced costs in remedial education, health, social welfare programs, and criminal justice
system expenditures.
5,7,107,108

13 Salud America! https://salud-america.org/
Family-, preschool-, and community-based interventions may help to improve school
readiness and lead to better developmental outcomes for Latino children.
Many children attend Head Start programs, which were founded to promote school readiness
for children of low-income families. In recent years, the Head Start curriculum has been
challenged to enhance children’s language and preliteracy skills using interactive reading with
active discussions. One of these programs, the Research-based, Developmentally Informed
(REDI) classroom intervention, uses evidence-based curricula that center on preschool
attainment of language, preliteracy, and social-emotional skills considered essential for later
achievement. In a study of 356 children (17% Latino) enrolled in Head Start programs, children
exposed to the REDI intervention had significantly improved vocabulary and social-emotional
skills compared with those who were not exposed to the REDI intervention,
109
and these skills
were sustained throughout kindergarten.
110
REDI-P, the parent program of the REDI, was
introduced to teach parents to engage their children in directed talk and play sessions and
included bi-weekly home visits. In two randomized controlled trials (N = 200, 19% Latino;
111
N =
556, 19% Latino);
102
children exposed to both REDI and REDI-P showed significant gains in
literacy and social-emotional skills compared with children not exposed to both interventions,
and these gains were sustained into kindergarten
112
and second-grade, with improved
classroom participation, student-teacher interactions, and friendships.
102
Another randomized
study (N = 200; 20% Latino) showed similar findings but also found that REDI-P was
augmented by pre-intervention parental support for learning, with children receiving greater
baseline parental support faring better, suggesting that parental support is a key contributor to
child learning in preschool programs.
112
The Miami School Readiness Project (MSRP) was a large public preschool program that
examined the effects of preschool curricula on kindergarten readiness in 7,045 Latino children
(and 6,700 black children).
113
The program involved the use of two different curricula: the more
conventional and widely used High/Scope curriculum, which balances child-initiated and
teacher-directed activities in small- and large-group settings, and the Montessori curriculum,
which individualizes learning to each student and fosters independent, child-directed learning
with fewer teacher-directed activities. Although all children made progress in pre-academic,
socioemotional, and behavioral skills regardless of curriculum, the Montessori program
appeared to be more beneficial for Latino children who, despite being at the highest pre-
academic and behavioral risk at baseline, finished the preschool year with test scores above the
national average. One potential reason that the Montessori program was such a success in
Latino children is that it incorporates a child’s culture into the classroom, which some say is
essential for preschool success in Latino children. And, since black children seemed to fare
better in the High/Scope program, these data suggest that preschool curricula should be tailored
to racial, ethnic, and cultural differences. It has also been suggested that Montessori teachers
may be more educated and more culturally aware than teachers of other preschool programs,
which may be another contributor to the positive findings in this study.
The Little by Little (LBL) program is a bilingual literacy promotion and supplemental nutrition
program provided as part of the WIC program. In LBL, parents receive brief counseling on the
importance of reading to and verbally interacting with their children, handouts on developmental
milestones and appropriate interaction methods for promoting optimal child development, and
an age-appropriate children’s book or toy for use during parent-child interactions. Reading
materials are provided in English or Spanish, depending on the family’s primary language. LBL
was implemented in Los Angeles, California, in 118,000 3- to 4-year-old, predominantly Latino
(92%) children in the WIC program; its effectiveness on kindergarten readiness was evaluated
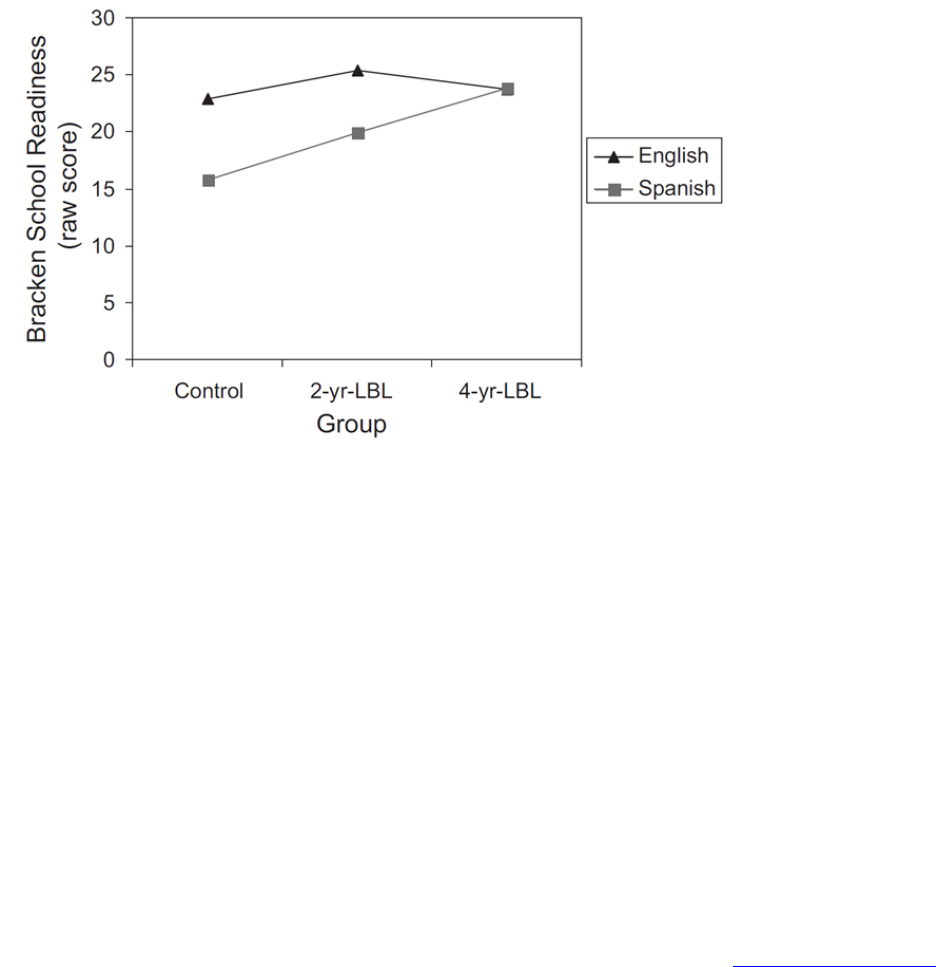
14 Salud America! https://salud-america.org/
by randomly selecting WIC families and dividing them into three groups based on their exposure
to the intervention: no intervention, 2-year intervention, and 4-year intervention.
100
Parents in the
intervention groups received the intervention when children were 2 years old (2-year
intervention) or when the mothers were in their third trimester of pregnancy (4-year
intervention). Although no significant differences were observed between intervention groups
among English-speaking families, Spanish-speaking families received significant benefit from
the intervention. Children in both intervention groups were significantly more prepared for
kindergarten (measured by Bracken School Readiness score) than those in the no intervention
group, with the 4-year group receiving the greatest benefit (Figure 2). The program also
improved the awareness in Spanish-speaking parents of the importance of promoting early
reading and verbal interaction with their children and providing a literature-rich home
environment to improve their child’s literacy skills and school readiness.
Figure 2. Effect of LBL Intervention vs Control on School Readiness in English- and Spanish-
Speaking Preschool Children
100
ParentCorps, another preschool program that involves both school-based and parenting-
centered interventions, aims to promote safe, nurturing, and predictable environments for
children. The program involves professional development for preschool teachers and parent
counseling administered by teachers and mental health professionals during after-school hours.
ParentCorps was evaluated in a randomized study of 4-year-olds (N = 1050; 9.8% Latino) from
99 preschool programs in New York City.
114
By second grade, children in this program had
fewer mental health problems, better student-teacher interactions, and higher academic
performance than peers who did not receive this intervention. Other examples of interventions
aimed at improving school readiness in Latino children include home visits, “Zero to Three”
programs, Pre-K 4 San Antonio, and First 5 LA.
2,115–118
Latino men are often less willing to talk about their problems, like parenting insecurities or health
issues, which can result in decreased engagement in their children’s life and decreased
attendance in parenting programs, which may hinder early childhood development. Researchers
in New York created a parenting class for 126 low-income, Spanish-speaking Latino dads, but
framed it as an academic-readiness program for children.
119
The eight-week training
intervention, which revolved around shared book reading, increased Latino dads’ parenting

15 Salud America! https://salud-america.org/
skills by 30 percent, and increased Latino children’s language development and school
readiness by 30 percent. Additionally, the 79-percent parent attendance rate was high,
researchers indicated. The finding suggests it is critical to develop culturally relevant, engaging,
and sustainable parenting interventions for Latino fathers.
Teaching social and emotional skills can also have an impact on student’s academic
development. Social and emotional learning is “the process through which children and adults
acquire and effectively apply the knowledge, attitudes, and skills necessary to understand and
manage emotions, set and achieve positive goals, feel and show empathy for others, establish
and maintain positive relationships, and make responsible decisions,” according to a Penn State
and Robert Wood Johnson Foundation report.
120
The report indicates that, when learned early,
social and emotional skills can help children overcome challenges and avoid unhealthy
behavior, improving a variety of outcomes into adulthood, and have significant economic impact
for individuals and society overall. The report cites research that indicates that students with
strong social and emotional skills: do better in school; are more likely to graduate college and
get a well-paying job; support healthy functioning and help people avoid problems like crime and
substance use; and have a greater likelihood for long-term success as an adult. Another report
indicates that evidence-based programs can optimize the teaching of social and emotional skills
in preschool through professional development for teachers, apparent involvement, and
integration with academic enrichment initiatives, which can spur greater benefits for children
with delays in social-emotional skill development associated with early socioeconomic
disadvantage.
121
Much of the Latino-focused research in this area specifically involves social and emotional
development in Spanish and English dual language learners.
122
Still, one study found that
teaching social and emotional skills to inner-city students contributes to their academic
achievement. The study involved all students enrolled in regular or bilingual education in an
inner-city school system where 2 out of 3 students qualified for a free or reduced price lunch
and 9 out of 10 students were black or Latino.
123
Another study found that classroom programs
designed to improve elementary school students’ social and emotional skills can also increase
reading and math achievement, even if academic improvement is not a direct goal of the skills
building. The benefit held true for students who qualified for free and reduced-priced lunch.
124
Early childhood development programs that have long-term social and emotional
development benefits for other minority and low-income children also likely benefit
Latino children.
Children who participate in high-quality early care and education (ECE) programs experience a
range of immediate and long-term cognitive and health benefits, with the greatest impact seen
in low-income populations.
98
Although extensive literature is available on the long-term effects of Head Start and other early
childhood development programs on black and white children, the effects of these programs on
Latino populations have mostly been ignored.
125
Additionally, nearly 40 years ago, it was
recognized that cultural differences exist among the different Spanish-speaking people and that
different subgroups should be analyzed separately. However, early data from Head Start
centers tended to combine all Latinos into one group.
125,126
From the available data, providing Spanish language in preschools was shown to enhance
Latino and non-Latino education as far back as the 1980s, and current recommendations
believe that Spanish language and culture should be instituted in preschool programs serving

16 Salud America! https://salud-america.org/
Latino communities.
126–128
The Head Start Curriculum is mandated to have at least one Spanish-
speaking educator, and that educator should be able to understand a Latino child’s culture and
heritage.
125
Although long-term effects of the Head Start program were not documented for
individual children or for Latinos specifically, an overall cost-benefit impact was found in social,
emotional and health outcomes.
129–132
White children who attended Head Start were more likely
to complete high school and attend college than their siblings who attended regular preschools.
For black children, there were less significant educational gains from attending Head Start
versus a regular preschool, but a decrease in criminal activity was observed.
133
The long-term effects of other preschool and elementary programs on low-income, but not
necessarily Latino, populations are mentioned herein to sort out factors that led to successful
outcomes in children attending these programs. The Child-Parent Center program in Chicago
provides educational enrichment through school- and family-based services from preschool to
third grade. In this program, parent involvement was mandatory, teachers interacted with
parents directly, and classroom sizes were small, all of which contributed to its success.
134
Compared with children who did not participate in the program, those who participated in the
preschool phase of the program were more likely to graduate high school, attend a 4-year
university, and have more overall years of education. Those participating in the preschool and
grade school phases had higher rates of full-time employment and educational attainment.
Other long-term benefits of the program included increases in attainment of health insurance,
reductions in depression and disability, and reductions in criminal activity and arrests.
The High/Scope Perry Preschool Program was implemented for 123 low-income black children
who were followed up from preschool to age 40. Those participating in the program showed less
criminal activity, greater earnings, higher rates of high school graduation, and higher IQs
compared with those who did not.
135
The Project STAR program enrolled children between
kindergarten and third grade and showed that improved test scores, and higher earnings,
college attendance, home ownership, and 401(k) savings at age 27, were due to noncognitive
skills learned in high-quality kindergartens. They also showed that smaller and better classroom
environments for grades 5-8 resulted in marked long-term benefits even without earlier
intervention and that students from smaller classes (13-17 children vs 20-25 children) were
more likely to attend college.
136
Finally, the Abecedarian Project cared for and educated children
from as young as 6 weeks to 8 years. Enrollment in the program led to better educational gains,
mixed economic benefits, and no difference in social-emotional measurements compared with
not being enrolled in the program.
137
Taken together, the most successful elements in these studies—smaller class sizes, more
parent involvement, and better-educated teachers—would likely benefit Latino children as well,
if implemented in Latino-focused programs. Importantly, these programs were more expensive
to run than the Head Start programs.
Latino families share many common values—such as familism and marianismo—that
may benefit Latino childhood development and influence early childhood development
programs.
Children begin to develop their social and emotional skills through initial interactions with family.
Through strong and consistent relationships, they learn the importance of social bonding,
connecting to others with empathy, and self-regulating emotions. Young children begin to learn
about complex social interactions by receiving responsive caregiving from parents, which often
leads to positive outcomes later in life. One study (N = 7,750; 19% Latino) found that although
Latino children may demonstrate cognitive gaps compared with white children after age 1, their
social-emotional health rivals that of white children, even when raised in lower-income families.
1

17 Salud America! https://salud-america.org/
These findings suggest that social and emotional health of Latinos develops on an independent
pathway. One potential reason is the parenting style among Latina mothers, which can be
characterized as warm and nurturing. Latina mothers are typically very responsive to their
children, and report fewer depressive symptoms than white mothers, which could be allowing for
stronger connectedness with their children.
Common values can be found among most Latino families.
• The concept of family, or familismo, is extremely important to many Latinos. Family
needs come before individual needs, and this is evident in Latinos’ desire to center many
activities around the extended family.
138
Due to economic circumstances, Latino
households may be large and include members of the extended family, which can be
stressful in some cases and helpful in others, especially regarding childrearing.
• Traditional gender roles, machismo and marianismo, are often practiced in Latino
families, especially in low-income families.
139,140
Machismo refers to the idea that the
father is the head of the household, strong protector, and authority figure, whereas
marianismo means the mother is self-sacrificing, religious and responsible for raising the
children and maintaining the house.
141
• Religion is also a cornerstone of the family and influences many beliefs and decisions
within the family.
142
Most Latinos in the U.S. practice Catholicism, but practices within
that faith may differ depending on the country of origin.
143
Because religion has been a
part of Latino culture for so long, religious beliefs are difficult to separate from cultural
values and often guide Latinos in many areas of life, even if they are not practicing
religion.
142
Many of these common qualities of Latino families—strong familial bonds, religious and cultural
values, protective fathers and nurturing mothers—are beneficial for the development of Latino
children and should be considered in early childhood education and development programs.
Educators and community organizations should target programs to the entire family, including
the extended family when feasible, and to mothers as caregivers and fathers as important
decision-makers. Coordination with local religious institutions is also important to ensure that
religious beliefs and cultural values are considered in program development.
144,145
Programs and policies providing maternal and breastfeeding support and family support
services promote healthy social and emotional development and overall wellbeing in
Latino children.
Although Latino children are generally well adjusted socially and emotionally, several factors
may negatively influence their overall health and wellbeing development. These include poverty
and/or large households, immigration status, the country of origin, maternal depression,
1,146,147
as well as other factors like breastfeeding initiation and duration.
148
Read the Salud America! research review about breastfeeding among Latina mothers.
148,149
Approaches are emerging on how to address these issues. For example, mental health
interventions can be made available to Latina mothers who are displaying negative thought
patterns, including anxiety, depression, and self-doubt.
150
Providing outlets for mothers to talk
with peers and trained counselors and/or nurses may help to reduce stress and improve
intrapersonal awareness toward mental health and its effects on family and childrearing. In
particular, home-based interventions have been successful in this population.
129,130128,129
The
Latino family typically includes extended relatives, and sometimes friends, which may lead to
several people living in one household. Latina mothers may shoulder many responsibilities

18 Salud America! https://salud-america.org/
because of the family structure. Involving family members, especially partners, in helping with
household responsibilities, including children’s activities, may reduce the load that mothers carry
in this culture.
127
Read the Salud America! research review about mental health and Latino
children.
33
Similarly, parent education classes could be offered to Latino parents to reinforce styles that are
responsive, positive, and warm. Innovative approaches may include meeting with families in the
home environment and learning about the challenges that exist from living with extended
families, often in small areas. Addressing specific parenting skills, such as skill encouragement,
monitoring discipline, and positive involvement), may be beneficial to immigrant parents.
131
Read
the Salud America! research review about building support for Latino families.
98
Conclusions and Policy Implications
Conclusions
Latino children are at increased risk of poor outcomes in many areas of early childhood
development. Factors such as socioeconomic status, parenting behaviors, family structure and
environment, childhood experiences, and access to early education programs and health
services can influence many aspects of child development. High-quality preschool programs,
parent-directed support and education, and family-, school- and community-based programs
have all been shown to improve developmental outcomes in Latino children. Preventing,
identifying, and helping children and families overcome ACEs can impact a child’s social
emotional development and chances of school success. Additional resources are needed to
develop new, culturally appropriate programs and policies and/or improve upon those already in
place, to further support Latino children in their formative years and beyond.
Policy Implications
To address adverse childhood experiences (ACEs) among Latino children:
• Improve access to home visits for Latino families by engaging community advocates,
civil rights organizations, and other stakeholders who understand the needs in their
communities; ensure that home visit programs are equitable and culturally sensitive to
the needs of Latinos.
• Strengthen the childcare workforce through training to provide trauma-informed care for
ACEs.
• Increase awareness of and support for the medical home system of care for Latino
children that can help to identify and address ACEs and other health-related issues
early.
• Increase collaboration between child welfare agencies and early intervention programs
to provide mental health services to children experiencing difficulties due to ACEs.
• Develop culturally sensitive programs, policies and interventions considering Latino
family structure and dynamics.
• Allocate funding for early-life interventions including prenatal care and parent education
and support to prevent ACEs in at-risk families.
To extend the benefits of early care and education (ECE) and preschool programs:
• Promote access to and availability and awareness of preschool and early childhood
education programs, especially for Latino children given the lower participation rates, to
better address the cognitive gaps prevalent in this group.

19 Salud America! https://salud-america.org/
• Incorporate culturally-relevant parent counseling, education, and support into all
preschool programs.
• Reduce classroom sizes to promote greater teacher-student interaction and
individualized education.
• Implement culturally-sensitive teacher education and training, especially targeted to
overcoming poor school readiness among Latino children.
• Increase parent involvement in classrooms and home visits by educators to ensure
reinforcement of preliteracy activities in the home.
• Ensure that at least one Spanish-speaking educator is present at preschools teaching
Latino children.
• Support adoption of school design strategies to support active transport and increased
student physical activity throughout the school day, such as outdoor learning
environments or green schoolyards.
To improve Latinos’ access to healthy food:
• Allocate funding to support community-based initiatives that improve access to grocery
stores, health food stores, and farmers’ markets in Latino communities.
• Partner with farmers’ markets to develop long-term strategies for improving access to
fresh fruits and vegetables in Latino communities.
• Increase access to culturally-appropriate healthy eating interventions and educational
programs or activities (i.e., gardening) for Latino children and their families.
• Improve Latinos’ access to school-, community-, and government-based food programs.
To increase Latinos’ access to physical activity spaces and opportunities:
• Improve access to active spaces (parks, trails, green space, recreation sites) in Latino
communities.
• Solicit community feedback to strengthen the development of new recreation sites and
improvements in the built environment.
• Implement Complete Streets transportation projects near affordable housing, schools,
grocery stores, and recreation sites to improve active travel to those sites.
• Construct affordable housing near public transit, employment centers, schools, grocery
stores, and parks.
• Improve outdoor learning environments and green schoolyards at childcare centers and
schools.
• Integrate considerations for non-motorized travel and public health into formalized
planning processes, such as master plans, comprehensive plans, zoning code updates,
housing and commercial developments, metropolitan planning organizations' (MPO)
transportation improvement project lists, trail plans, and regional transportation plans,
with specific focus on improving environments in low-income communities.
• Reform transportation spending at all levels to tie it to larger goals for health, safety,
equity, and the environment—rather than to a focus only on traffic volumes and speeds.
To improve Latinos’ healthcare access:
• Incorporate assessment of patients’ childhood history in routine primary care visits to aid
in the identification of presence or risk of ACEs, and implement culturally and
linguistically relevant interventions.
• Advocate for early developmental-behavioral surveillance and screening, according to
the American Academy of Pediatrics recommendations.
• Provide home visiting to ensure parents and caregivers have the time, knowledge, and
resources needed to ensure proper childhood development.

20 Salud America! https://salud-america.org/
• Incorporate physical activity as a patient “vital sign.”
• Support the capacity of school-based health clinics and programs to promote healthy
eating and physical activity.
Future Research Needs
Further research is needed to identify the barriers to healthy eating in Latino children and
evaluate current and new strategies for improving access and adherence to a healthy diet.
Studies should also aim to identify the determinants of ACEs in Latino families and evaluate
interventions for preventing ACEs and/or mitigating their harmful effects. The use of
administrative data, such as Medicaid claims and other service records, may be useful for these
studies and may help to target prevention and early intervention for children with or at risk of
ACEs. More research is needed to identify the barriers to and predictors of mental health
service use among Latino youth and develop the necessary assessment and counseling tools to
identify at-risk Latino youth. More research is needed to identify the barriers to preschool
participation and in-home preliteracy activities to inform the development of targeted in-home
interventions to improve school readiness in Latino children. Accurate census data is also
critical to ensure equitable distribution of funding for early educational programs, healthcare,
safe places to walk and play, access to healthy food, and maternal and breastfeeding
support. Additionally, further research is needed to evaluate the short- and long-term effects of
existing preschool programs, such as Head Start, REDI, and MSRP, especially for Latino
children, since this information is currently lacking. Finally, more research is needed to
determine parent and teacher qualities that lead to educational success in Latino children and to
evaluate strategies that promote the development of these qualities in Latino parents and
teachers who teach Latino children.

21 Salud America! https://salud-america.org/
References
1. Guerrero, A. D. et al. Early Growth of Mexican–American Children: Lagging in Preliteracy
Skills but not Social Development. Matern. Child Health J. 17, 1701–1711 (2013).
2. Krogstad, J. M. Hispanics only group to see its poverty rate decline and incomes rise. Pew
Research Center (2014).
3. Proctor, B., Semega, J. & Kollar, M. Income and Poverty in the United States: 2015.
(2016). Available at: https://www.census.gov/library/publications/2016/demo/p60-256.html.
(Accessed: 25th January 2017)
4. Isaacs, J. B. Starting School at a Disadvantage: The School Readiness of Poor Children.
Brookings (2001).
5. US Department of Education. A Matter of Equity: Preschool in America. (2015).
6. Yoshikawa, H. et al. Investing in our future: The evidence base on preschool education.
(Society for Research in Child Development, 2013).
7. White House Initiative on Educational Excellence for Hispanics. Early Learning: Access to
A High Quality Early Learning Program. Available at: https://sites.ed.gov/hispanic-
initiative/files/2014/05/WHIEEH-Early-learning-Fact-Sheet-FINAL_050614.pdf. (Accessed:
25th October 2017)
8. Braveman, P., Egerter, S., Arena, K. & Aslam, R. Early Childhood Experiences Shape
Health and Well-Being Throughout Life. (Robert Wood Johnson Foundation, 2014).
9. Bright, M., Knapp, C., Hinojosa, M., Alford, S. & Bonner, B. The Comorbidity of Physical,
Mental, and Developmental Conditions Associated with Childhood Adversity: A Population
Based Study. Matern. Child Health J. 20, 843–853 (2016).
10. Perry, A., Patlak, M., Ramirez, A. G. & Gallion, K., J. Making Healthy Food and Beverages
the Affordable, Available, Desired Choices Among Latino Families. (2015).
11. Liu, G. C., Hannon, T., Qi, R., Downs, S. M. & Marrero, D. G. The obesity epidemic in
children: Latino children are disproportionately affected at younger ages. Int. J. Pediatr.
Adolesc. Med. 2, 12–18 (2015).
12. Galindo, C. & Fuller, B. The social competence of Latino kindergartners and growth in
mathematical understanding. Dev. Psychol. 46, 579–592 (2010).
13. Child Trends. Dissemination of Child Trends report: “The Invisible Ones: How Latino
Children Are Left Out of Our Nation’s Census Count”. Child Trends
14. Newton, J. Prevention of mental illness must start in childhood: growing up feeling safe
and protected from harm. Br J Gen Pr. 65, e209–e210 (2015).
15. Robert Wood Johnson Foundation. Early Childhood Experiences Shape Health and Well-
Being Throughout Life. (2014).
16. Lucenko, B. A., Sharkova, I. V., Huber, A., Jemelka, R. & Mancuso, D. Childhood adversity
and behavioral health outcomes for youth: An investigation using state administrative data.
Child Abuse Negl. 47, 48–58 (2015).
17. Bright, M. A., Alford, S. M., Hinojosa, M. S., Knapp, C. & Fernandez-Baca, D. E. Adverse
childhood experiences and dental health in children and adolescents. Community Dent.
Oral Epidemiol. 43, 193–199 (2015).
18. Burke, N. J., Hellman, J. L., Scott, B. G., Weems, C. F. & Carrion, V. G. The impact of
adverse childhood experiences on an urban pediatric population. Child Abuse Negl. 35,
408–413 (2011).
19. Flaherty, E. G. et al. Adverse Childhood Experiences and Child Health in Early
Adolescence. JAMA Pediatr. 167, 622–629 (2013).
20. Jimenez, M. E., Wade, R., Schwartz-Soicher, O., Lin, Y. & Reichman, N. E. Adverse
Childhood Experiences and ADHD Diagnosis at Age 9 Years in a National Urban Sample.
Acad. Pediatr. 17, 356–361 (2017).

22 Salud America! https://salud-america.org/
21. Kerker, B. D. et al. Adverse Childhood Experiences and Mental Health, Chronic Medical
Conditions, and Development in Young Children. Acad. Pediatr. 15, 510–517 (2015).
22. Mersky, J. P., Topitzes, J. & Reynolds, A. J. Impacts of adverse childhood experiences on
health, mental health, and substance use in early adulthood: A cohort study of an urban,
minority sample in the U.S. Child Abuse Negl. 37, 917–925 (2013).
23. Pretty, C., O’Leary, D. D., Cairney, J. & Wade, T. J. Adverse childhood experiences and
the cardiovascular health of children: a cross-sectional study. BMC Pediatr. 13, 208
(2013).
24. Thompson, R. et al. Trajectories of Adverse Childhood Experiences and Self-Reported
Health at Age 18. Acad. Pediatr. 15, 503–509 (2015).
25. Caballero, T. M., Johnson, S. B., Buchanan, C. R. M. & DeCamp, L. R. Adverse Childhood
Experiences Among Hispanic Children in Immigrant Families Versus US-Native Families.
Pediatrics e20170297 (2017). doi:10.1542/peds.2017-0297
26. Llabre, M. M. et al. Childhood Trauma and Adult Risk Factors and Disease in
Hispanics/Latinos in the US: Results From the Hispanic Community Health Study/Study of
Latinos (HCHS/SOL) Sociocultural Ancillary Study. Psychosom. Med. 1 (2016).
doi:10.1097/PSY.0000000000000394
27. Wing, R., Gjelsvik, A., Nocera, M. & McQuaid, E. L. Association between adverse
childhood experiences in the home and pediatric asthma. Ann. Allergy. Asthma. Immunol.
114, 379–384 (2015).
28. Isasi, C. R. et al. Association of Childhood Economic Hardship with Adult Height and Adult
Adiposity among Hispanics/Latinos. The HCHS/SOL Socio-Cultural Ancillary Study. PLOS
ONE 11, e0149923 (2016).
29. Campbell, F. et al. Early Childhood Investments Substantially Boost Adult Health. Science
343, 1478–1485 (2014).
30. Perez, N. M., Jennings, W. G., Piquero, A. R. & Baglivio, M. T. Adverse Childhood
Experiences and Suicide Attempts: The Mediating Influence of Personality Development
and Problem Behaviors. J. Youth Adolesc. 45, 1527–1545 (2016).
31. Martinez, J. I., Gudiño, O. G. & Lau, A. S. Problem-Specific Racial/Ethnic Disparities in
Pathways From Maltreatment Exposure to Specialty Mental Health Service Use for Youth
in Child Welfare. Child Maltreat. 18, 98–107 (2013).
32. Gudiño, O. G., Lau, A. S., Yeh, M., McCabe, K. M. & Hough, R. L. Understanding
Racial/Ethnic Disparities in Youth Mental Health Services: Do Disparities Vary by Problem
Type? J. Emot. Behav. Disord. 17, 3–16 (2009).
33. Ramirez, A. Mental Health & Latino Kids: A Research Review. Salud America (2017).
Available at: http://salud-america.org/healthymindsresearch/. (Accessed: 29th September
2017)
34. Ramos-Olazagasti, M. A., Bird, H. R., Canino, G. J. & Duarte, C. S. Childhood Adversity
and Early Initiation of Alcohol Use in Two Representative Samples of Puerto Rican Youth.
J. Youth Adolesc. 46, 28–44 (2017).
35. Allem, J.-P., Soto, D. W., Baezconde-Garbanati, L. & Unger, J. B. Adverse childhood
experiences and substance use among Hispanic emerging adults in Southern California.
Addict. Behav. 50, 199–204 (2015).
36. Walsh, E. G. & Cawthon, S. W. The mediating role of depressive symptoms in the
relationship between adverse childhood experiences and smoking. Addict. Behav. 39,
1471–1476 (2014).
37. Robert Wood Johnson Foundation. Traumatic Experiences Widespread Among U.S.
Youth, New Data Show. RWJF (2017). Available at: https://www.rwjf.org/en/library/articles-
and-news/2017/10/traumatic-experiences-widespread-among-u-s--youth--new-data-
show.html. (Accessed: 25th October 2017)

23 Salud America! https://salud-america.org/
38. American Academy of Pediatrics. Recommendations for Preventive Pediatric Health Care
Bright Futures. (2015).
39. Marks, K. P. et al. Systemwide Solutions to Improve Early Intervention for Developmental–
Behavioral Concerns. Pediatrics 136, e1492–e1494 (2015).
40. Davis, M. Home Visits Work: Let’s Make Them Universal. RWJF (2016). Available at:
http://www.rwjf.org/en/culture-of-health/2016/11/home-visits-make-them-universal.html.
(Accessed: 1st August 2017)
41. McKelvey, L. M., Whiteside-Mansell, L., Conners-Burrow, N. A., Swindle, T. & Fitzgerald,
S. Assessing adverse experiences from infancy through early childhood in home visiting
programs. Child Abuse Negl. 51, 295–302 (2016).
42. Garcia, C. et al. Development of Project Wings Home Visits, a Mental Health Intervention
for Latino Families Using Community-Based Participatory Research. Health Promot. Pract.
13, 755–762 (2012).
43. Balistreri, K. S. Adverse Childhood Experiences, the Medical Home, and Child Well-Being.
Matern. Child Health J. 19, 2492–2500 (2015).
44. McCarter, S., Jones, K. & Rager, K. M. Characteristics of Youth in the U.S. Receiving
Services From a Patient-Centered Medical Home (PCMH). Soc. Work Health Care 50,
595–605 (2011).
45. Bethell, C., Gombojav, N., Solloway, M. & Wissow, L. Adverse Childhood Experiences,
Resilience and Mindfulness-Based Approaches. Child Adolesc. Psychiatr. Clin. N. Am. 25,
139–156 (2016).
46. Casanueva, C., Smith, K., Ringeisen, H., Dolan, M. & Tueller, S. Families in need of
domestic violence services reported to the child welfare system: Changes in the National
Survey of Child and Adolescent Well-Being between 1999–2000 and 2008–2009. Child
Abuse Negl. 38, 1683–1693 (2014).
47. Ghosh Ippen, C., Harris, W. W., Van Horn, P. & Lieberman, A. F. Traumatic and stressful
events in early childhood: Can treatment help those at highest risk? Child Abuse Negl. 35,
504–513 (2011).
48. Kalmakis, K. A. & Chandler, G. E. Health consequences of adverse childhood experiences:
A systematic review. J. Am. Assoc. Nurse Pract. 27, 457–465 (2015).
49. Marie-Mitchell, A. & O’Connor, T. G. Adverse Childhood Experiences: Translating
Knowledge into Identification of Children at Risk for Poor Outcomes. Acad. Pediatr. 13,
14–19 (2013).
50. Merritt, D. H. & Klein, S. Do early care and education services improve language
development for maltreated children? Evidence from a national child welfare sample. Child
Abuse Negl. 39, 185–196 (2015).
51. Saltzman, W. R. The FOCUS Family Resilience Program: An Innovative Family
Intervention for Trauma and Loss. Fam. Process 55, 647–659 (2016).
52. Bartlettt, J. D., Smith, S. & Bringewatt, E. Helping Young Children Who Have Experienced
Trauma: Policies and Strategies for Early Care and Education - Executive Summary. (Child
Trends, 2017).
53. Bernal, G. & Domenech Rodríguez, M. M. Advances in Latino Family Research: Cultural
Adaptations of Evidence-Based Interventions. Fam. Process 48, 169–178 (2009).
54. Hollar, D. et al. Effect of a Two-Year Obesity Prevention Intervention on Percentile
Changes in Body Mass Index and Academic Performance in Low-Income Elementary
School Children. Am. J. Public Health 100, 646–653 (2010).
55. Vikraman, S., Fryar, C. D. & Ogden, C. L. Caloric intake from fast food among children and
adolescents in the United States, 2011-2012. NCHS Data Brief (2012).
56. Skala, K. et al. Ethnic Differences in the Home Food Environment and Parental Food
Practices Among Families of Low-Income Hispanic and African-American Preschoolers. J.
Immigr. Minor. Health 14, 1014–1022 (2012).

24 Salud America! https://salud-america.org/
57. Amuta, A. O., Jacobs, W., Idoko, E. E., Barry, A. E. & McKyer, E. L. J. Influence of the
Home Food Environment on Children’s Fruit and Vegetable Consumption: A Study of Rural
Low-Income Families. Health Promot. Pract. 16, 689–698 (2015).
58. Santiago-Torres, M., Adams, A. K., Carrel, A. L., LaRowe, T. L. & Schoeller, D. A. Home
Food Availability, Parental Dietary Intake, and Familial Eating Habits Influence the Diet
Quality of Urban Hispanic Children. Child. Obes. 10, 408–415 (2014).
59. Grigsby-Toussaint, D. S., Zenk, S. N., Odoms-Young, A., Ruggiero, L. & Moise, I.
Availability of Commonly Consumed and Culturally Specific Fruits and Vegetables in
African-American and Latino Neighborhoods. J. Am. Diet. Assoc. 110, 746–752 (2010).
60. Asfour, L. et al. Ethnicity, Household Food Security, and Nutrition and Activity Patterns in
Families With Preschool Children. J. Nutr. Educ. Behav. 47, 498–505.e1 (2015).
61. Hughes, S. O., Power, T. G., Liu, Y., Sharp, C. & Nicklas, T. A. Parent emotional distress
and feeding styles in low-income families. The role of parent depression and parenting
stress. Appetite 92, 337–342 (2015).
62. Brown-Riggs, C. Nutrition and Health Disparities: The Role of Dairy in Improving Minority
Health Outcomes. Int. J. Environ. Res. Public. Health 13, 28 (2015).
63. Bandy, T. & Moore, K., A. What Works for Latino/Hispanic Children and Adolescents:
Lessons from Experimental Evaluations of Programs and Interventions - Child_Trends-
2011_02_01_RB_WW4LatinoChildren.pdf. childtrends.org (2011). Available at:
https://www.childtrends.org/wp-content/uploads/2011/02/Child_Trends-
2011_02_01_RB_WW4LatinoChildren.pdf. (Accessed: 31st July 2017)
64. National Center for Education Statistics. Early Childhood Program Participation Survey of
the National Household Education Surveys Program (ECPP-NHES:2005). (2005).
Available at: https://nces.ed.gov/programs/digest/d09/tables/dt09_044.asp. (Accessed: 1st
August 2017)
65. Foltz, J. L. et al. Population-Level Intervention Strategies and Examples for Obesity
Prevention in Children. Annu. Rev. Nutr. 32, 391–415 (2012).
66. Davis, J. N., Ventura, E. E., Cook, L. T., Gyllenhammer, L. E. & Gatto, N. M. LA Sprouts: A
Gardening, Nutrition, and Cooking Intervention for Latino Youth Improves Diet and
Reduces Obesity. J. Am. Diet. Assoc. 111, 1224–1230 (2011).
67. National Council of La Raza. An Essential Investment in the Health of Latino Children.
(2016). Available at: http://www.afabc.org/wp-
content/uploads/2016/09/childhoodnutrition_reauthorization_12016.pdf. (Accessed: 25th
January 2017)
68. Food Assistance Programs | Nutrition.gov. Nutrition.gov (2017). Available at:
https://www.nutrition.gov/subject/food-assistance-programs. (Accessed: 9th August 2017)
69. Martinez-Schiferl, M. & Zedlewski, S. R. Emergency food assistance helps many low-
income hispanic children. (Urban Institute, 2010).
70. Babey, S. H., Hastert, T. A. & Brown, E. R. Teens living in disadvantaged neighborhoods
lack access to parks and get less physical activity. UCLA Cent. Health Policy Res. (2007).
71. Gomez-Feliciano, L. et al. Active Living Logan Square: joining together to create
opportunities for physical activity. Am. J. Prev. Med. 37, S361–S367 (2009).
72. Gordon-Larsen, P., Nelson, M. C., Page, P. & Popkin, B. M. Inequality in the Built
Environment Underlies Key Health Disparities in Physical Activity and Obesity. Pediatrics
117, 417–424 (2006).
73. Kamel, A. A., Ford, P. B. & Kaczynski, A. T. Disparities in park availability, features, and
characteristics by social determinants of health within a U.S.–Mexico border urban area.
Prev. Med. 69, S111–S113 (2014).
74. Powell, L. M., Slater, S., Chaloupka, F. J. & Harper, D. Availability of Physical Activity–
Related Facilities and Neighborhood Demographic and Socioeconomic Characteristics: A
National Study. Am. J. Public Health 96, 1676–1680 (2006).

25 Salud America! https://salud-america.org/
75. Wilson, D. K., Kirtland, K. A., Ainsworth, B. E. & Addy, C. L. Socioeconomic status and
perceptions of access and safety for physical activity. Ann. Behav. Med. 28, 20–28 (2004).
76. Moore, L. V., Diez Roux, A. V., Evenson, K. R., McGinn, A. P. & Brines, S. J. Availability of
Recreational Resources in Minority and Low Socioeconomic Status Areas. Am. J. Prev.
Med. 34, 16–22 (2008).
77. Garcia, R. & Strongin, S. Healthy parks, schools and communities: mapping green access
and equity for Southern California. The City Project Web Site (2011). Available at:
http://www.mapjustice.org/images/Southern_California_Report_FInal_Medium_Res.2.pdf.
(Accessed: 12th June 2017)
78. Wen, M., Zhang, X., Harris, C. D., Holt, J. B. & Croft, J. B. Spatial Disparities in the
Distribution of Parks and Green Spaces in the USA. Ann. Behav. Med. 45, 18–27 (2013).
79. Galvez, M. P. et al. Associations Between Neighborhood Resources and Physical Activity
in Inner-City Minority Children. Acad. Pediatr. 13, 20–26 (2013).
80. Spengler, J. Promoting physical activity through the shared use of school and community
recreational resources. (Active Living Research, 2012).
81. Cohen, D. A. et al. Use of neighbourhood parks: does socio-economic status matter? A
four-city study. Public Health 127, 325–332 (2013).
82. Rundle, A. et al. Associations between Body Mass Index and Park Proximity, Size,
Cleanliness, and Recreational Facilities. Am. J. Health Promot. 27, 262–269 (2013).
83. Office of Disease Prevention and Health Promotion. Healthy People 2020. (2017).
Available at: https://www.healthypeople.gov/. (Accessed: 12th June 2017)
84. Shahum, L. Safe Streets: Insights on Vision Zero Policies From European Cities. (The
German Marshall Fund of the United States, 2017).
85. Logan Square Neighborhood Association. Designing the Bloomingdale Trail Event
(10/4/11). (2012). Available at: http://www.lsna.net/Issues-and-programs/Health/Youth-
Create-Visions-of-New-Bloomingdale-Trail/Designing-the-Bloomingdale-Trail-Event-10-4-
11-.html. (Accessed: 12th June 2017)
86. Miami Dade County. Parks and Open Space Master Plan. Available at:
http://www.miamidade.gov/parksmasterplan/. (Accessed: 1st August 2017)
87. National Recreation and Park Association. Parks & Recreation in Underserved Areas: A
Public Health Perspective. Available at:
http://www.nrpa.org/uploadedFiles/nrpa.org/Publications_and_Research/Research/Papers/
Parks-Rec-Underserved-Areas.pdf. (Accessed: 12th June 2017)
88. Open Streets MPLS. Open Streets MPLS. Open Streets Available at:
http://www.openstreetsmpls.org/. (Accessed: 12th June 2017)
89. Swanson, J., Ramirez, A. G. & Gallion, K. J. Making Physical Activity a Daily Experience
for Latino Youth. (2016).
90. The Trust for Public Land. The 606. The 606 (2015). Available at: http://www.the606.org/.
(Accessed: 12th June 2017)
91. National Physical Activity Plan Alliance. National Physical Activity Plan. (2016). Available
at: http://physicalactivityplan.org/docs/2016NPAP_Finalforwebsite.pdf. (Accessed: 25th
October 2017)
92. Grant, R. W., Schmittdiel, J. A., Neugebauer, R. S., Uratsu, C. S. & Sternfeld, B. Exercise
as a Vital Sign: A Quasi-Experimental Analysis of a Health System Intervention to Collect
Patient-Reported Exercise Levels. J. Gen. Intern. Med. 29, 341–348 (2014).
93. Lobelo, F. & de Quevedo, I. G. The Evidence in Support of Physicians and Health Care
Providers as Physical Activity Role Models. Am. J. Lifestyle Med. 10, 36–52 (2016).
94. Tarasenko, Y. N., Miller, E. A., Chen, C. & Schoenberg, N. E. Physical activity levels and
counseling by health care providers in cancer survivors. Prev. Med. 99, 211–217 (2017).
95. Booth, F. W., Roberts, C. K. & Laye, M. J. Lack of exercise is a major cause of chronic
diseases. Compr. Physiol. 2, 1143–1211 (2012).

26 Salud America! https://salud-america.org/
96. Fuller, B. et al. Maternal Practices That Influence Hispanic Infants’ Health and Cognitive
Growth. Pediatrics peds.2009-0496 (2010). doi:10.1542/peds.2009-0496
97. Ansari, A. & López, M. Preparing low-income Latino children for kindergarten and beyond:
How children in Miami’s publicly-funded preschool programs fare. children 7, 9 (2015).
98. Ramirez, A. Building Support for Latino Families: A Research Review. Salud America
(2017). Available at: https://salud-america.org/building-support-for-latino-families-
research/. (Accessed: 25th October 2017)
99. Kenney, M. K. Child, Family, and Neighborhood Associations with Parent and Peer
Interactive Play During Early Childhood. Matern. Child Health J. 16, 88–101 (2012).
100. Whaley, S. E., Jiang, L., Gomez, J. & Jenks, E. Literacy Promotion for Families
Participating in the Women, Infants and Children Program. Pediatrics 127, 454–461
(2011).
101. Ryan, C. Language use in the United States: 2011. Am. Community Surv. Rep. 22, 1–16
(2013).
102. Bierman, K. L., Heinrichs, B. S., Welsh, J. A., Nix, R. L. & Gest, S. D. Enriching preschool
classrooms and home visits with evidence-based programming: sustained benefits for low-
income children. J. Child Psychol. Psychiatry 58, 129–137 (2017).
103. Malik, R., Hamm, K., Adamu, M. & Morrissey, T. Child Care Deserts – Center for American
Progress.
104. Ramirez, A. Family Support Research: Policy Implications. Salud America (2017).
Available at: https://salud-america.org/family-support-research-policy-implications/.
(Accessed: 25th October 2017)
105. Tirabassi Sofield, B. M. It’s not child’s play: the impact of SES and urbanicity on access to
recess. (Rutgers University-Graduate School of Education, 2013).
106. Council on School Health. The Crucial Role of Recess in School. PEDIATRICS 131, 183–
188 (2013).
107. Karoly, L. A. The Economic Returns from Investing in Early Childhood Programs in the
Granite State. (2017).
108. Heckman, J. J. Invest in early childhood development: Reduce deficits, strengthen the
economy. Heckman Equ. 7, (2012).
109. Nix, R. L., Bierman, K. L., Domitrovich, C. E. & Gill, S. Promoting Children’s Social-
Emotional Skills in Preschool Can Enhance Academic and Behavioral Functioning in
Kindergarten: Findings from Head Start REDI. Early Educ. Dev. 24, (2013).
110. Bierman, K. L. et al. Effects of Head Start REDI on Children’s Outcomes 1 Year Later in
Different Kindergarten Contexts. Child Dev. 85, 140–159 (2014).
111. Bierman, K. L., Welsh, J. A., Heinrichs, B. S., Nix, R. L. & Mathis, E. T. Helping head start
parents promote their children’s kindergarten adjustment: The research‐based
developmentally informed parent program. Child Dev. 86, 1877–1891 (2015).
112. Mathis, E. T. B. & Bierman, K. L. Effects of parent and child pre-intervention characteristics
on child skill acquisition during a school readiness intervention. Early Child. Res. Q. 33,
87–97 (2015).
113. Ansari, A. & Winsler, A. Montessori public school pre-K programs and the school readiness
of low-income Black and Latino children. J. Educ. Psychol. 106, 1066–1079 (2014).
114. Brotman, L. M. et al. Effects of ParentCorps in Prekindergarten on Child Mental Health and
Academic Performance: Follow-up of a Randomized Clinical Trial Through 8 Years of Age.
JAMA Pediatr. 170, 1149–1155 (2016).
115. City of San Antonio. Pre-K 4 San Antonio. (2017). Available at:
http://www.sanantonio.gov/Pre-K-4-San-Antonio. (Accessed: 12th June 2017)
116. First 5 LA. First 5 LA. First 5 LA (2017). Available at: http://www.first5la.org/. (Accessed:
12th June 2017)

27 Salud America! https://salud-america.org/
117. NBC News. Chicago Program Uses Home Visits To Boost Latino Early Education. (2015).
Available at: http://www.nbcnews.com/news/latino/chicago-program-uses-home-visits-
boost-latino-early-education-n311711. (Accessed: 12th June 2017)
118. Zero to Three. Advancing the proven power of early connections. ZERO TO THREE
(2017). Available at: https://www.zerotothree.org/. (Accessed: 12th June 2017)
119. Chacko, A., Fabiano, G. A., Doctoroff, G. L. & Fortson, B. Engaging Fathers in Effective
Parenting for Preschool Children Using Shared Book Reading: A Randomized Controlled
Trial. J. Clin. Child Adolesc. Psychol. Off. J. Soc. Clin. Child Adolesc. Psychol. Am.
Psychol. Assoc. Div. 53 1–14 (2017). doi:10.1080/15374416.2016.1266648
120. Jones, D., Crowley, D. M. & Greenberg, M. T. Improving Social Emotional Skills in
Childhood Enhances Long-Term Well-Being and Economic Outcomes. (Edna Bennet
Pierce Prevention Research Center, Pennsylvania State University, 2017).
121. Bierman, K. L., Greenberg, M. T. & Abenavoli, R. Promoting Social and Emotional
Learning in Preschool: Programs and Practices that Work. (Edna Bennet Pierce
Prevention Research Center, Pennsylvania State University, 2016).
122. Center for Early Care and Education Research—Dual Language Learners (CECER-DLL),
Chapel Hill: The University of North & Carolina, FPG Child Development Institute. Social-
Emotional development in dual language learners: Annotated bibliographies from a critical
review of the research. (2011). Available at:
http://cecerdll.fpg.unc.edu/sites/cecerdll.fpg.unc.edu/files/imce/documents/AB%20-
%20Socioemotional%20Development.pdf. (Accessed: 17th August 2017)
123. Schonfeld, D. J. et al. Cluster-randomized trial demonstrating impact on academic
achievement of elementary social-emotional learning. Sch. Psychol. Q. 30, 406–420
(2015).
124. Rimm-Kaufman, S. E. et al. Efficacy of the Responsive Classroom Approach: Results
From a 3-Year, Longitudinal Randomized Controlled Trial. Am. Educ. Res. J. 51, 567–603
(2014).
125. Currie, J. & Thomas, D. Does Head Start Help Hispanic Children? Labor and Population
Program, Working Paper Series 96-17. (1996).
126. Bean, F. D. & Tienda, M. Hispanic population of the United States. (Russell Sage
Foundation, 1987).
127. Johnson, D. C., Lynch, S. & Stephens, C. Educational language policy and the new Latino
diaspora in Iowa. (2016).
128. Puente, S. & Hernandez, R. Transforming Early Learning: Educational Equity for Young
Latinos. (2009).
129. Currie, J. Economic Impact of Head Start. (2005). Available at:
https://www.princeton.edu/~jcurrie/publications/CurrieANGxp.pdf. (Accessed: 17th August
2017)
130. Deming, D. Early Childhood Intervention and Life-Cycle Skill Development: Evidence from
Head Start. Am. Econ. J. Appl. Econ. 1, 111–134 (2009).
131. Ludwig, J. & Phillips, D. A. The Benefits and Costs of Head Start. (National Bureau of
Economic Research, 2007). doi:10.3386/w12973
132. Ludwig, J. & Phillips, D. A. Long-Term Effects of Head Start on Low-Income Children. Ann.
N. Y. Acad. Sci. 1136, 257–268 (2008).
133. Garces, E., Duncan, T. & Currie, J. Longer Term Effects of Head Start. (2000). Available
at: http://www.nber.org/papers/w8054.pdf. (Accessed: 17th August 2017)
134. Temple, J. A. & Reynolds, A. J. Benefits and costs of investments in preschool education:
Evidence from the Child–Parent Centers and related programs. Econ. Educ. Rev. 26, 126–
144 (2007).
135. Schweinhart, L. J. Long-term follow-up of a preschool experiment. J. Exp. Criminol. 9,
389–409 (2013).

28 Salud America! https://salud-america.org/
136. Chetty, R., Friedman, J. N. & Rockoff, J. E. The Long-Term Impacts of Teachers: Teacher
Value-Added and Student Outcomes in Adulthood. (National Bureau of Economic
Research, 2011). doi:10.3386/w17699
137. Campbell, F. A. et al. Adult outcomes as a function of an early childhood educational
program: An Abecedarian Project follow-up. Dev. Psychol. 48, 1033–1043 (2012).
138. Smith-Morris, C., Morales-Campos, D., Alvarez, E. A. C. & Turner, M. An anthropology of
familismo: On narratives and description of Mexican/immigrants. Hisp. J. Behav. Sci. 35,
35–60 (2013).
139. Prelow, H. M., Loukas, A. & Jordan-Green, L. Socioenvironmental Risk and Adjustment in
Latino Youth: The Mediating Effects of Family Processes and Social Competence. J. Youth
Adolesc. 36, 465–476 (2007).
140. Villegas, J., Lemanski, J. & Valdéz, C. Marianismo and Machismo: The Portrayal of
Females in Mexican TV Commercials. J. Int. Consum. Mark. 22, 327–346 (2010).
141. Paludi, M. A. Praeger Guide to the Psychology of Gender. (Greenwood Publishing Group,
2004).
142. Gallo, L. C., Penedo, F. J., Espinosa de los Monteros, K. & Arguelles, W. Resiliency in the
Face of Disadvantage: Do Hispanic Cultural Characteristics Protect Health Outcomes? J.
Pers. 77, 1707–1746 (2009).
143. Espinosa, G., Elizondo, V. & Miranda, J. Hispanic Churches in American Public Life:
Summary of Findings. (University of Notre Dame Institute for Latino Studies, 2003).
144. Skogrand, L., Hatch, D. & Singh, A. Understanding Latino families, implications for family
education. (Utah State University, Extension, 2005).
145. Turner, K., Wildsmith, E. & Alvira-Hammond, M. Households of Low-Income Hispanic
Children: Composition and Economic Circumstances. in (Appam, 2016).
146. Jung, S., Fuller, B. & Galindo, C. Family Functioning and Early Learning Practices in
Immigrant Homes. Child Dev. 83, 1510–1526 (2012).
147. Smith, E. N., Grau, J. M., Duran, P. A. & Castellanos, P. Maternal Depressive Symptoms
and Child Behavior Problems among Latina Adolescent Mothers: The Buffering Effect of
Mother-reported Partner Child Care Involvement. Merrill-Palmer Q. Wayne State Univ.
Press 59, (2013).
148. Weddle, L. ., Ramirez, A. G. & Gallion, K. G. Helping Latino Children Reach a Healthy
Weight by Kindergarten. (Salud America!, 2015).
149. Ramirez, A. Latina Mom and Baby Health: A Research Review. Salud America (2016).
Available at: https://salud-america.org/latina-mom-and-baby-health-research/. (Accessed:
25th October 2017)
150. Beeber, L. S., Perreira, K. M. & Schwartz, T. Supporting the Mental Health of Mothers
Raising Children in Poverty. Ann. N. Y. Acad. Sci. 1136, 86–100 (2008).
151. Garcia, C., McNaughton, D., Radosevich, D. M., Brandt, J. & Monsen, K. Family Home
Visiting Outcomes for Latina Mothers With and Without Mental Health Problems. Public
Health Nurs. 30, 429–438 (2013).
152. Holtrop, K., McNeil Smith, S. & Scott, J. C. Associations between Positive Parenting
Practices and Child Externalizing Behavior in Underserved Latino Immigrant Families.
Fam. Process 54, 359–375 (2015).
