

ii
Acknowledgements
On behalf of the residents of Broome County, we are pleased to present the
Broome County Community Health Assessment 2019-2024
We hope that it serves to improve the health and well-being of all residents of Broome County.
With gratitude to the following individuals for their service on and contributions to the Broome County
Community Health Assessment 2019-2024 Steering Committee:
Binghamton Housing Authority – Elaine Miller
Binghamton University – Leon Cosler, Diane Crews, Yvonne Johnston, Titilayo Okoror, Christine
Podolak
Broome County Council of Churches – Michael Leahey
Broome County Health Department – Amy Chaluisant, Rebecca Kaufman, Mary McFadden,
Chelsea Reome-Nedlik, Dr. Christopher Ryan
Broome County Legislature – Kim Myers, Kelly Wildoner
Broome County Mental Health Department – Lynne Esquivel, Emily Hotchkiss-Plowe, Megan
Wise
Broome County Office for Aging – Lucia Esposito, Maria Fabrizi, Rita Fluharty, Lisa Schuhle
Broome County Planning Department – Stephanie Brewer
Broome Tioga BOCES – Alan Buyck
Broome County Urban League – Jennifer Lesko
Broome County YMCA – Gareth Sansom
Care Compass Network – Lisa Bobby, Shelbi DuBord
Cayuga Medical Associates – Jeffrey Penoyer
Cornerstone Family Healthcare – Marianne Buck, Kelly Wildey
Excellus Blue Cross Blue Shield – Melissa Klinko
Family and Children’s Society – Lisa Hoeschele
Guthrie Medical Group, PC – Shawn Karney, Hillary Saxton, Sherry Salisbury
HealtheConnections (formerly HealthlinkNY) – Adam Hughes, Rachel Kramer
Mental Health Association of the Southern Tier – Kathy Eckert
Mothers and Babies Perinatal Network – Christy Finch
Our Lady of Lourdes Hospital – Deborah Blakeney, Susan Bretscher, Bernard Bush, Wayne
Mitteer, Robin Kinslow-Evans
Rural Health Network of SCNY – Pam Guth, Mary Maruscak, Jack Salo
Southern Tier Independence Center – Chad Eldred, Susan Ruff
SUNY Upstate Medical University Clinical Campus at Binghamton – Lenore Boris
Tioga County Health Department – Amy Fancher, Lisa McCafferty, Susan Medina, Heather
Vroman
United Health Services Hospitals – Karen Bayer, Scott Hall
WEBB Consulting – Lea Webb

iii
With grateful acknowledgement
to the Broome County Health Department:
Mary McFadden, Deputy Director
Chelsea Reome, MPA, Public Health Representative
and to the Binghamton University graduate students:
Amelia Martin, Luis Midence, and Emma Ospelt
Master of Public Health (MPH) Program
Margaret Reynolds
Biomedical Anthropology Program
For their substantive contributions to the preparation of this report
and without whom this submission would not have been possible.
This report was submitted by the Broome County Community Health Assessment Coordinator, Yvonne
Johnston, DrPH, MPH, MS, RN, FNP.
Questions or comments should be directed to:
Dr. Yvonne Johnston, Associate Professor & Founding Director, MPH Program
Decker College of Nursing and Health Sciences, Binghamton University
PO Box 6000, Binghamton, NY 13902-6000
E-mail: johnston@binghamton.edu

iv
The Broome County Health Department works with the community to preserve, promote
and protect the public health and quality of life of all Broome County residents.
Our Vision:
“By 2017, Broome County will be distinguished as a community that
maximizes the opportunity for all people to take responsibility for
their own well-being and achieve their optimal quality of life. The
health of the community will also be enhanced by a community wide
partnership of organizations that will assess, prioritize and take
action on initiatives to improve specific public health indicators and
measures of community health status.”
Steering Committee for the Broome County Community Health Assessment 2019-2024
v
Cover Page
Broome County
Community Health Assessment (CHA)
Community Health Improvement Plan (CHIP)
and Community Service Plan (CSP)
2019 - 2024
County covered:
Broome County
Participating Local Health
Department:
Broome County Health Department
225 Front Street, Binghamton, NY 13905
Phone: 607-778-3930 FAX: 607-778-2838
Web: www.gobroomecounty.com/hd
Participating Hospitals:
Our Lady of Lourdes Memorial Hospital, Inc.
169 Riverside Drive, Binghamton, NY 13905
Phone: 607-798-5111
Web: www.lourdes.com
United Health Services Hospitals, Inc.
UHS Wilson Medical Center
33-57 Harrison Street, Johnson City, NY 13790
Phone: 607-763-6000
UHS Binghamton General Hospital
10-42 Mitchell Avenue , Binghamton, NY 13903
Phone: 607-762-2200
UHS Medical Group
40 Arch Street, Johnson City, NY 13790
Phone: 607-763-6293
Web: http://www.uhs.net/
Coalition/entity completing
assessment and plan:
Broome County Health Department

vi
vii
Executive Summary
The Community Health Assessment is a process for examining the health of a community. Importantly,
this assessment serves as a baseline for evaluating progress toward the New York State’s Prevention
Agenda 2024 goals. These goals are designed to improve the health of all New Yorkers. This assessment
also marks our progress toward Healthy People 2020 objectives. While completion of a community
health assessment is required of local health departments and hospitals, there are many benefits to
doing so.
The Broome County 2019-2024 Community Health Assessment is unprecedented in the fact that it has
incorporated an unparalleled array of community voices, the institutional knowledge and experience of
dedicated long-standing community partners, population-based health and evidence-based
interventions, organic local level data, and a health in all policies approach. The recent evolution of
changes in the health system landscape allowed Broome County to incorporate contemporary initiatives
that focus more on social determinants of health and the priority populations impacted by them. These
new initiatives and resources that have shaped the 2019-2024 Broome County Health
Assessment/Improvement Plan include Broome County’s Age Friendly Initiative, the Broome County
Opioid Awareness Council, the Delivery System Reform Incentive Program - Care Compass Network, the
Population Health Improvement Program, and Healtheconnections, the local regional health information
organization.
As the lead agency for this multi-tiered collaborative process, the Broome County Health Department
provided guidance, leadership, and direction working diligently with our local hospital systems,
community based organizations, education institutions, business sector, faith based communities, and
elected officials to conduct the assessment as prescribed and design a unified action plan that
incorporates our community’s most significant health priorities. This plan emphasizes the social
determinants of health, incorporates evidence-based interventions with specific actions/roles by
community partners, sustainable resources, and a focus on our community’s most disparate
populations.
Local public health priorities were identified in an iterative process by the Steering Committee beginning
in April 2019 at the CHA Symposium event and formalized at the November 2019 CHA Steering
Committee meeting. At their May 2019 meeting, the CHA Steering Committee discussed data presented
at the Symposium and considered data collected during the Symposium using the Focus Area Ranking
Tool as well as analysis of breakout session themes. The CHA Steering Committee recognized and valued
the need to align selected CHA priority areas with other initiatives (e.g., DSRIP) and with hospital
Community Service Plans (CSPs). The group spoke at length about how the social determinants of health
play into the top-ranking focus areas, and current Broome County initiatives to address those issues.
The majority of data used to determine new efforts and continuing work on some existing priorities
came from a broad set of data sources including:
State and Federal: US Census Bureau American Community Survey, NYS Prevention Agenda
Dashboard, NYS Expanded Behavioral Risk Factor Surveillance System (eBRFSS) Survey, NYS
Statewide Planning and Research Cooperative System (SPARCS), NYS Community Health
Indicators Reports (CHIRs), County Health Assessment Indicators (CHAI), NYS County Health
viii
Indicators by Race/Ethnicity (CHIRE), NYS Vital Statistics, NYS Sub-County Health Data Report for
County Health Rankings-Related Measures,
Foundations and Community Organizations: Robert Wood Johnson Foundation County Health
Rankings, Rural Broome Counts Needs Assessment, NYS Population Health Improvement Project
(PHIP) Community Dashboard (HealtheConnections), Care Compass Network (DSRIP).
Local: To garner input from the broader community at the local level, four Community Health
Surveys were issued electronically via the Broome County website and through social media of
all community partners, along with printed copies, as requested to community
partners/gatekeeper representing health disparities. The extensive data used in this process
were compiled into appended documents to this report and are intended to serve as a reference
for those seeking detailed information about our community.
The following New York State Prevention Agenda 2019-2024 priority areas, goals and focus areas have
been identified by Broome County Community Health Assessment Steering Committee:
Priority Area #1: Prevent Chronic Disease
Focus Area 1: Healthy Eating and Food Security
Goal #1: Increase access to healthy and affordable foods and beverages
Goal #2: Increase skills and knowledge to support healthy food and beverage choices
Goal #3: Increase food security
Focus Area 2: Chronic Disease Preventative Care and Management
Goal #1: Increase cancer screening rates for breast, cervical, and colorectal cancer
Goal #2: Increase early detection of cardiovascular disease, diabetes, prediabetes and obesity
Goal #3: Promote evidenced-based care to prevent and manage chronic diseases including asthma,
arthritis, cardiovascular disease, diabetes and prediabetes and obesity
Goal #4: In the community setting, improve self-management skills for individuals with chronic
diseases, including asthma, arthritis, cardiovascular disease, diabetes and prediabetes, and obesity
Priority Area #2: Promote Well-Being and Prevent Mental & Substance Use Disorders
Focus Area 1: Mental and Substance Use Disorders Prevention
Goal #1: Prevent opioid and other substance misuse and deaths
Goal #2: Prevent and address adverse childhood experiences (ACES)
Goal #4: Reduce the prevalence of major depressive disorders
Goal #5: Prevent suicides
Several activities supported development of the combined Community Health Improvement Plan (CHIP)
/Community Service Plans (CSPs). Once the Steering Committee determined the priority areas on which

ix
to focus, the NYSDOH template was populated with information solicited from members of the Steering
Committee and included identification of intervention strategies to be used, potential activities or action
items, key stakeholders, roles, resources available and possible metrics to use for measuring process and
outcomes. Steering committee members were asked to consider several elements while selecting the
interventions used for the CHIP. Some of the elements included the evidence basis, current resources
supporting potential interventions, and the ability to implement, evaluate and sustain the interventions.
The draft document was distributed prior to Steering Committee meeting and discussed. The plan was
refined over the course of several communications with members and final draft version of the CHIP was
unanimously approved by the Steering Committee in December 2019. This CHIP will serve as the basis
for ongoing Steering Committee meetings during which it will likely undergo further refinement. As the
CHIP is implemented and evaluated, specific actions/interventions may be modified and new ones
added in a continuous and dynamic plan, do, check, act (PDCA) cycle.
The Steering Committee will continue to meet on a monthly basis to assess progress to date and adapt
the CHIP as circumstances direct. quarterly basis, community partners will complete a performance
monitoring tool that tracks all CHIP related activities and process measures as well as incremental gains
made on outcome objectives. Meetings will focus on successes and setbacks encountered as
stakeholders implement the CHIP, and will serve as a forum for brainstorming and networking to ensure
success of or make modifications to the plan based on changing circumstances or emergent issues. The
Steering committee will analyze the functionality, responsiveness, and capacity of the community-health
systems-government partnership to address public health needs. New members will be welcomed at
any time to contribute to process. As part of ongoing analysis of performance, the Steering Committee
will seek additional representation from sector specific community organizations and priority population
representatives to assist with evaluating impact of CHIP.
In closing, it is important that we reflect on the magnitude of this assessment process and importance of
producing an action plan that will undoubtedly shape the health outcomes of our community over the
next several years. The undertaking of work from our community partners; including Binghamton
University’s Graduate Students, and support of our health department and hospitals’ leadership
fostered a comprehensive, in depth look into the health status of those who live here in Broome County.
It is hoped that this information will help to inform policy, systems and environmental changes that will
affect all levels of the health impact pyramid, while serving as a resource for academics and clinicians,
and assisting individuals to focus on the health of their community and finding ways to improve it.

x
TABLE OF CONTENTS
Contents
Acknowledgements ................................................................................................ ii
Our Vision: ............................................................................................................... iv
Cover Page .............................................................................................................. v
Executive Summary................................................................................................ vii
TABLE OF CONTENTS.............................................................................................. x
Section One — Populations at Risk ...................................................................... 1
A. Demographic and Health Status Information ..............................................................................1
Population .................................................................................................................................................................................... 1
Age and Gender .......................................................................................................................................................................... 5
Race and Ethnicity ................................................................................................................................................................... 7
Income and Poverty Level ..................................................................................................................................................... 9
Employment ............................................................................................................................................................................. 11
Education .................................................................................................................................................................................. 12
Housing ....................................................................................................................................................................................... 16
Marital Status .......................................................................................................................................................................... 17
Households and Families .................................................................................................................................................... 17
Grandparents ........................................................................................................................................................................... 17
Language & Nativity ............................................................................................................................................................ 17
Disability .................................................................................................................................................................................... 18
Veteran Status ......................................................................................................................................................................... 18
Commuting ............................................................................................................................................................................... 18
Natality ....................................................................................................................................................................................... 20
Morbidity ................................................................................................................................................................................... 21
Mortality .................................................................................................................................................................................... 30
Premature Death and Years of Productive Life Lost ............................................................................................. 32
Basic Service Area: Family Health ................................................................................................. 34
Dental Health Education .................................................................................................................................................... 34
Primary and Preventive Health Care Services ......................................................................................................... 35
Lead Poisoning ........................................................................................................................................................................ 36
xi
Prenatal Care and Infant Mortality .............................................................................................................................. 37
Family Planning ..................................................................................................................................................................... 39
Nutrition .................................................................................................................................................................................... 41
Injury Prevention ................................................................................................................................................................... 42
Basic Service Area: Disease Control ............................................................................................... 44
Sexually Transmitted Diseases ........................................................................................................................................ 44
Tuberculosis ............................................................................................................................................................................. 45
Communicable Diseases...................................................................................................................................................... 46
Immunizations ........................................................................................................................................................................ 49
Chronic Diseases: Cancer ................................................................................................................................................... 50
Chronic Diseases: Cardiovascular Disease ................................................................................................................. 53
Chronic Diseases: Cerebrovascular Disease (Stroke) ............................................................................................ 55
Chronic Diseases: Diabetes Mellitus .............................................................................................................................. 57
Chronic Diseases: Cirrhosis ............................................................................................................................................... 57
Chronic Diseases: Asthma .................................................................................................................................................. 58
Chronic Diseases: Chronic Obstructive Pulmonary Disease ............................................................................... 59
Human Immunodeficiency Virus (HIV) & Acquired Immunodeficiency Syndrome (AIDS) ................. 60
Optional Service Areas ................................................................................................................. 61
Dental Health Services ........................................................................................................................................................ 61
Home Health Services .......................................................................................................................................................... 63
Optional Other Service Areas / Programs ...................................................................................... 63
Medical Examiner .................................................................................................................................................................. 63
Emergency Medical Services ............................................................................................................................................ 63
Laboratories ............................................................................................................................................................................. 63
B. Behavioral Risk Factors ............................................................................................................ 64
Physical Activity ..................................................................................................................................................................... 66
Diet & Nutrition ...................................................................................................................................................................... 69
Overweight and Obesity ...................................................................................................................................................... 70
Tobacco Use .............................................................................................................................................................................. 74
Substance Abuse ..................................................................................................................................................................... 75
Mental Health .......................................................................................................................................................................... 78
Poverty, Crime, & Delinquency among Youth ........................................................................................................... 78
Depression in the Elderly ................................................................................................................................................... 79
Social Determinants of Health ......................................................................................................................................... 79
C. The Local Healthcare Environment ........................................................................................... 81
The Physical Environment - Geography & Climate ................................................................................................ 81
xii
Legal Aspects - Laws & Regulations .............................................................................................................................. 82
Social Aspects .......................................................................................................................................................................... 83
Health Care and Economics .............................................................................................................................................. 83
Institutions - Schools ............................................................................................................................................................ 83
Agriculture ................................................................................................................................................................................ 84
Media Messages ...................................................................................................................................................................... 84
Laws and Regulations .......................................................................................................................................................... 85
Environmental Management ........................................................................................................................................... 85
Section Two — Local Health Unit Capacity Profile ....................................... 86
Introduction ................................................................................................................................. 86
Organization ................................................................................................................................ 87
Staffing & Skill Level ............................................................................................................................................................. 88
Expertise & Technical Capacity ......................................................................................................................................... 88
Adequacy & Deployment of Resources .......................................................................................... 89
Administration ......................................................................................................................................................................... 89
Maternal Child Health and Development ..................................................................................................................... 94
Environmental Health ........................................................................................................................................................ 100
Clinic Services......................................................................................................................................................................... 104
Chronic Disease and Injury Prevention Program Grants ..................................................................................... 112
Child Fatality Review Team Report .............................................................................................................................. 115
Section Three — Problems and Issues in the Community .............................. 127
A. Profile of Community Resources ............................................................................................. 127
Assessment of Services ...................................................................................................................................................... 127
B. Access to Care ........................................................................................................................ 128
Hospitals ................................................................................................................................................................................. 128
Primary Care & Other Healthcare Services ............................................................................................................ 129
Healthcare Workforce ...................................................................................................................................................... 134
Primary Care & Preventive Health Services Utilization ................................................................................... 139
C. Emerging Issues in the Community .......................................................................................... 140
The Opioid Epidemic ......................................................................................................................................................... 140
The Vaping Scourge ........................................................................................................................................................... 145
The Age Friendly Initiative ............................................................................................................................................. 148
Food Insecurity .................................................................................................................................................................... 151
The Housing Crisis .............................................................................................................................................................. 153
Transportation Troubles ................................................................................................................................................. 158
Burdens of the Uninsured................................................................................................................................................ 161

xiii
D. Broome County Community Health Assessment 2019-2024 Process ......................................... 163
Collaborative Partners ..................................................................................................................................................... 163
Collaborative Efforts ......................................................................................................................................................... 163
Vision ........................................................................................................................................................................................ 164
Community Themes & Strengths Assessment ........................................................................................................ 164
Community Health Status Assessment ...................................................................................................................... 164
Local Public Health System Assessment ................................................................................................................... 165
Forces of Change Assessment ........................................................................................................................................ 165
Development of the Community Service Plans & Community Health Improvement Plan ................ 166
Community Health Assessment Symposium ........................................................................................................... 167
Community Survey ............................................................................................................................................................. 169
Section Four — Local Health Priorities ......................................................... 172
A. Prevention Agenda Priorities ................................................................................................. 172
Summary of the Process for Identification of Local Public Health Priorities ......................................... 172
HIGH PRIORITY: Promote Well-Being and Prevent Mental & Substance Use Disorders- Mental and
Substance Use Disorders Prevention ......................................................................................................................... 174
HIGH PRIORITY: Prevent Chronic Diseases – Healthy Eating and Food Security ................................ 174
Summary
..................................................................................................................................................................................................... 175
Section Five — Opportunities for Action: The Community Health
Improvement Plan .............................................................................................. 176
Priority Area #1: Prevent Chronic Disease .................................................................................... 176
Focus Area #1: Healthy Eating and Food Security ............................................................................................. 176
Focus Area #2: Preventive Care and Management ............................................................................................. 179
Priority Area #2: Promote Mental Wellbeing and Prevent Mental & Substance Use Disorders ...... 182
Focus Area #!: Prevent Mental and Substance User Disorders ..................................................................... 182

Broome County
Community Health Assessment 2019-2024 1
Section One — Populations at Risk
A. Demographic and Health Status Information
Population
Broome County is located in the Southern Tier of New York State (NYS), which encompasses nine
counties along the Pennsylvania border and is one of three counties in the central New York region.
The estimated population of Broome County in 2018 was 191,659. The county covers a land area of
705.77 square miles yielding a population density of 272 persons per square mile. The county is
comprised of 16 towns, 7 villages, and 1 city. Three towns (Chenango, Union, and Vestal) and one city
(Binghamton) have populations greater than 10,000 and 14 towns have populations less than 10,000
(Figure 3). The largest concentrations of residents are located in the southwest section of the county,
which includes the City of Binghamton and the towns of Vestal and Union (Figure 4). Broome County
ranks 19
th
out of 62 counties in population size. State population maps appear in Appendix B1-B3.
Figure 1. Broome County Population, 1810–2010
The population of Broome County grew steadily
from 1810 to 1970, peaking at 221,815 persons
in 1970 (Figure 1). This growth was attributable
to manufacturing opportunities offered by such
businesses as Endicott-Johnson Shoe Company,
International Business Machines (IBM), and Link
Flight Simulation. Since 1970, Broome County
has experienced a net out-migration due to
economic forces resulting in a reversal of this
trend (Table 1 and Figure 2).
SOURCE: US Census Bureau, Population of States and Counties of the
United States: 1790 to 1990; American Fact Finder, 2000, 2010
Population projection estimates suggest that this decline is likely to continue through 2050 with a net
population loss of approximately 5,000 persons over this period of time (Cornell University, Program on
Applied Demographics [PAD] Projections, 2019). The population changes are not evenly distributed
across municipalities. Between 2000 and 2018, the towns of Maine and Triangle experienced a net
outmigration that exceeded 10% while the towns of Barker and Lisle experienced net population
increases in excess of 15% and 5% respectively (Figure 5). Between 2010 and 2015, Conklin, City of
Binghamton and Nanticoke experienced the largest population losses (2.7%, 2.8%, and 3.4%

Broome County
2 Community Health Assessment 2019-2024
respectively).
1
Both Conklin and Nanticoke have a high percentage of their populations located within
the 1% and 0.2% flood boundaries (Conklin, 62.2% and 70.7% respectively; Nanticoke, 62.4% for both).
2
Flooding from severe storms particularly in September of 2004 and June 2006 may account for at least
some of these population losses during the previous intercensal period, and population impacts from
hurricane Irene and tropical storm Lee in 2011 and hurricane Sandy in 2012 may account for some of
these losses during the current intercensal period.
Table 1. Population Estimates, Broome County, NY, 2000–2018
Year
(as of July 1)
Population
Estimate
Population
Loss
Percent Change
(from Previous Year)
2000
200,299
—
—
2001
199,958
341
-0.170
2002
199,670
288
-0.144
2003
198,326
1,344
-0.673
2004
197,453
873
-0.440
2005
196,127
1,326
-0.672
2006
195,942
185
-0.094
2007
195,477
465
-0.237
2008
195,018
459
-0.235
2009
194,630
388
-0.199
2010
200,272
5,642
+2.899
2011
199,031
1241
-0.620
2012
198,060
971
-0.488
2013
197,911
149
-0.075
2014
197,251
660
-0.333
2015
195,794
1457
-0.739
2016
194,345
1449
-0.740
2017
192,959
1386
-0.713
2018
191,659
1300
-0.674
SOURCE: US Census Bureau, Population Estimâtes Program, 2000-2018
1
Cornell Program on Applied Demographics. (2017). Broome County Profile 2017: A collection of recent
demographic, social and economic data. Retrieved from https://pad.human.cornell.edu/profiles/Broome.pdf
2
Broome County Hazard Mitigation Plan. (2013). DMA 2000 Hazard Mitigation Plan Update – Broome County, New York.
Retrieved from
http://gobroomecounty.com/files/planning/_pdf/Hazard%20Mitigation/Final%20Draft%20For%20Approval/Section%205_4_1
%20b%20Flood%20February%202013%20low%20res.pdf

Broome County
Community Health Assessment 2019-2024 3
Figure 2. Population Trend, Broome County, NY, Actual 2000–2018, Projected 2019-2050
SOURCE: US Census Bureau, Population Estimates Program, 2000–2012; Cornell University, Program on
Applied Demographics Projections, 2013
Figure 3. Population Estimates by Municipality, Broome County, NY, 2018
Source: U.S. Census Bureau, American Community Survey 5-Year Estimates, 2018
186,000
188,000
190,000
192,000
194,000
196,000
198,000
200,000
202,000
Population Count
Year
Broome County Population Trend,
Actual 2000-2018, Projected 2019-2050
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
45,000
50,000
Population Count
Town / City
Population Estimates by Municipality,
Broome County, NY 2018

Broome County
4 Community Health Assessment 2019-2024
Figure 4. Population Map of Broome County, NY (persons per square mile), Broome County, NY, 2010
SOURCE: Cornell University, Program on Applied Demographics Projections, 2017
Figure 5. Intercensal Percent Population Change by Municipality, 2010-2018
SOURCE: US Census Bureau Intercensal Population Estimates, 2010-2018
-15.0
-10.0
-5.0
0.0
5.0
10.0
15.0
20.0
Percent Population Change
Town / City
Intercensal Percent Population Change
by Municipality, 2010-2018

Broome County
Community Health Assessment 2019-2024 5
Figure 6. Population Estimates by Age Category, Broome County, NY, 2018
SOURCE: US Census Bureau, Population Estimates Program, 2018
Age and Gender
Population estimates by gender for Broome County (2017) appear in Appendix B5. Specific age groups
by gender (2017) appear in Appendix B4. The median age in Broome County is 38.1 years for males, 42.2
for females, and 39.6 overall, ranking it in the third quartile for NYS. In comparison, the median age is
38.4 years in NYS and 37.8 years in the US. Children under 18 years of age comprise 19.5% of the
population; and adults age 65 and older, 17.9% (Figure 6), yielding a child dependency ratio
3
of 31.4, an
old age dependency ratio
4
of 28.6, and an age dependency ratio
5
of 60.1. These figures are 33.4, 23.9,
and 57.3 for NYS, and 36.9, 23.9, and 60.8 for the US respectively. Maps from the Census 2010 showing
counties by age concentrations appear in Appendix B6 and B7, and graphically depicts the lower
concentration of youth and higher concentration of elderly relative to the rest of the state. Thus,
Broome County experiences a greater burden of care for their elderly than NYS or the US.
For the estimated 2017 population, 48.8% are male and 51.2% are female. The population pyramid in
Figure 7 depicts 5-year age groups or cohorts for both males (left side) and females (right side). Up to
age 40, males outnumber females, but after age 50 women comprise the larger proportion of the total
3
The child dependency ratio = [(the number of people age <18) (the number of people age 18-64)] x 100. This ratio reflects the burden of care
for children on the working population.
4
The old age dependency ratio = [(the number of people age 65+) (the number of people age 18-64)] x 100. This ratio reflects the burden of
care for elders on the working population.
5
The dependency ratio = [(the number of people age <18 + the number of people age 65+) (the number of people age 18-64)] x 100. This
number reflects the care burden for the economically dependent members of society on the working population.
Under 5 years, 5%
5 to 9 years, 5%
10 to 14 years, 5%
15 to 19 years, 8%
20 to 24 years, 10%
25 to 29 years, 6%
30 to 34 years, 5%
35 to 39 years, 6%
40 to 44 years, 5%
45 to 49 years, 6%
50 to 54 years, 7%
55 to 59 years, 8%
60 to 64 years, 7%
65 to 69 years, 6%
70 to 74 years, 4%
75 to 79 years, 3%
80 to 84 years, 3%
85 years and over, 3%
2018 Population Estimates by Age Category

Broome County
6 Community Health Assessment 2019-2024
population. The sex ratio
6
is 107.7 in the three youngest cohorts (ages 0 to 14) as compared to 62.1 in
the three oldest cohorts (75 and older), which reflects the higher mortality rates among older men.
Because women tend to have less economic security than men, widows who live alone may require
more services or assistance to remain in their home. The “bulge” in the young adult population is likely
attributable to college attendance at Broome Community College and Binghamton University, and the
narrowing in the 30–39 age category suggests that graduates subsequently seek job opportunities
outside Broome County. The outmigration of young adults and an aging population are responsible for
the higher observed old age dependency ratio, which indicates the burden of care on working families in
order to support an aging population.
Figure 7. Population Pyramid by Age and Gender, Broome County, NY, 2017
SOURCE: US Census Bureau, Population Estimates Program, 2018
Figure 8 provides data for age distribution of populations across municipalities (see also Appendix B8).
Municipalities with the largest percentage of population 65 years of age or older are the towns of
Sanford (25.2%), Nanticoke (21.7%), and Kirkwood (20.0%). Municipalities with the largest proportion of
population under the age of 15 years are the towns of Lisle (20.2%), Conklin (20.0%), and Triangle
(19.6%). In this figure, each bar represents 100% of the population for each municipality. The different
color lengths are sectioned based on the relative percentages of the age groups within each
municipality. The age dependency ratios are graphically represented by the length of the top and
bottom sections in relation to the middle section of each bar. Towns with the highest dependency ratios
are Sanford, Nanticoke, and Kirkwood; and towns with the lowest dependency ratio are Barker,
Colesville, and Vestal.
6
The sex ratio = [(the number males) (the number of females)] x 100
4,744
4,659
5,532
6,674
9,510
5,919
5,088
4,944
4,836
5,689
6,308
7,819
5,812
5,265
4,886
3,662
3,313
3,544
Under 5 years
5 to 9 years
10 to 14 years
15 to 19 years
20 to 24 years
25 to 29 years
30 to 34 years
35 to 39 years
40 to 44 years
45 to 49 years
50 to 54 years
55 to 59 years
60 to 64 years
65 to 69 years
70 to 74 years
75 to 79 years
80 to 84 years
85 years and over
Female
Male
5,432
5,846
4,801
8,284
10,278
4,915
5,192
5,771
3,798
5,361
6,470
6,853
6,929
5,391
3,589
2,822
2,078
1,625

Broome County
Community Health Assessment 2019-2024 7
Figure 8. Age Distribution by Municipality, Broome County, NYS, Census 2017
SOURCE: US Census Bureau, Census 2017
Race and Ethnicity
The majority of Broome County’s population is white and non-Hispanic (Table 2, see also Appendices B9
& B10). Population estimates indicate that the proportions of Blacks and Asians have increased between
2000 and 2017. For Black non-Hispanics, the population has increased from 3.3% to 5.8% and for Asian
non-Hispanics from 2.8% to 4.2%. The proportion of Hispanics or Latinos, regardless of race, has also
increased from 2.0% in 2000 to an estimated 4.0% in 2017. Population trends for Black non-Hispanics,
Asians, and Hispanics indicate a continuous near linear increase. (Appendices B11-B13).
Rural areas of Broome County show less diversity than urban areas (Figure 9 and Appendix B14); and in
all areas of Broome County, the proportion of non-white population is well-below NYS and US averages
(Table 2). The municipalities with the highest percentage of Blacks include the City of Binghamton
(11.2%), the town of Union (6.3%) and the town of Dickinson (5.1%). The municipalities with the largest
concentration of Asians are Vestal (13.2%) and the City of Binghamton (4.6%). The largest
concentrations of Hispanics are in the City of Binghamton (7.1%) and the towns of Kirkwood (7.0%) and
Vestal (4.7%).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Municipality
Age Distribution by Municipality, Census 2017
65+
15-64
Age < 15

Broome County
8 Community Health Assessment 2019-2024
Table 2. Population Estimates by Race / Ethnicity Category, Broome County, NY, 2012, 2017
Race / Ethnicity Category
Broome County
NYS
US
2012
Census
Percent
2017
Estimate
Percent
2012
%
2017
%
2012
%
2017
%
One race
193,793
97.8
196,124
97.2
97.3
95.9
97.1
96.9
White
173,806
87.8
168,776
86.1
65.2
63.8
73.9
73.0
Black or African American
9,993
5.0
11,279
5.8
15.6
15.7
12.6
12.7
American Indian or Alaska
Native
451
0.2
451
0.2
0.4
0.4
0.8
0.8
Asian
7,242
3.7
8,321
4.2
7.7
8.3
5.0
5.4
Native Hawaiian or Other
Pacific Islander
182
0.1
71
.01
-
0.01
0.2
0.2
Other race
79
0.1
197
1.0
-
8.7
3.7
4.8
Two or more races
4,267
2.2
5,480
2.8
2.7
3.0
2.9
3.1
Not Hispanic or Latino
191,002
96.4
188,305
96.0
81.8
81.1
83.1
82.4
Hispanic or Latino
7,058
3.6
7,819
4.0
18.2
18.9
16.9
17.9
TOTAL
198,060
100.0
196,124
100.0
100.0
100.0
100.0
100.0
SOURCE: US Census Bureau, Census 2010, Population Estimates Program 2017
Figure 9. Minority Distribution by Municipality, Broome County, NYS, Census 2017
SOURCE: US Census Bureau, Census 2017
0
5
10
15
20
25
30
Percent of Total Population
Municipality
Minority Distribution by Municipality,
Census 2017
Two or More
Other
Asian
Black

Broome County
Community Health Assessment 2019-2024 9
Income and Poverty Level
In Broome County, the median household
income was $49,064, which is lower than both
NYS ($55,972) and the US ($51,484). These
figures are based on three-year averages and
expressed in 2017 inflation-adjusted dollars.
Median income for nonfamily households is
36.4% of that for married families. The median
earnings for an individual were $27,112. Female
earnings were 73% that of males. In addition,
there is a positive association between earnings
and educational attainment. On average, each
increase in education level yields a 30% increase
in earnings. Data tables and maps for income
appear in Appendices B15-B22.
Figure 10. Median Household Income by Municipality, Broome County, NYS, Census 2017
SOURCE: US Census Bureau, Census 2017
There were 31,795 individuals below poverty level in Broome County, which represents 17.1% of the
population for whom poverty status was determined (Table 3). For the period 2013-2017, the
proportion of individuals below poverty was higher in Broome County (17.1%) than in NYS (15.1%) or
the US (14.6%), and relates to the lower income levels observed for both individuals and households.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Municipality
Median Household Income by Municipality,
Census 2017
$100,000 or more
$50,000-$99,000
$25,000-$49,999
Less than $25,000

Broome County
10 Community Health Assessment 2019-2024
Detailed analyses of poverty level and demographic/social characteristics are provided for individuals and
for families (Appendices B23-B33). The age group with the highest percentage below poverty level is
children under 18 years of age (23.0%). The proportion of individuals below poverty level is 3.2 times
higher for Blacks/African Americans and 2.7 times higher for Asians as well as 3.0 times higher for
Hispanics (any race) than for whites (non-Hispanic). The percent below poverty level decreases with
greater educational attainment; and over 34% of individuals who have less than a high school education
are below poverty level. More than 20% of individuals who worked part-time year-round were below
poverty level and 25.0% of individuals who did not work were below poverty level.
The differences in poverty level among type of household are particularly striking (Appendix B24).
Families in which the head of household is female with no husband present have poverty rates that are
more than seven times higher than married-couple families (e.g., 32.0% vs. 4.5%). These differences are
compounded by significant racial and ethnic disparities. Over 61% percent of families receiving
Supplemental Security Income and/or cash public assistance were below poverty level, and the poverty
level was more than 64 % for families with 3 or more children in which the head of household was
female with no husband present.
Municipalities with the highest percentage of individuals or families below poverty level included the
City of Binghamton (33.3%) and the towns of Colesville (16.6%), Kirkwood (13.9%), Union (13.4%), Lisle
(13.4%), Vestal (13.4%), and Fenton (13.0%) indicating that both rural and urban areas appear to
experience higher levels of poverty than suburban areas (Appendix B32 & B33).
In relation to indicators of poverty for children and youth, rates in Broome County are higher than NYS.
In 2017, there were 8,571 children under the age of 18 who were living below poverty level (23 per 100)
and 8,272 received free or reduced-price school lunch in public schools (54.3 per 100). Between 2012
and 2017, slight decreases were observed across all poverty indicators for Broome County as well as NYS
and the US (Table 3). Poverty in childhood is associated with a wide range of social, educational, and
health-related problems, and this indicator offers an important leverage point for primary prevention.
Table 3. Poverty Indicators for Children and Youth, Broome County, New York State, US 2012 & 2017
Broome
2012
(%)
Broome
2017
(%)
NYS
2012
(%)
NYS
2017
(%)
US
2012
(%)
US
2017
(%)
Children living below poverty
(age < 18 years)
25.5
23.0
22.8
21.3
22.6
20.3
Households receiving food
stamp/SNAP benefits
(past 12 months)
17.0
16.0
15.5
15.2
13.6
12.6
Families receiving public
assistance
39.6
38.1
36.5
33.2
32.7
28.0
Households receiving
Supplemental Security Income
7.0
5.6
6.6
6.9
5.4
6.7
SOURCE: US Census Bureau, American Community Survey, 2013-2017 (5-year estimates)

Broome County
Community Health Assessment 2019-2024 11
Employment
For the period 2013-2017, the three-year unemployment rate for Broome County was 9.1%. Young
adults had the highest unemployment rates, with 15.9% of 16–19 year olds and 12.3% of 20–24 year-
olds unemployed. Unemployment rates for Blacks/African Americans, Asians, and Hispanics (any race)
were 16.7%, 8.1%, and 11.1% respectively. The rates for Blacks/African Americans and Hispanics were 2-
3 times higher than for Whites (6.3%). More than 26% of the population 16 years of age or over and who
were below the poverty level were unemployed. Of those who reported any type of disability, 15.3%
were unemployed. Trends in employment are indicators of economic vitality. The economic conditions
in NYS have resulted in similar fluctuations in unemployment for both Broome County and NYS (see
Figure 11).
Figure 11. Unemployment Rates for Broome County and New York State, 1990–2017
SOURCE: New York State Department of Labor, 1990-2017
County-specific information for employment status also appears in Appendices B34-B41. For the period
2013-2017, the three-year employment rate for Broome County was 54.1%. Employment rates were
lowest for the eldest and youngest populations and highest for the 55--64 age group (76.3.0%). Rates of
employment were higher for whites (54.8%) than for Blacks/African-Americans (49.8%), Asians (42.8%),
or Hispanics (47.4%). For those below poverty level, employment rates were 32.0% and for those with
any type of disability 31.1%. Because insurance status is generally linked to employment, lower rates of
employment are associated with lack of access to health care and health care coverage, which in turn
are related to higher morbidity and mortality rates.
Municipalities with the highest employment among the population age 16 years and over were the
towns of Kirkwood (63.9%), Barker (63.7%) and Windsor (62.6%). The highest unemployment among
municipalities included the towns of Sanford (11.8%), Nanticoke (6.1%), Lisle (7.1%), and Colesville
(6.4%), as well as the city of Binghamton (5.4%). Labor force refers to the number of people available for
work—both those who are employed and those who are unemployed, but looking for work. Individuals
who are not in the labor force include those who are going to school or are retired, those whose family
0%
2%
4%
6%
8%
10%
Percent
Year
Unemployment Rates, Broome County &
New York State, 1990–2017
Broome County
New York State

Broome County
12 Community Health Assessment 2019-2024
responsibilities keep them from working, and those who have given up trying to find a job.
Municipalities with the largest proportion of the population age 16 and over who are not in the labor
force were the towns of Dickinson (50.5%), Vestal (51.9%), and Sanford (50.3%) in addition to the city of
Binghamton (44.9 %). These data are presented in Figure 12 below.
Figure 12. Employment by Municipality, Broome County, NYS, Census 2017
SOURCE: US Census Bureau, Census 2017
Education
Comparisons of three-year estimates for educational attainment appear in Table 4 and the data are
shown in Figure 13. Among individuals 25 years of age and over, the percent population with less than a
ninth-grade education is lower for Broome County (2.9%) than for NYS (6.5%) or the US (5.4%). The
percent population who are high school graduates or who have an associate degree is higher than state
and national averages. These data indicate a somewhat more educated public. Although the percent
population enrolled in college or graduate school is higher in Broome County than in NYS or the US, a
lower percentage of the adult population who reside in the county have earned a bachelor’s degree or
higher. These data suggest that college graduates who earn their degree in Broome County may migrate
out of the local area.
Educational attainment by municipality is presented in Figure 13 and corresponding data appear in
Appendix B46. The municipalities with the highest proportion of population who have less than a high
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Municipality
Employment by Municipality, Census 2017
Armed Forces
Not in Labor Force
Civilian Unemployed
Civilian Employed

Broome County
Community Health Assessment 2019-2024 13
school education are the townships of Colesville (16.9%) and Lisle (12.6%), and the City of Binghamton
(14.9%). These municipalities represent both inner city (urban) and rural areas. The municipalities with
the highest percent population having a bachelor’s degree or better are the towns of Vestal (44.1%) and
Chenango (33.3%). These suburban areas are located near two major educational institutions: Broome
Community College and Binghamton University, which may account for the more educated population
in proximity.
School enrollment data are presented in Table 5. In Broome County, the percent of children enrolled in
preschool is lower than both state and national averages (4.9% vs. 6.0% respectively) whereas the
percent population enrolled in college or graduate school is higher for Broome County than either the
state or the nation (40.9% vs. 31.0% and 28.0% respectively). Data for school enrollment by municipality
is presented in Figure 15 and these data appear in Appendix B46. Municipalities with the highest
proportion of the student population enrolled in college located in the town of Vestal (72.3%) and the
city of Binghamton (44.8%). The annual dropout rate for Broome County for the 2016-2017 school year
was 2.9%, which was higher than the 2.1% for NYS, and the percent of high school graduates intending
to enroll in college was 88.4% compared to 84.0% for NYS. Appendices B42-B47 contain relevant
education information.
Table 4. Educational Attainment for Broome County, New York State, and United States, 2013-2017
Educational Attainment
Broome County
NYS
US
Population
Estimate
Percent
(%)
Percent
(%)
Percent
(%)
Population 25 years and over
129,802
Less than 9th grade
3,497
2.7
6.5
5.4
9th to 12th grade, no diploma
8,932
6.7
7.4
7.2
High school graduate (includes equivalency)
40,700
31.4
26.3
27.3
Some college, no degree
23,958
18.5
15.9
20.8
Associate’s degree
16,307
12.6
8.7
8.3
Bachelor’s degree
20,371
15.7
19.9
19.1
Graduate or professional degree
16,037
12.4
15.4
11.8
Percent high school graduate or higher
90.4
86.1
87.3
Percent bachelor’s degree or higher
28.0
35.3
30.9
SOURCE: US Census Bureau, American Community Survey, 2013-2017
Table 5. School Enrollment for Broome County, New York State, and United States, 2013-2017
School Enrollment
Broome County
NYS
US
Population
Estimate
Percent
(%)
Percent
(%)
Percent
(%)
Population 3 years and over enrolled in school
53,058
Nursery school, preschool
2,612
4.9
6.0
6.2
Kindergarten
2,136
4.0
5.1
4.8
Elementary school (grades 1–8)
17,093
32.2
40.2
37.9
High school (grades 9–12)
9,530
18.0
20.8
20.4
College or graduate school
21,687
40.9
28.0
31.0

Broome County
14 Community Health Assessment 2019-2024
SOURCE: US Census Bureau, American Community Survey, 2013-2017
Figure 13. Educational Attainment, 2013-2017
SOURCE: US Census Bureau, American Community Survey, 2013-2017
Figure 14. Educational Attainment by Municipality, Broome County, NYS, Census 2013-2017
SOURCE: US Census Bureau, Census 2013-2017
2.7
6.7
31.4
18.5
12.6
15.7
12.4
6.5
7.4
26.3
15.9
8.7
19.9
15.4
5.4
7.2
27.3
20.8
8.3
19.1
11.8
0
5
10
15
20
25
30
35
< 9th grade Some High
School
High school
graduate
Some college,
no degree
Associate's
degree
Bachelor's
degree
Graduate or
professional
degree
Percent of People 25 Years
and Over
Educational Attainment, 2013-2017
Broome
NYS
US
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Municipality
Educational Attainment by Municipality,
Census 2013-2017
BA/BS or Higher
Some College
High School
< High School

Broome County
Community Health Assessment 2019-2024 15

Broome County
16 Community Health Assessment 2019-2024
Figure 15. School Enrollment by Municipality, Broome County, NYS, Census 2013-2017
SOURCE: US Census Bureau, Census 2013-2017
Housing
Housing information can be found in Appendices B48. Between 2013 and 2017, Broome County had an
estimated 90,727 housing units and an 86.9% occupancy rate. The majority of housing in Broome
County (55.2%) was built before 1960 and only 10.9% of homes are newer (built since 1990). Of the total
number of housing units, most are single-unit (62.9%), 32.2% are multi-unit and 4.9% are mobile homes.
Of the occupied housing units, 65.7% are owner-occupied and 34.3% are renter-occupied. The median
value of an owner-occupied home for the 2013-2017 period was $113,100, which is 60% of the national
median value ($187,640) and only 63% of the median value of a home in NYS ($179,500). Over 62.8% of
occupied housing units use gas for heating, 11.7% use kerosene or fuel oil, 13.2% use electricity, 6.7%
use propane, and 3.6% heat their homes with wood. Monthly owner costs for housing units with a
mortgage were $1,185 for those units without a mortgage, $495, and for renters, $734. Almost 20% of
housing units with a mortgage had owner costs that were 26.0% or more of the household income, and
this figure was only 12.8% for housing units without a mortgage. In contrast, 54.1% of renters spent 30%
or more of the household income on rent. For transportation, 12.4% did not have access to a private
vehicle while 50.8% had two or more vehicles.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Municipality
School Enrollment by Municipality, Census 2013-
2017
College or Higher
Grade 9-12
Grade K-8
Preschool

Broome County
Community Health Assessment 2019-2024 17
Marital Status
Information about marital status can be found in Appendix B49. In Broome County, 45.4% of the male
population over age 15 are currently married, 40.0% were never married, 9.8% are divorced, 2.8% are
widowed, and 2.0% are separated (3-year estimates for 2013-2017). Among females over the age of 15,
41.7% are currently married, 33.6% were never married, 12.4% are divorced, 10.1% are widowed, and
2.2% are separated. In comparison to Whites, Blacks/African-Americans are more likely to be never
married or separated and less likely to be currently married. Asians are more likely to be never married
and less likely to be divorced or separated than Whites. Hispanics (any race) are more likely to be never
married and less likely to be divorced than White, Non-Hispanics. Foreign born citizens have lower rates
of divorce and separation than native citizens, which may relate to a traditional value placed on
marriage by first generation immigrants. Females are more likely to be widowed than males (10.1%
compared to 2.8%).
Households and Families
Household and family data are provided in Appendix B50. For the period 2013-2017, the total number of
households in Broome County was estimated to be 78,821 and the average household size was 2.36
persons. Most households were comprised of families, both married-couple households (42.8%) and
single head of household (16.5%, comprised of 11.5% female and 5.0% male). The remaining nonfamily
households consisted of a person living alone (34.1%) or a person living with other non-related
individuals (9%). Of those householders who live alone, 43% are over the age 65. These demographics
represent an important consideration when planning for the delivery of care, particularly in relation to
chronic disease management.
Grandparents
Information about grandparents is located in Appendix B52. An estimated 2,672 grandparents lived with
their own grandchildren under the age of 18. Of these grandparents, 68.6% had primary responsibility
for care of the children. Of those grandparents who were responsible for the care of their own
grandchildren under the age of 18, 59.3% were female, 88% were between the ages of 30 and 59 years,
66.1% were married, 36.3% had some disability, 9.8% spoke a language other than English, 5.2% did not
speak English very well, and 27.3% were below poverty level. In 20.1% of cases, no parent was present.
Language & Nativity
Although fairly homogenous in its racial make-up, Broome County has become more diverse, owing to
its use as a resettlement site for Asian/Pacific Islander, Middle Eastern, African, and Eastern European
refugees. Despite this influx, only 7.1% of people living in Broome County were foreign-born, less than
half of the national average (14.3%) and nearly one-fourth of the NYS average (24.7%). Broome County
has relatively higher rates of non-English speaking residents than many other rural upstate New York
counties. For the period 2013-2017, an estimated 9.5% of individuals five years of age or older spoke a

Broome County
18 Community Health Assessment 2019-2024
language other than English in the home including Indo-European language (4.2%), Asian/Pacific Islander
Language (2.6%), and Spanish (2.2%). Not surprisingly, individuals who speak a language other than
English in the home are more likely to be foreign-born. Notably, these individuals are more likely to be
below poverty level than those who are English-only speaking. Comparisons of educational attainment
reveal an interesting dichotomy. Compared to those who speak English only, those who speak a
language other than English in the home are more likely to have less than a high school education or to
have a bachelor’s degree or higher. Information about language and nativity can be found in Appendices
B53 and B54.
Disability
For the period 2013-2017, an estimated 15.4% of individuals age 5 or more residing in Broome County
had some type of disability; 9.3% had one disability and 8.7% had two or more disabilities. Males with
disabilities outnumbered females by 2:1 in the 5 to 17 age category, which is likely associated with high
risk behaviors and traumatic injuries that are more prevalent in this age group. In contrast, females
outnumbered males by a factor of 1.3 in the 65 and over age group, which likely relates to the longevity
of women and increased risk for disability that comes with age. Almost 35% of the total population age
65 and older reported some type of disability. Among those individuals over the age of 5 years for whom
poverty status was determined, the proportion of those with any disability was 25% for Broome County,
11.3% for NYS, and 13.6% in the US. In Broome County, 25.6% percent of individuals with a disability
have incomes below poverty level. This figure increases to almost 40% if the person has an employment
disability (determined by asking individuals if they have a physical, mental, or emotional condition
lasting 6 months or more that caused difficulty in working at a job or business). Information about
disabilities is located in Appendices B55-B58.
Veteran Status
Ten percent of the civilian population aged 18 or older in Broome County has veteran status (Appendix
B59). The majority of these individuals were veterans of the Vietnam War (34.9%), Korean War (12.7%),
or Gulf War ’90-01 (12.0%). Over 21% were from two recent Gulf War periods. Most veterans are white
(95.6%), male (94.2%), and age 55 or older (76%). Compared to non-veterans, they are less than half as
likely to be below poverty level (6.9% vs. 16.4%), but nearly twice as likely to have a disability (29.5% vs.
17.1%).
Commuting
Of the workers in Broome County age 16 or over, an estimated 88.8% used a privately-owned car, truck,
or van to get to work. Of these commuters, only 8.4% carpooled and 80.4% drove alone. Alternative
modes of transportation reported include: public transportation (excluding taxicab), 3.9%; walked to get
to work, 4.0%; bicycle, 0.1%; and taxicab, motorcycle, or other, 1.0%. Over 4% of workers age 16 or
older worked at home. 16.7% reported travel time as a half-hour or more and the mean travel time to
work was just over 18 minutes. The vast majority work in NYS (98.5%) and most worked in Broome

Broome County
Community Health Assessment 2019-2024 19
County (88.6%). Because travel occurs predominantly by privately owned vehicle, those who live in rural
areas, who are on fixed incomes, or who must travel distances may have difficulty accessing services in
urban areas. Information about commuting is located in Appendices B60.
A summary of the US Census Bureau demographic data from the American Community Survey 2013–
2017 is presented in Appendix B62.
The next section provides epidemiologic data for select areas of public health concern. In each section,
applicable Healthy People 2020 objectives are listed followed by analyses of data making comparisons
between Broome County and NYS as well as Upstate NY. Where possible, trend data are also examined
with data presented in chart format in the appendices.
To determine quartile rankings, rates among NYS counties are sorted in ascending or descending order
and subsequently divided into four equal groups so that each quartile represents one-fourth of the data.
The first quartile includes the top 25% of the data and the fourth quartile includes the bottom 25%. For
rates of disease, the data are sorted in ascending order. For screenings or health behaviors, the data are
sorted in descending order. In both cases, the first quartile or top 25% represents the best performance
on that indicator. Maps of NYS with quartile rankings are provided in the appendices.
Achievement toward relevant Healthy People 2020 objectives are explored. The Prevention Agenda
indicators for tracking NYS public health priorities are presented in Appendix B162. Data come from a
variety of sources compiled by the New York State Department of Health (NYSDOH) including the
Prevention Quality Indicators (disparities in ambulatory care sensitive conditions), the Community
Health Indicator Reports (CHIRS), and the County Health Indicators by Race/Ethnicity (CHIRE). The
county’s performance on specific indicators in relation to both state and national priorities is discussed
in relevant sections that follow.
In 2012, NYSDOH developed the CHIRS which consolidated the Community Health Assessment
Indicators (CHAI) and others within this new reporting system. The CHIRS provides data for over 300
health indicators at the county, regional, and state levels. In addition, data and maps are available that
provide quartile rankings for counties within the state. Finally, the CHIRS offers access to information
about trends over time (table and graphic form) with single- and three-year averages at the county-level
as compared to Upstate New York. Numerous data sources are used in compiling these reporting
systems including: vital statistics; hospitalization and emergency department data from the Statewide
Planning and Research Cooperative (SPARCS); specific disease registries such as for cancer, AIDS/HIV,
and sexually transmitted diseases; program-based data such as Student Weight Status Category
Reporting System (SWSCR), Behavioral Risk Factor Surveillance System (BRFSS), Women’s Infants, and
Children (WIC) program, and Childhood Lead Prevention Program among others. The CHIRE contains a
subset of these health indicators stratified by race/ethnicity in order to assist communities in addressing
disparities among minority subgroups. The CHIRE data are located in Appendix B61 and are discussed in
further detail in the Social Determinants of Health section. Citations for all data sources in this
community health assessment are noted at the bottom of each data table or chart.

Broome County
20 Community Health Assessment 2019-2024
New York State (NYS) is composed of a total of 62 counties. Upstate New York (Upstate NY) refers to the
57 counties outside of the New York City metro area and thus excludes the Bronx, Kings, New York,
Queens, and Richmond Counties.
Natality
Data related to family planning and natality can be found in Appendix B63 along with additional charts
and maps in Appendices B64-B93.
The birth rate for Broome County was 10.2 live births per 1,000 women with almost no change in this
rate for the past 5 years. This rate is somewhat lower than Upstate NY (10.6) and NYS (13.5). For the
period 2014-2016, Broome County’s fertility rate (i.e., births per 1,000 female population age 15–44)
was 53.4 per 1,000. In comparison, the fertility rate was 58.5 per 1,000 for NYS and 57.2 per 1,000 for
Upstate NY. Broome County’s fertility rate was significantly lower. For Broome County, the teen fertility
rate was: 0.6 per 1,000 for females age 10-14 years, 20.3 per 1,000 for females age 15-17 years, 26.9 for
females age 15-19 years, and 32.8 for females age 18-19 years. The fertility rate among females age 15-
17 years was significantly higher for Broome County than for Upstate NY and significantly lower among
females age 18-19 years. The fertility rates among females age 15-19 years and 18-19 years were
significantly lower for Broome County than for NYS as a whole. Broome County was in the second
quartile for the overall fertility rate, in the third quartile for fertility rate among females age 10-14 and
15-17, in the second quartile for fertility rate among females age 15-19 years, and in the first quartile for
fertility rate among females age 18-19 years. Over the last few years, teen fertility rates have trended
slightly downward across all age groups.
For the 2014-2016 period, the pregnancy rate for females age 15–44 in Broome County was 75.2
pregnancies per 1,000 females compared to 83.8 for NYS (significantly lower) and 72.8 for upstate NY.
This rate has increased slightly over the past five years. Age-specific rates were significantly lower for
Broome County than for NYS among females aged 10–14, 15–17, 18-19, and 15–19. Although Broome
County ranked in the fourth quartile for teen pregnancy among 15–17 year-olds and was significantly
higher than all other Upstate NY counties, it was below the Healthy People 2020 objective of 36.2 per
1,000. Trend data indicate that the three-year average pregnancy rate for 10–14 year-olds has declined
slightly from 1.1 to 0.6between 2006 and 2016. The three-year average for pregnancy rate among 15–19
year-old females in Broome County has similarly decreased slightly from 45.8 in 2005 to 26.9 in 2016.
There is considerable heterogeneity within the county in relation to pregnancy rates with the highest
rates in the city of Binghamton (zip codes 13901, 13903, 13904, 13905), Johnson City (zip code 13790),
Healthy People 2020 Objectives — Natality
FP-8. Reduce pregnancies among adolescent females.
FP-8.1 Reduce pregnancies among adolescent females aged 15 to 17 years
Target: 36.2 pregnancies per 1,000
FP 8.2 Reduce pregnancies among adolescent females aged 18 to 19 years
Target: 105.9 pregnancies per 1,000

Broome County
Community Health Assessment 2019-2024 21
and Deposit (zip code 13754). Though pregnancy rates are generally lower than the state, fertility rate
and trend data suggest close monitoring of and continued public health efforts in the area of teenage
pregnancy.
Morbidity
Disease morbidity relates to the prevalence or occurrence of injury or illness in a population. Prevalence
is calculated as a proportion and is defined as the number of individuals with a defined disease or
condition divided by the total population at a given point in time. Prevalence measures are useful for
assessing the public health impact of a specific disease within a community and for projecting the
medical care needs of affected individuals. Incidence refers to the number of new cases that develop in
a given period of time divided by the total population at risk. This figure provides an estimate of the
probability or risk that an individual will develop a disease and is useful for examining antecedent
exposures.
Detailed information is provided in each basic service area section that follows. A summary table of
selected morbidity indicators is provided in Table 6 below. These indicators were selected as they
represent areas in which Broome County underperformed relative to the state and provide
opportunities for improvement. Comparisons of Broome County data were made to NYS and Upstate
NY, and a check mark () appears in the column where the morbidity indicator for Broome County is
significantly higher than NYS or Upstate NY. An additional column is provided to indicate morbidity
indicators that are in the fourth quartile for the state (poorest performance), for which a check mark ()
appears in this column. The table includes both crude and age-adjusted rates. The former indicates the
actual rate of disease in the population, and the latter is useful for state-level comparisons given the age
differences between populations.
Table 6. Selected Morbidity Indicators, Broome County, 2014-2016
Morbidity Indicator
Number of
Cases
(3 years)
Rate
> NYS
> Upstate
NY
4
th
Quartile
NYS
CHILD HEALTH
Pneumonia hospitalization
(age 0–4 years, per 10,000)
23
22.4
Gastroenteritis hospitalization
(age 0–4 years, per 10,000)
S
N/A
Otitis media hospitalization
(age 0–4 years, per 10,000)
S
N/A
Incidence rate among children <72 months of
age with confirmed blood lead level ≥10 mcg/dL
(rate per 1,000 children screened)
86
11.3
ORAL HEALTH
Dental caries experience (percent of 3
rd
grade
children) [2009-2011 data]
N/A
56.7
N/A
Untreated dental caries
(percent of 3
rd
grade children) [2012]
N/A
42.3
N/A

Broome County
22 Community Health Assessment 2019-2024
Morbidity Indicator
Number of
Cases
(3 years)
Rate
> NYS
> Upstate
NY
4
th
Quartile
NYS
Caries outpatient emergency department visits
(age 3-5 years, rate per 10,000) [2016]
N/A
100.6
1
st
Morbidity Indicator
Number
of Cases
(3 years)
Rate
> NYS
> Upstate
NY
4
th
Quartile
NYS
COMMUNICABLE DISEASES
Pneumonia/flu hospitalization
(age 65+ years, rate per 10,000)
389
108.9
Chlamydia case rate – ages 15-44 years
(rate per 100,000)
700
185.9
Meningococcal incidence
(rate per 100,000)
N/A
N/A
OCCUPATIONAL
Asbestosis hospitalization
(rate per 10,000)
S
N/A
INJURY
Self-Inflicted injury hospitalization
+
(age-adjusted rate per 10,000)
143
8
Unintentional injury hospitalization
+
(age-adjusted rate per 10,000)
1,802
72.0
Age 25-64 years
576
61.8
Age 65 years and older
1,117
312.6
Fall-related hospitalization
+
(age adjusted rate per 10,000)
997
36.1
Poisoning hospitalization
+
(age-adjusted rate per 10,000)
192
12.8
ALCOHOL & OTHER DRUGS
Alcohol-related motor vehicle injuries & deaths
219
37.2
Newborn drug related discharges
(per 10,000 newborn discharges)
11.9
SOURCE: New York State Community Health Indicators Reports, 2014–2016
+
Age-adjusted hospitalization rate reported
* Rate unstable, fewer than 10 events in numerator
Broome County was lower than or similar to NYS and Upstate NY for most hospitalization rates with
several noteworthy exceptions. Pneumonia hospitalizations in children age 0–4 were significantly lower
than both statewide rates and ranked in the second quartile. Pneumonia hospitalizations among adults
age 65 and older were slightly higher in Broome County than in Upstate NY (Appendices D37 & D38).
Hospitalization rates for children age 0-4 were suppressed for both gastroenteritis and otitis media.
Child and adolescent health indicators are located in Appendix B172 with trend data and maps in
Appendices B173-B189.

Broome County
Community Health Assessment 2019-2024 23
Several categories for injury-related hospitalizations were identified as significant areas of need,
including self-inflicted injury, unintentional injury (overall, age 25-64, and 65+), falls, and poisoning. In all
categories, the rates observed in Broome County were higher than NYS and Upstate NY. In addition,
Broome County ranked in the first quartile for self-inflicted injury hospitalizations, unintentional injury
hospitalizations among adults aged 65 and older, and fall-related hospitalizations. Injury mortality and
morbidity indicators can be found in Appendix C102 with additional tables, charts, and maps in
Appendices C103-C143. An occupational hazard, asbestosis hospitalizations were higher in Broome
County than in NYS and Upstate NY. Occupational health indicators are located in Appendix C12 and in
Appendices C13-C25.
The incidence of high blood lead levels among children under the age of 6 years was significantly higher
in Broome County than in Upstate NY. Blood lead levels and lead screening appear in Appendices C24
and C25 and discussed further in the lead poisoning section that follows. Dental caries among third
grade children was significantly higher in Broome County than for NYS and the percent of third grade
children with untreated dental caries was significantly higher in Broome County than Upstate NY. The
number of emergency department visits for dental caries was higher in Broome County than in NYS but
lower than Upstate NY. Oral health indicators can be found in Appendix D273 with additional
information contained in Appendices D274-D290. Oral health is discussed further in the Dental Health
Services section. Broome County ranked in the fourth quartile for blood lead levels, dental caries
experience, and untreated dental caries, as well as in the highest quartile for emergency department
visits for dental caries.
Alcohol-related motor vehicle injuries and deaths were significantly higher in Broome County than NYS;
however, they were lower than Upstate NY (see Appendices C102 & C142-C143). Finally, the newborn
drug-related discharge rate in Broome County was significantly higher than the statewide average, and
Broome County ranked in the fourth quartile for this indicator (see Appendices C26 & C90).
The prevalence rates for asthma, diabetes, hypertension, cardiovascular disease, and
overweight/obesity are listed in Table 7. Broome County was higher than NYS and Upstate NY on most
of these measures.
Table 7. Selected Chronic Disease Indicators, Broome County, 2016
Morbidity Indicator
Prevalence
(%)
CHRONIC DISEASE
Asthma (adult)
12.2
Diabetes (adult)
8.6
High blood pressure (adult)
34.0
Cardiovascular disease (adult)
[diagnosis of heart attack, stroke, or angina]
9.4
SOURCE: New York State Community Health Indicators Reports, 2016

Broome County
24 Community Health Assessment 2019-2024
Table 7 (cont). Selected Chronic Disease Indicators, Broome County, 2014-2016
Morbidity Indicator
Prevalence
(%)
OVERWEIGHT & OBESITY
Obesity (adult)
25.7
Overweight (school-age children)
16.4
Elementary students (pre-K, K, 2
nd
& 4
th
grades)
15.5
Middle & high school students (7
th
& 10
th
grades)
18.3
Obesity (school-age children)
17.7
Elementary students (pre-K, K, 2
nd
& 4
th
grades)
15.7
Middle & high school students (7
th
& 10
th
grades)
20.7
Overweight or Obese (school-age children)
34.1
Elementary students (pre-K, K, 2
nd
& 4
th
grades)
31.3
Middle & high school students (7
th
& 10
th
grades)
39.1
Pregnant women in WIC who were pre-pregnancy …
Overweight
22.3
Obese
33.5
Children in WIC (age 2-4 years)
Obese
13.9
SOURCE: New York State Community Health Indicators Reports, 2014-2016
The incidence rate for all cancers was significantly higher in Broome County as compared to NYS.
However, incidence rates for specific cancers were not significantly higher than NYS or Upstate NY.
Although Broome County ranked in the fourth quartile for prostate cancer, the rate was significantly
higher than the upstate area or the state as a whole. Table 8 lists incidence rates cancer diagnoses. The
cancers with the greatest number of newly diagnosed individuals were female breast (184.4), prostate
(116.1), lung and bronchial (88.6), and colorectal (45.6).
Table 8. Cancer Incidence (descending order), Broome County, 2013-2015
Cancer Incidence
(rates per 100,000)
Number of Cases
(3 years)
Crude Rate
Age-Adjusted Rate
ALL CANCERS
622.1
481.4
Female breast
556
184.4
143.0
Prostate
338
116.1
88.2
Lung & bronchus
552
88.6
66.2
Colon & rectum
270
45.6
34.7
Lip, oral cavity & pharynx
99
16.7
13.0
Ovary
52
17.2
13.4
Cervix / uteri
22
7.3
6.0
Melanoma
11
3.3
2.5
LATE STAGE
Female breast
155
51.4
43.0
Prostate
60
20.6
15.2
SOURCE: New York State, Community Health Indicator Reports, 2013-2015

Broome County
Community Health Assessment 2019-2024 25
Table 9 rank orders condition-specific hospitalizations. For the period 2014-2016, the conditions with
the highest crude hospitalization rate are (descending order): diabetes (any diagnosis), cardiovascular
disease, diseases of the heart, pneumonia, unintentional injury, falls, coronary heart disease,
cerebrovascular disease, chronic lower respiratory disease, congestive heart failure, and heart attack.
Public health interventions directed toward reducing the incidence of breast, lung, and colorectal
cancers as well as hospitalizations related to diabetes, cardiovascular disease (all forms), unintentional
injuries, and falls are likely to have the greatest public health impact on overall disease morbidity for
residents of Broome County. The disproportionate ratios by race are evident in Table 10 in particular for
diabetes and asthma among Blacks as compared to Whites. Additional information related to
hospitalizations and emergency department visits can be found in Appendices B94-B133.
Table 9. Hospitalization Rates (descending order), Broome County, 2014-2016
Condition-Specific Hospitalization
(rate per 10,000)
Number of Cases
(3 years)
Crude Rate
Age-Adjusted
Rate
Hypertension (any diagnosis)
Diabetes (any diagnosis)
5,358
274.3
213.2
Cardiovascular Disease
3,239
165.8
123.1
Diseases of the Heart
2,152
110.2
81.7
Pneumonia (age 65+)
389
108.9
--
Unintentional Injury
1,802
92.3
72.0
Fall-related
997
51.0
36.1
Coronary Heart Disease
732
37.5
28.7
Cerebrovascular
598
30.6
22.3
Chronic Lower Respiratory Disease
351
29.0
23.6
Congestive Heart Failure
508
26.0
18.0
Heart Attack
491
25.1
19.3
Diabetes (primary diagnosis)
350
17.9
16.7
Hypertension (age 18+)
236
15.0
Traumatic Brain Injury
188
9.6
7.8
Asthma (age 0–17 years)
30
7.8
--
Asthma
5.0
5.4
Cirrhosis
92
4.7
4.6
SOURCE: New York State, Community Health Indicators Reports, 2014-2016
Table 10. Hospitalization Rates by Race, Broome County, NY, 2014-2016
Condition-Specific Hospitalization (rate per 10,000)
White
Black
Total
Ratio
Diabetes (any diagnosis)
182.2
358.0
189.3
2.0
Diseases of the Heart
83.5
105.9
84.2
1.3
Congestive Heart Failure
23.5
41.0
23.8
1.7
Coronary Heart Disease
28.8
31.9
29.2
1.1
Cerebrovascular
24.4
27.8
24.7
1.1
Diabetes (primary diagnosis)
12.9
35.3
14.2
2.7
Asthma (Age 0-17 years)
12.0
19.6
12.8
1.6
Asthma
9.3
20.0
9.9
2.2
Diabetes Short-term Complications
5.4
19.9
6.0
3.7
SOURCE: NYSDOH, Broome County Health Indicators by Race Ethnicity, 2014-2016

Broome County
26 Community Health Assessment 2019-2024
Prevention Quality Indicators for Adults and Children
The Prevention Quality Indicators (PQI) were developed by the Centers for Disease Control and
Prevention for use in assessing the quality of outpatient care. This set of measures includes conditions
for which appropriate outpatient care can potentially prevent the need for hospitalization or for which
early intervention can prevent complications or more severe disease. These indicators are measured as
rates of admission to the hospital for the condition in a given population and can be used to evaluate
the overall quality of primary and preventive care. Thus, the Hospital Inpatient PQIs, as a set of
population-based measures among NYS adults, identify “ambulatory care sensitive conditions” and are
available for four areas: acute admissions, circulatory admissions, diabetes admissions, and respiratory
admissions.
A similar set of population-based measures were developed for examining ambulatory sensitive
conditions among children. The NYS Hospital Inpatient Prevention Quality Indicators for Pediatric
Discharges (PDIs) include: acute discharges for gastroenteritis and urinary tract infections, short-term
complications from diabetes (diabetic ketoacidosis), and asthma. Both the Urinary Tract Infection and
Gastroenteritis PDIs include admissions for patients aged 3 months through 17 years. The Asthma PDI
includes admissions for patients aged 2 through 17 years. Eligible admissions for the Diabetes Short-
term Complications PDI includes admissions for patients aged 6 through 17 years.
Rates for the NYS PQIs and NYS PDIs are calculated using acute care, hospital discharge data from the
Statewide Planning and Research Cooperative System (SPARCS) inpatient data for counts in the
numerator and Claritas population information for the denominator. Datasets provide observed and
expected rates as well as differences in rates by resident county. The Observed Rate is the number of
discharges divided by the population then multiplied by 100,000. The Expected Rate is the number of
discharges adjusted by age group, gender and race/ethnicity divided by the population then multiplied
by 100,000. The Difference in Rates is the Observed Rate minus the Expected Rate. The PDI database
also includes risk-adjustment, calculated as the Observed PDI Rate divided by the Expected PDI Rate and
multiplied by the statewide PDI rate. Data are available for years 2009-2016 and include composite rates
as indicated in the table below:
COMPOSITE RATE
PQI Conditions
PDI Conditions
Acute
Bacterial Pneumonia
Dehydration
Urinary Tract Infection
Gastroenteritis
Urinary Tract Infection
Circulatory
Angina
Heart Failure
Hypertension
Diabetes
Diabetes Short-Term Complications
Diabetes Long-Term Complications
Lower-Extremity Amputations
Uncontrolled Diabetes
Diabetes Short-Term Complications
Respiratory
Asthma in Younger Adults
COPD or Asthma in Older Adults
Asthma
Chronic Disease
Circulatory Discharges
Diabetes Discharges
Respiratory Discharges
Diabetes Discharges
Respiratory Discharges
Overall
All PQI Discharges
All PDI Discharges

Broome County
Community Health Assessment 2019-2024 27
PQI data tables and charts are located in Appendices B100-B118 and PDI information in Appendices
B119-B133. Limitations for interpretation of estimated rates are noted as follows:
Outmigration for healthcare services: Broome County borders Pennsylvania and some
individuals who live in Broome County seek services outside the local area. Previous
examination of this concern revealed that approximately 5% of individuals seek care outside
Broome County, though no differential bias in relation to the type of care was noted. Thus, the
outmigration for healthcare services may attenuate the rates, but only to a small extent and not
for any particular type of hospital admission.
Version Changes: There may be modifications of the quality indicator logic incorporated into
version changes of the PDI software. Therefore, trends in rates must be interpreted with
caution when completing longitudinal analysis across years that utilize different versions of the
PDI software.
Transition from ICD-9-CM to ICD-10-CM Coding System: To mitigate the impact of ICD-10
compliance and PDI software version changes, as well as to facilitate trending of the PDI data, a
staggered 12-month analysis period was used to represent 2015 PDI data. Therefore, PDI rates
calculated for CY 2015 discharges should be treated with caution as they might reflect the
change in the coding system and not the trends in PDI rates.
Other Sources of Bias: Missing demographic information and zip codes as well as the stability of
rates for categories in which there are small counts can be a source of imprecision and bias in
these estimates.
Prevention Quality Indicators for Adult Discharges
Among acute care hospitalizations, the highest volume condition was bacterial pneumonia, followed by
urinary tract infection, and then dehydration (Appendix B 100). Trend analysis for bacterial pneumonia
reveals a steady decline in the observed rate between 2009 (446.3 hospitalizations per 100,000
population) and 2016 (282.1 hospitalizations per 100,000 population), which is a 36.8% reduction over
the eight year period. In 2016, the adjusted hospitalization rate for Broome County was considerably
higher than NYS (199.1 vs. 110.6 per 100,000, rate ratio 1.80). [Appendix B101]
In 2016, the adjusted rate for dehydration in Broome County was 144.7 hospitalizations per 100,000
population, which was appreciably higher than NYS (95.7 per 100,000, rate ratio 1.58). In Broome
County, trends in hospitalizations for dehydration show a U-shaped pattern with rates declining
between 2009 and 2013 and then increasing between 2013 and 2016 compared to NYS, which has had a
modest and gradual decline for most of the period. [Appendix B102]
In 2016, the adjusted rate for hospitalizations due to urinary tract infections was slightly higher in
Broome County than NYS (151.9 vs. 133.7 per 100,000, rate ratio 1.14). Both Broome County and NYS
experienced a consistent and slight decline in hospitalizations due to urinary tract infections over the 8-
year period. [Appendix B103] For all acute conditions, there was a steady decline in hospitalizations for
both Broome County and NYS, though hospitalization rates for Broome County were notably higher than
statewide. [Appendix B104]
For hospitalizations due to circulatory conditions, the highest volume condition was heart failure. In
2016, the adjusted hospitalization rate for Broome County was higher than NYS (443.4 vs. 328.9 per
100,000, rate ratio 1.35). Trend analysis for heart failure reveals an increasing trend in the observed rate
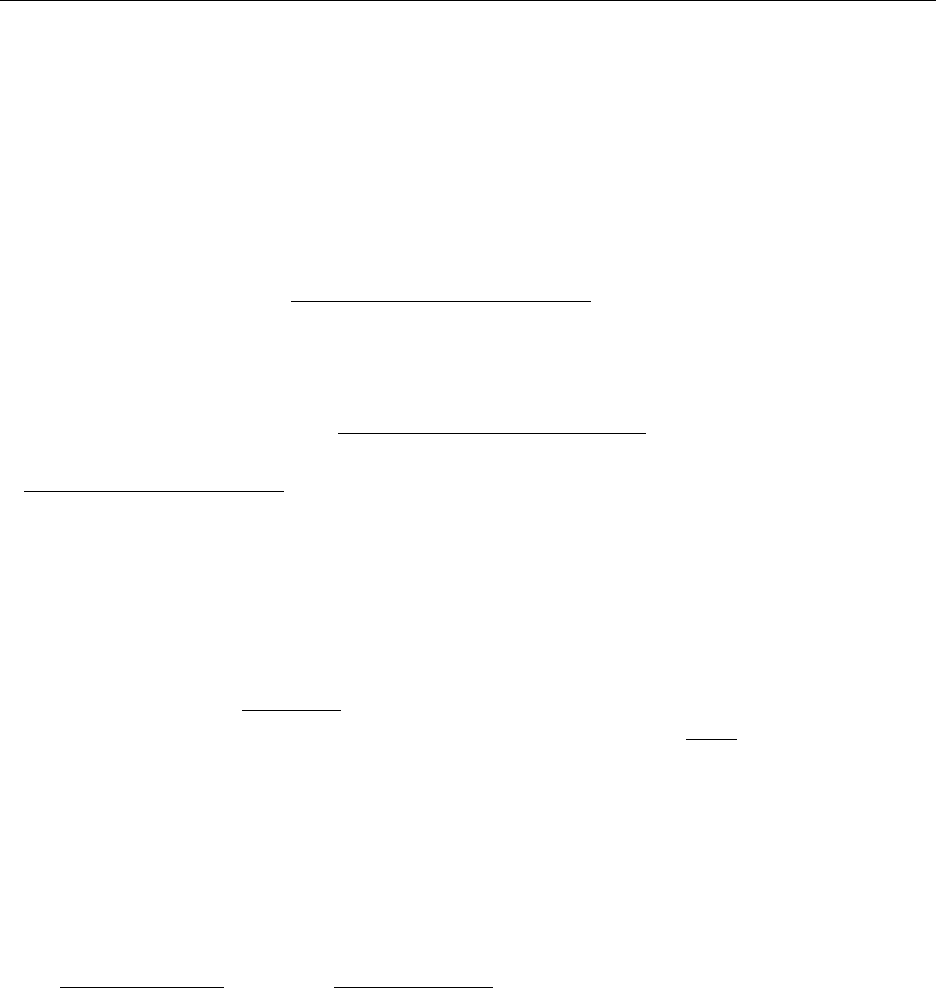
Broome County
28 Community Health Assessment 2019-2024
between 2010 (361.7 hospitalizations per 100,000 population) and 2016 (443.4 hospitalizations per
100,000 population), which is a 22.6% increase over the eight year period. [Appendix B106] Data charts
for hypertension and angina appear in Appendices B105 & B107 respectively, and the circulatory
composite in Appendix in B108. Hospitalization rates for both hypertension and angina revealed a
declining trend and these declines appear to attenuate the notable increase in heart failure
hospitalizations such that the overall circulatory composite was relatively stable over time.
For hospitalizations due to diabetic complications, the highest volume condition was for long-term
complications associated with diabetes; data for lower extremity amputation was sparse. In 2016, the
adjusted hospitalization rate for diabetes long-term complications in Broome County was lower than
NYS (66.9 vs. 79.1 per 100,000, rate ratio 0.85). [Appendix B110] Although the observed hospitalization
rates for diabetes long-term complications increased over the period, the adjusted rates showed a
modest decline.
The adjusted hospitalization rates for diabetes short-term complications in Broome County were similar
to NYS across the period and were relatively stable. [Appendix B109] Although there were fewer cases
of lower extremity amputations among patients with diabetes, the rates and trends were similar for
Broome County and NYS. [Appendix B11]. The observed hospitalization rate for uncontrolled diabetes in
Broome County declined 61.6% between 2009 and 2015 from 26.3 to 10.1 hospitalizations per 100,000
population. Rates for this indicator were similar to NYS rates as was the downward trend over time.
However, for both Broome County and NYS, there was a sudden and steep spike in uncontrolled
diabetes hospitalizations and it is not clear if this increase is an artifact of the change in ICD codes or
represents a meaningful trend. [Appendix B112]
For hospitalizations due to respiratory conditions, the highest volume condition was chronic obstructive
pulmonary disease (COPD) or asthma among older adults. Trend analysis for COPD shows a 20%
decrease in the observed rate between 2009 and 2012 (549.3 to 438.9 hospitalizations per 100,000
population), and slightly higher rates over the last three years, with an observed rate of 502.7 per
100,000 population in 2016 (Appendix B115). Adjusted rates for COPD hospitalizations were slightly
lower for Broome County than for NYS (432.8 vs. 461.5 per 100,000 population, rate ratio 0.94) in 2016,
and both Broome County and NYS showed similar decreasing trends in hospitalization rates for COPD
over the 8-year period. Hospitalization rates for asthma in young adults revealed a similar declining
trend and the overall respiratory composite rate was relatively stable with mild fluctuations over time.
For all chronic conditions and for the overall composite, there was an absolute reduction in the number
of potentially preventable hospitalizations. There were approximately 19 fewer potentially preventable
hospitalizations per 100,000 population for chronic conditions (2% decrease between 2009 and 2016),
171 per 100,000 fewer for acute conditions (21.4% decrease between 2009 and 2016), and 190 per
100,000 fewer overall (10.4% decrease between 2009 and 2016). The difference in reductions between
chronic and acute hospitalizations likely reflects the more challenging nature of preventing
exacerbations associated with chronic health conditions.

Broome County
Community Health Assessment 2019-2024 29
Prevention Quality Indicators for Pediatric Discharges (PDI)
For pediatric hospitalizations due to acute conditions in 2016, the observed rates for Broome County
were slightly higher for gastroenteritis (34 per 100,000 population) than for urinary tract infections (29
per 100,000 population). [Appendix B119] Trend analysis for gastroenteritis showed a decline in
hospitalization rates over the 8-year period. [Appendix B120] In Broome County, there was a 61%
reduction in the observed rate for gastroenteritis (the rate decreased from 87.3in 2009 to 34.1 per
100,000 in 2016). The hospitalization rates for urinary tract infection showed greater variability in the
trend line (Appendix B122). Still, there was a 34% reduction in rates between 2009 and 2016 (from 43.6
to 28.8 per 100,000 population). The adjusted rates for gastroenteritis were similar between Broome
County and NYS and they shared a similar downward trend. The adjusted rates for urinary tract
infections were similar between Broome County and NYS, though the trend was less discernable. When
adjusting for risk, however, NYS rates were flat as compared to Broome County, which showed a
pronounced decline (Appendix B123).
For pediatric hospitalizations due to diabetes short-term complications in 2016, the observed rate for
potentially preventable hospitalizations in Broome County was 22.9 per 100,000 population (Appendix
B126). The adjusted hospitalization rates for Broome County were similar to NYS and trend analysis
revealed similar stable/flat rates over the 8-year period between 2009 and 2016.
For pediatric hospitalizations due to asthma in 2016, the observed rate for potentially preventable
hospitalizations in Broome County was 60.7 per 100,000 population (Appendix B128). In 2016, the
adjusted hospitalization rates for Broome County were considerably lower for Broome County than for
NYS (141.3 vs. 208.5 per 100,000 population respectively, rate ratio 0.49). Trend analysis revealed
similar stable rates between 2009 and 2016, though Broome County rates were appreciably lower
throughout the entire 8-year period.
The acute composite for PDIs includes hospitalizations for gastroenteritis and urinary tract infections.
Although there was variability in the observed hospitalization rates, a downward trend was observable
for Broome County over the 2009-2016 period (Appendix B124). In 2016, the adjusted hospitalization
rate for the acute composite was just slightly lower in Broome County than in NYS (50.8 vs. 57.2 per
100,000 population, rate ratio 0.88). In Broome County, the observed hospitalization rate for acute
conditions was 58.8 per 100,000 population in 2009 and 34.3 per 100,000 population in 2016 (a rate
difference of 89.7 fewer hospitalizations per 100,000, rate ratio 0.58).
The chronic composite for PDIs includes hospitalizations for both diabetes short-term complications and
asthma. Similar to acute conditions, there was notable variability in the observed hospitalization rates
for the chronic composite in Broome County, though a trend was less discernable (Appendix B130). In
2016, the adjusted hospitalization rates for the chronic composite was appreciably lower in Broome
County than for NYS (117.1 vs. 164.6 per 100,000 population, rate ratio 0.71). In Broome County, the
observed hospitalization rate for chronic conditions was 154.4 per 100,000 in 2009 and 64.7 per 100,000
population in 2016 (a rate difference of 24.5 fewer hospitalizations per 100,000, rate ratio 0.42).
The risk adjusted hospitalization rate for the overall composite showed a decreasing trend for both
Broome County and NYS between 2009 and 2016. Although the trends were similar, Broome County had
consistently lower hospitalizations rates overall than NYS. A spike in hospitalization rates for the overall
composite was observable in 2015 and it is not clear if it is an artifact of the change in ICD codes.

Broome County
30 Community Health Assessment 2019-2024
Mortality
Mortality relates to the occurrence of death in a population. Mortality rates for various conditions
appear in Appendix B136. Additional information is provided in Appendices B137-B161.
The crude mortality rate for Broome County in 2016 was 1,057.8 per 100,000 population. The crude
mortality rate was 973.0 per 100,000 population for Upstate NY and 769.8 per 100,000 population for
NYS. The crude mortality rate has remained relatively stable over the past 10 years.
The top five leading causes of death in descending order are: heart disease, cancer, stroke, and chronic
lower respiratory diseases (CLRD), and unintentional injuries. For all of these conditions, Broome County
experiences a higher mortality rate than Upstate NY and the state as a whole (Table 12). Leading causes
of premature death (age 35-64 years) in descending order are: cardiovascular disease, diseases of the
heart, coronary heart disease, and cerebrovascular disease. For nearly all of these causes, Broome
County experiences a higher mortality rate than Upstate NY and the state as a whole.
Table 12. Leading Causes of Death, Broome County, Upstate New York, New York State 2014-2016
Cause of Death
(rate per 100,000 population)
Broome County
NYS
Upstate NY
Number
Rate
Rate
Rate
LEADING CAUSES OF DEATH
Heart Disease
1,552
173.3
178.1
174.4
Cancer
1,296
156.9
149.2
155.4
Stroke
243
27.5
25.6
28.3
Unintentional Injury
314
50.2
30.2
36.5
Chronic Lower Respiratory Diseases
351
40.3
28.9
34.6
Liver Disease
95
13.4
6.8
7.4
Pneumonia
20
CAUSES OF PREMATURE DEATH
Cardiovascular Disease
288
132.4
102.4
101.0
Diseases of the Heart
234
107.6
83.4
82.8
Coronary Heart Disease
150
68.9
66.4
60.5
Cerebrovascular Disease
29
13.3
10.5
10.3
Congestive Heart Failure
8
3.7*
2.5
3.3
SOURCE: New York State, Community Health Indicators Reports, 2014-2016
NOTE: * = unstable rate
Healthy People 2020 Objectives — Mortality
MICH-3 Reduce the rate of child deaths.
MICH 3.1 Reduce the rate of deaths among children aged 1-4 (26.5 deaths per 100,000 population)
MICH 3.2 Reduce the rate of deaths among children aged 5-9 (12.4 deaths per 100,000 population)
MICH- 4 Reduce the rate of adolescent and young adult deaths.
MICH 4.1 Adolescents aged 10 to 14 years (14.8 deaths per 100,000 population)
MICH 4.2 Adolescents aged 15 to 19 years (54.3 deaths per 100,000 population)
MICH 4.3 Adolescents aged 20 to 24 years (88.3 deaths per 100,000 population)

Broome County
Community Health Assessment 2019-2024 31
A summary table of selected mortality indicators is provided in Table 13, below. Comparisons of Broome
County data were made to Upstate NY and NYS, and a check mark () appears in the column where the
mortality rate for Broome County is significantly higher. An additional column is provided to indicate
mortality rates which are in the highest quartile for the state (top 25% of all counties in NYS), for which a
check mark () appears in this column. Conditions were not included in this table if the crude mortality
rate was significant but the age-adjusted rate was not. The mortality indicators in this table represent
opportunities for improvement and public health intervention.
In general, mortality rates have remained relatively stable or slightly declined over the past 16 years
(2000–2016). For many conditions, the age-adjusted rates are significantly higher for Broome County
than both NYS and Upstate NY including: diabetes and cirrhosis mortality; premature death and pre-
transport mortality due to cardiovascular disease; pre-transport mortality for diseases of the heart,
coronary heart disease, and cerebrovascular disease; and for infant and neonatal mortality. Rates for
these conditions placed Broome County in the fourth quartile relative to the rest of the state. The
absolute number of deaths (3-year total) was highest for cardiovascular disease (1,961), diseases of the
heart (1,552), all cancers (1,296), and coronary heart disease (1,299).
Thus, there are few areas in which Broome County does not experience a disproportionate share of
deaths. Although the AIDS mortality rate in Broome County was in the fourth quartile for the state, it is
nonetheless significantly lower than NYS. Mortality rates in Broome County relative to other NYS
counties were in the first quartile for: childhood mortality (age 15-19 years), suicide mortality (age 15-19
years), age-adjusted motor vehicle mortality, and alcohol-related motor vehicle injuries and deaths. In
all other areas of mortality, Broome County was not significantly different than Upstate NY or NYS.

Broome County
32 Community Health Assessment 2019-2024
Table 13. Selected Mortality Indicators, Broome County, 2014-2016
Mortality Indicator
Number of
Cases
(3 years)
Crude
Rate
Age-Adjusted
Rate
> Upstate
NY
>
NYS
4
th
Quartile
NYS
CANCER (2014-2016)
1,296
2180.7
156.9
Lung and bronchus
330
40.3
48.7
Prostate
59
16.6
23.5
Ovarian
27
5.4
10.9
DIABETES
168
28.5
20.6
CIRRHOSIS
95
16.1
13.4
CARDIOVASCULAR
1,961
332.8
218.8
Premature death (age 35-64)
288
132.4
Pretransport mortality
1,224
207.7
Diseases of the heart
1,552
263.4
173.3
Premature death (age 35-64)
234
107..6
Pretransport mortality
1,006
179.9
Coronary heart disease
977
165.8
136.2
Premature death (age 35-64)
150
68.9
Pretransport mortality
654
111.0
CEREBROVASCULAR DISEASE
243
41.2
27.5
Premature death (age 35-64)
29
13.3
Pretransport mortality
111
18.8
Homicide
13
2.2
2.8
Unintentional injury
314
53.3
50.2
Alcohol Related Motor Vehicle
Injuries and Deaths
273
37.2
INFANT MORTALITY
(per 1,000 births)
Infant (<1 year)
35
5.8
Neonatal (<28 days)
24
4.0
Post-neonatal
(1 month to 1 year)
11
1.8
Perinatal (20 weeks gestation
to 28 days of life)
56
9.2
Chronic Lower Respiratory
Diseases (COPD)
351
59.6
40.3
AIDS
10
1.7
1.4
SOURCE: New York State Community Health Indicators Reports, 2014-2016
Premature Death and Years of Productive Life Lost
For any given death, the years of productive life lost (YPPL) is the number of years prior to age 75 that
the death occurred. Deaths over age 75 neither add to nor subtract from the tally of YPLLs. Thus, the
YPLLs for a county as a whole will increase a lot with the death of one child, although those cases are
rare. A county's YPLLs will increase only a little with the death of one older adult, but the higher
frequency of that occurrence can contribute much to the total YPLLs.
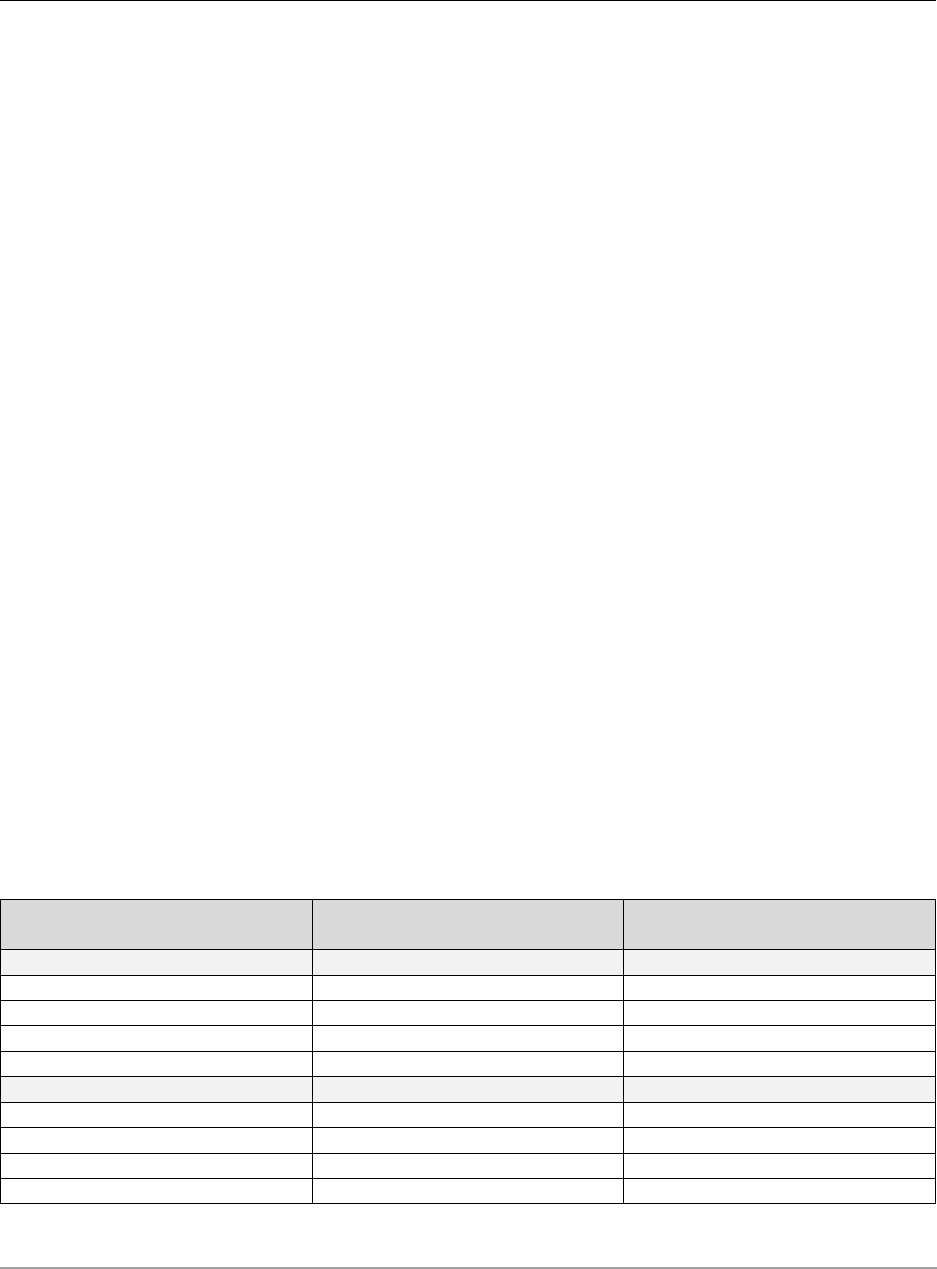
Broome County
Community Health Assessment 2019-2024 33
The single year and 3-year averages for YPLL in Broome County as compared to Upstate NY for 2001-
2016 appear in Appendix B134. In 2016, the YPPL among Broome County residents was higher than
among Upstate NY residents (7,795 vs. 6,352 per 100,000 population, rate ratio 0.81) and Broome
County ranked in the fourth quartile for this indicator among NYS counties. Between 2001 and 2016,
there was an increasing trend in the YPLL among Broome County residents as compared to Upstate NY,
whose trend was relatively stable over the same period.
A possible explanation for this increase is that chronically ill individuals (of any age) who are unable to
relocate remain in the county whereas healthy young and middle-aged adults can leave the area for jobs
or retirement. For the chronically ill who remain, each early death adds to the YPLL for the county. For
the healthy who leave, they not included in either the numerator (if they should have an untimely
death) or in the denominator (total population). Thus, high rates of outmigration among younger,
healthier residents can result in substantial increases in the YPLL. If similar patterns exist across
geographic regions, then the outmigration would likely result in non-differential bias and the relative
comparisons between regions should remain valid.
Because YPLLs place greater emphasis on deaths among youths and adolescents, these losses have a
greater impact on the metric than deaths from chronic disease among older individuals. Thus, increases
in the number of deaths due to violence, suicide, and overdose among adolescents and young adults
would contribute to a larger number of YPLLs. Individuals who do not have access to healthcare
resources are more likely to die younger, and includes those who are economically disadvantaged, those
with a disability, and/or those who reside in neighborhoods where there are higher rates of violent
crime and drug abuse. These social determinants have disproportionate impacts on the health of Black
and Hispanic residents; those who are Asian tend to experience better health outcomes. Thus, the YPPL
among these population sub-groups are higher, and such disparities were evident in YPPL for White
Non-Hispanics compared to Black Non-Hispanics and Hispanics in Broome County for the period 2009-
2013.
Age-adjusted Years of Potential Life Lost (YPLL, before age 75, rate per 100,000population), Broome
County, Southern Tier, Upstate New York, New York State, 2009-2013
COUNTY SUB-POPULATION
TOTAL PREMATURE DEATHS
YEARS OF POTENTIAL LIFE LOST
(rate per 100,000 population)
RACE / ETHNICITY
White Non-Hispanic
3,369
6,735
Black Non-Hispanic
179
10,040
Other Non-Hispanic
39
3,063
Hispanic
71
7,189
TOTAL
Broome County
3,684
6,819
Southern Tier
7,781
6,069
Upstate New York
178,012
5,528
New York State
292,218
5,352
SOURCE: New York State Department of Health, Sub-County Health Data Report for County Health Rankings-Related Measures 2016: Broome
County

Broome County
34 Community Health Assessment 2019-2024
Basic Service Area: Family Health
Dental Health Education
Information on oral health indicators can be found in appendices (D279-D296). The age-adjusted
percentage of adults who have had a dental visit within the last year in Broome County in 2016 was
67.9% compared with NYS (68.4%). Broome County ranked in the third quartile for this indicator. The
percentage of Medicaid enrollees with at least one dental visit within the last year and at least one
preventive dental visit within the last year for the three-year period 2015-2017 was (33.2%, 28.4%
respectively) and compares similarly with NYS for both indicators. Broome County ranks in the first and
second quartile for these indicators. There is still limited data available in relation to knowledge about
oral health, but from 2007-2009 the age-adjusted incidence of Lip, Oral, and Pharynx Cancer was 16.7
per 100,000 in Broome County compared with NYS (12.9 per 100,000).
The School-Based Health Center Dental Program provides education on brushing, flossing, and
nutrition at every dental visit. Oral health status indicators are presented in the Dental Health Services
section, and the data for oral health come from screenings performed on third grade children. These
data indicate a significant proportion of third grade children experience untreated dental caries, 42.3%
in Broome County from 2009-2011. Although a significant proportion of third graders experience
untreated dental caries, 80.6% have had at least one dental visit in the last year, and 88.5% have dental
insurance. The data support the ongoing and critical need for dental education in order to preserve
permanent dentition and maintain oral health. Poor dental health can lead to localized infections of the
bone and surrounding structures and has been linked to obesity and other chronic diseases including
cardiovascular disease and diabetes.

Broome County
Community Health Assessment 2019-2024 35
Primary and Preventive Health Care Services
Data for primary and preventive health care is from the Expanded Behavioral Risk Factor Surveillance
System (BRFSS) and can be found in Appendix B164-B170. In Broome County for 2016 the age-adjusted
percent of women aged 21-65 who received a Pap smear within the past three years was 82.9%, which
was similar to New York State (82.2%). Broome County was in the third and fourth quartiles respectively
for the state and well below the Healthy People 2020 objective of 93%. The percent of women in 2016
aged 50-74 who received a mammogram within the last 2 years was 58.8% in Broome County, and was
significantly lower than NYS (71.2%). The percent of women in 2016 aged 50-74 in Broome County who
received breast cancer screening was 71.3% compared with 79.7% for New York State, and is slightly
below the Healthy People 2020 objective of 81.8%. Broome County ranked in the first quartile for this
indicator. In 2016, the percentage of adults receiving a colonoscopy in the past 10 years for both age
groups 50-64, and 50-75, Broome County (68.5% and 72.9% respectively) was slightly higher than NYS
(63.1%, 68.5%).
The percentage of adults who have had their cholesterol checked in the last 5 years was 79.9% for
Broome County from 2013-2014, both males and females experienced similar percentages, and those
aged 65+ had the highest percentages. Broome County ranked in the second quartile for this indicator.
The percent of adults who were diagnosed with high blood pressure in was 34.0% for Broome County
for 2016 compared with NYS (28.9%), and Broome County ranked in the fourth quartile for this
indicator.
Healthy People 2020 Objectives — Primary & Preventive Health Care
C-15 Increase the proportion of women who receive a cervical cancer screening based on the
most recent guidelines.
Target: 93.0%
C-16 Increase the proportion of adults who receive a colorectal cancer screening based on the
most recent guidelines.
Target: 70.5%
C-17 Increase the proportion of women who receive a breast cancer screening based on the
most recent guidelines.
Target: 81.1%
HDS-4 Increase the proportion of adults who have had their blood pressure measured within the
preceding 2 years and can state whether their blood pressure was normal or high.
Target: 92.6%
HDS-5 Reduce the proportion of persons in the population with hypertension.
HDS-5.1 Reduce the proportion of adults with hypertension. (26.9%)
HDS-5.2 Reduce the proportion of children and adolescents with hypertension. (3.2%)
HDS-6 Increase the proportion of adults who have had their blood cholesterol checked within the
preceding 5 years.
Target: 82.1%

Broome County
36 Community Health Assessment 2019-2024
Lead Poisoning
Information about blood lead levels and lead screening can be found in Appendices C1-C11. The
incidence of children < 72 months of age with confirmed blood lead levels ≥ 10 mcg/dL in Broome
County was 11.3 per 1,000 children from 2014-2016, which decreased from 18.8 per 1,000 children in
2013. However, this most recent metric for Broome County (11.3) is significantly higher than NYS (4.2
per 1,000), and Broome County ranks in the third quartile for this indicator.
The percent of children born in 2013 with a lead screening by 9 months was 0.4% and was significantly
lower than NYS (1.9%) and Upstate NY (1.2%). For this same cohort of children, 58.8% in Broome County
had received a lead screening by 18 months compared to NYS (74.8%) and Upstate NY (71.7%), and
38.2% had at least two lead screenings by 36 months, compared to NYS (62.8%) and Upstate NY (55.9%).
The percentage of children receiving a lead screening by 18 months and at least two by 36 months is
significantly lower in Broome County compared with NYS for both indicators. Broome County ranks in
the first quartile in NYS for lead screenings for all age categories (lowest performance) and in the third
quartile for incidence of elevated blood lead levels among children under the age of six (higher rate).
Examination of trends shows substantial improvement of rates in lead screening among children (by age
36 months) with rates increasing from 31.7% in 2004 to 54.3% in 2013. However, there has been a
decrease in the percentage of children receiving at least one screening by 36 months in recent years,
decreasing from 67.1 in 2011 to 54.3 in 2013, and holding steady rates of about 38.0% for those
receiving at least two screenings by 36 months. Simultaneously, the incidence of elevated blood lead
levels among children under the age of 6 appears to be declining in most recent years, decreasing from
15.8 per 1,000 in 2015 to 7.9 per 1000 in 2016.
Despite these gains, additional effort in the area of lead screening is needed to prevent lead exposure
and identify children with high blood lead levels, especially when comparing Broome County to the state
of New York for the percentages of children receiving at least one or two blood lead tests by 36 months.
For employed persons age 16 and older, rates for elevated blood lead levels (≥10 mcg/dL) in Broome
County were significantly lower from 2014-2016 than both NYS and Upstate NY (5.7 per 100,000 vs. 17.3
and 19.1 respectively). Broome County ranked in the first and second quartile for this indicator and has
Healthy People 2020 Objectives — Lead Poisoning
EH-8 Reduce blood lead levels in children.
EH-8.1 Eliminate blood lead levels in children. (no applicable measure)
EH-8.2 Reduce the mean blood lead levels in children.
(1.4 g/dL average blood lead level in children age 1 to 5)
OSH-7. Reduce the proportion of persons who have elevated blood lead concentrations from work
exposures.
Target: 20.2 persons per 100,000 employed adults

Broome County
Community Health Assessment 2019-2024 37
met the Healthy People 2020 objective of less than 20.2 per 100,000 employed persons for this indicator
(Appendix C12 and C24-C25).
Prenatal Care and Infant Mortality
Maternal and infant health indicators including prenatal care and infant mortality can be found in
Appendix C26. Appendices C27-C101 contains additional charts and maps for each indicator. For the
period from 2014–2016, the percent of births with early prenatal care (those who began prenatal care in
the first trimester) was 74.0% for Broome County, compared with both NYS (75.2%) and Upstate NY
(78.4%). Broome County ranked in the third quartile on this indicator and falls below the Healthy People
2020 objective of 77.9%. The proportion of births with late (in the third trimester) or no prenatal care
from 2014 to 2016 was higher in Broome County than for Upstate NY (5.3% vs. 4.6%), but similar to NYS
(5.6%), was in the third quartile for the state. Although Broome County appears to outperform NYS,
there has been an increasing trend over the past 5 years, which is a concern.
Healthy People 2020 Objectives – Prenatal Care & Infant Mortality
MICH-1 Reduce fetal and infant deaths.
MICH-1.1 Fetal deaths at ≥ 20 weeks gestation
(5.6 fetal deaths per 1,000 live births & fetal deaths)
MICH-1.2 Fetal & infant deaths during perinatal period (28 weeks gestation to ≥ 7 days
after birth; 5.9 per 1,000 live births & fetal deaths )
MICH-1.3 Infant deaths (within 1 year)
MICH-1.4 Neonatal deaths (within the first 28 days of life)
MICH-1.5 Postneonatal deaths (between 28 days & 1 year)
MICH-3 Reduce child deaths.
MICH-3.1 Children age 1 to 4 years (25.7 deaths per 100,000 population)
MICH-3.2 Children age 5 to 9 years (12.3 deaths per 100,000 population)
MICH-4 Reduce adolescent and young adult deaths.
MICH-4.1 Children age 10 to 14 years (15.2 deaths per 100,000 population)
MICH-4.2 Children age 15 to 19 years (55.7 deaths per 100,000 population)
MICH-4.3 Children age 20 to 24 years (88.5 deaths per 100,000 population)
MICH-5 Reduce maternal deaths.
Target: 11.4 maternal deaths per 100,000 live births.
MICH-10 Increase the proportion of pregnant women who receive early and adequate prenatal care.
MICH-10.1 Care beginning in first trimester of pregnancy (77.9%)
MICH-10.1 Early and adequate prenatal care (77.6%)

Broome County
38 Community Health Assessment 2019-2024
The Kotelchuck Index is one measure used to examine the level of prenatal care and is defined as the
percentage of births to women who began care in the first trimester of pregnancy and completed at
least 80% of the expected prenatal visits. For Broome County, the percent receiving adequate prenatal
care as defined by this index was (79.9%) from 2014 to 2016, and meets the Healthy People 2020
objective of 77.6%. This percentage in Broome County was higher than both NYS (74.0%) and Upstate
NY (75.7%). Broome County ranked in the first/second quartile for this indicator and was above the
Healthy People 2020 objective of 77.6%. The percentage of women in the Special Supplemental
Nutrition Program for Women, Infants, and Children (WIC Program) with early (first trimester) prenatal
care from 2009-2011 was 83.9% for Broome County, and was lower when compared with both NYS
(86.5%) and Upstate NY (87.2%). For this low-income group, the Healthy People 2020 objective is
currently being met. Trend data indicate that early prenatal care had declined over a five-year period
between 2011 and 2016, and the percentage of births with late or no prenatal care had increased from
3.6% in 2011 to 5.6% in 2016. Thus, continued efforts in this this area will assist in reaching/maintaining
achievement of Healthy People 2020 objectives.
From 2014-2016, infant (age < 1 year) mortality for Broome County was 5.8 per 1,000 live births
compared with NYS and Upstate NY (4.5 and 5.0 respectively). From 2015-2016 the infant (age < 1 year)
mortality rate decreased from 6.6 per 1,000 to 5.0 per 1,000 in Broome County. From 2014-2016,
Neonatal (age < 28 days) mortality for Broome County was 4.0 per 1,000 live births compared with NYS
and Upstate NY (3.1 and 3.5 respectively). Broome County ranked in the third quartile for both infant
and neonatal mortality indicators.
From 2014-2016, perinatal mortality for 20 weeks gestation to 28 days of life was 9.2 per 1,000 live
births in Broome County compared with NYS (9.1) and Upstate NY (8.2). This rate decreased in Broome
County, with 11.1 per 1,000 live births in 2015 to 8.5 per 1,000 live births in 2016. From 2014-2016,
perinatal mortality for 28 weeks gestation to 7 days of life was 5.9 in Broome County, compared with
NYS (5.1) and Upstate NY (5.4). The post-neonatal (1 month to 1 year) mortality rate was 1.8 per 1,000
live births in the three-year period from 2014-2016 and was similar to statewide rates. Broome County
ranked in the third quartile for the perinatal and post-neonatal indicators.
The fetal death rate (> 20 weeks gestation) was 5.2 per 1,000 live births over the same three-year
period, compared with NYS (6.0) and Upstate NY (4.8). Again, Broome County ranked in the third
quartile. Trend data for infant deaths, neonatal deaths, post-neonatal deaths, and spontaneous fetal
deaths appear in Appendix C60-C72. On average, in Broome County fetal and infant death rates have
trended slightly downward in recent years, however some of these rates include fewer than 10 events
and are considered unstable. Notably, the infant mortality rate has trended downward from 2015-2016
in Broome County.
The maternal mortality rate for Broome County was 16.5 per 100,000 live births, for 2014-2016
(Appendices C73), compared with NYS (20.4) and Upstate NY (17.8). With this rate Broome County is
considered higher than the Healthy People 2020 objective of 11.4 per 100,000 live births, however,
there were fewer than 10 events in the numerator, so this rate is considered unstable.

Broome County
Community Health Assessment 2019-2024 39
Family Planning
For the 3-year period from 2014-2016, the percentage of births within 24 months of a woman’s previous
pregnancy was higher in Broome County (35.9%), compared with both NYS and upstate NY (31.2%, and
33.0% respectively). Broome County ranked in the fourth quartile for this indicator. Broome County
exceeded the Healthy People 2020 target of 29.8% for this metric. The percentage of births to teens
aged 15–17 was 1.6% and for teens age 15-19 was 5.4%. Although the percentage for the younger age
group was similar to NYS, the percentage for teens age 15-19 was higher than both NYS and Upstate NY
(3.8% and 4.2% respectively). Broome County ranked in the third quartile for the former and in the
second quartile for the latter. The percent of births to women 35 years of age and older was 13.7% for
Broome County, appreciably lower than the 22.1% for NYS and 20.2% for Upstate NY. The teen fertility
rate per 1,000 females in Broome County has trended downward from 2001 to 2016 for all three age
categories 15-17, 15-19, and 18-19 years, decreasing from 16.5% to 8.3%, 27.1% to 13.9%, and 37.2% to
18.8% respectively. These data are located in Appendix B under Family Planning (Appendices B63 and
B65-B89).
In Broome County, the three-year total for induced abortions was 2,128. Of these, 253 or 11.9%
occurred in the 15–19 age group. The abortion ratio (the number of induced abortions per 1000 live
births) was 350.8 for all women. For women aged 15 to 19, the abortion ratio was 778.5, which is more
than twice the overall ratio. For all ages, and in particular for the 15–19-year-old age group, the abortion
ratio was significantly lower than NYS. However, these metrics were higher than Upstate NY (231.7 and
653.3 respectively). These data are located in Appendix B under Family Planning (Appendices B90-B93).
The percentage of births to women 25 years of age or older who did not have at least a high school
education was 7.9% as compared to 12.8% for NYS and 10.1% for Upstate NY. These differences were
statistically significant, and Broome County ranked in the first/second quartile for this indicator. The
percent of births to out of wedlock mothers was 47.7% for Broome County, which was significantly
Healthy People 2020 Objectives — Family Planning
FP-5 Reduce the proportion of births occurring within 24 months of a previous birth.
Target: 29.8%
FP-8 Reduce pregnancies among adolescent females.
FP-8.1 Age 15 to 17 years (36.2 pregnancies per 1,000)
FP-8.2 Age 18 to 19 years (105.9 pregnancies per 1,000)
MICH-8 Reduce low birth weight (LBW) and very low birth weight (VLBW).
MICH-8.1 Low birth weight (LBW) (7.8%)
MICH-8.2 Very low birth weight (VLBW) (1.4%)
MICH-9 Reduce preterm births.
MICH-9.1 Total preterm births (11.4%)
MICH-9.2 Late preterm or live births at 34 to 36 weeks of gestation (8.1%)
MICH-9.3 Live births at 32 to 33 weeks of gestation (1.4%)
MICH-9.4 Very preterm or live births at less than 32 weeks of gestation (1.8%)

Broome County
40 Community Health Assessment 2019-2024
higher than the 39.3% for NYS and 38.1% for Upstate NY. Broome County ranked in the third quartile for
this indicator. The percent of first births was 37.8% for Broome County, and compared similarly to
Upstate NY (39.0%) but significantly lower than NYS (41.2%). The percent of births that were multiple
births was 3.7% for Broome County, which was similar to Upstate NY and NYS. The Caesarian section
rate for Broome County was 34.5% which was also similar to NYS and Upstate NY. Broome County
ranked in the third quartile for this indicator. Trend data indicate that the percentage of out-of-wedlock
births, the percentage of multiple births, and the percentage of births delivered by Cesarean section
have all trended slightly upward or held relatively stable between 2006 and 2016 (Appendices C26-C35,
also C58 & C59).
In relation to premature births and low birthweight from 2014-2016, Broome County figures were
similar to NYS and Upstate NY for: very low birthweight (<1.5 kg, 1.2%) and very low birthweight among
singleton births (0.7%). In Broome County the percentage of low birthweight (<2.5 kg, 7.2%) was slightly
lower when compared with NYS (7.9%) and Upstate NY (7.7%). The percentage of low birthweight
among singleton births (<2.5 kg) in Broome County (1.3%) was similar to Upstate NY and NYS. Broome
County ranked in the first and second quartiles for all categories of low birthweight. The percent of
premature (births <32 weeks in gestation) was 1.3% for Broome County, ranking in the first and second
quartiles for the state. This percentage was 7.1% for 32 to < 37 weeks gestation and 8.5% overall (<37
weeks gestation). The rates for prematurity were not significantly different than statewide rates.
Broome County was lower than both the Healthy People 2020 objectives for all gestational time points
and the Prevention Agenda 2017 target of 10.2% for preterm births. Trend data for low birthweight
reveals that from 2007 to 2016, percentages of low birthweight and very low birthweight in Broome
County have trended slightly downward or remained relatively stable over the past years. Information
about birthweight can be found in Appendices C74-C81.
The percent of births with a 5-minute APGAR score of less than 6 was 0.7% for Broome County and
performed similarly compared with statewide percentages. Broome County ranked in the first/second
quartiles for this indicator (Appendices C88 & C89).
In Broome County for 2014, newborns with withdrawal syndrome and/or affected by narcotics via
placenta or breast milk was 11.9 per 1,000 delivery hospitalizations/newborn discharges. This rate is
significantly higher than NYS (5.9 per 1,000), and Broome County ranked in the third quartile for this
indicator (Appendix C90). The number of newborns with withdrawal syndrome and/or affected by
narcotics via placenta or breast milk represents a growing concern for Broome County.

Broome County
Community Health Assessment 2019-2024 41
Nutrition
The percent of pregnant women participating in the WIC program who have anemia in the third
trimester was significantly lower for Broome County (32.9%) than for both NYS (37.3%) and Upstate NY
(36.0%) from 2009-2011. Broome County ranked in the fourth quartile for the state. The prevalence of
anemia among low income pregnant women was more than twice the Healthy People 2020 objective of
14.5%. From 2010-2012, the percentage of pregnant women in WIC that were pre-pregnancy obese
(BMI 30 or higher) was significantly higher in Broome County (33.5%) compared with NYS (24.2%) and
Upstate NY (28.6%). From 2010-2012, the percentage of pregnant women in WIC that were pre-
pregnancy overweight but not obese (BMI 25 to < 30) was significantly lower in Broome County (22.3%)
compared with NYS (26.6%) and Upstate NY (26.4%). Broome County ranked in the fourth quartile for
obesity and in the first quartile for overweight.
For Broome County, from 2014 to 2016 the percentage of infants who were fed any breast milk in the
delivery hospital was 80.5%, which was significantly lower than NYS (87.3%) and Upstate NY (83.8%).
The percentage of infants who were exclusively breastfed in the hospital was 71.0%, and this figure was
higher than both NYS (45.2%) and Upstate NY (52.4%) and the Prevention Agenda 2017 objective of
48.1%. Broome County ranked in the third quartile for any breastfeeding but in the first/second quartile
for exclusively breastfeeding in the hospital. The percentage of WIC mothers who breastfed for at least
six months over the three-year period 2014-2016 was 22.3%, and Broome County was significantly lower
than both NYS (40.3%) and Upstate NY (30.7%) for this indicator. High performance on these indicators
may reflect the baby friendly focus and policy initiatives in Broome County, though more effort is
Healthy People 2020 Objectives — Nutrition
NWS-21 Reduce iron deficiency among young children and females of childbearing age.
NWS-21.1 Children age 1 to 2 years (14.3%)
NWS-21.2 Children age 3 to 4 years (4.3%)
NWS-21.3 Females aged 12 to 49 years (9.4%)
NWS-22 Reduce iron deficiency among pregnant females.
Target: 14.5%
MICH-21 Increase the proportion of infants who are breastfed.
MICH-21.1 Infants who are ever breastfed (81.9%)
MICH-21.2 Infants who are breastfed at 6 months (60.6%)
MICH-21.3 Infants who are breastfed at 1 year (34.1%)
MICH-21.4 infants who are breastfed exclusively through 3 months (46.2%)
MICH-21.4 infants who are breastfed exclusively through 6 months (25.5%)
MICH-22 Increase the proportion of employers that have worksite lactation support programs.
Target: 38%
MICH-23 Reduce the proportion of breastfed newborns who receive formula supplementation
within the first 2 days of life.
Target: 14.2%

Broome County
42 Community Health Assessment 2019-2024
needed in relation to sustaining breast feeding through the first six months after delivery. Information
about breastfeeding is located in Appendices (C53-C57).
Injury Prevention
Due to the change in ICD codes, the comparisons between years 2014 and 2016 cannot be made. The
rate for 2015 was excluded due to SPARCS data transitioning on October 1, 2015 from ICD-9-CM to ICD-
10-CM diagnosis codes. Since ICD-9CM and ICD-10-CM are not comparable, an annual rate for 2015
cannot be calculated, and data for 2016-and-forward should not be compared with data for 2014-and-
prior. For 2016-year data, ICD-10-CM codes were used. The data table for injury indicators is located in
Appendix C102 with charts and graphs in Appendices C103-C143.
The age-adjusted suicide mortality rate per 100,000 for 2014 to 2016 was 11.8 in Broome County and
was higher than both NYS (8.0) and Upstate NY (9.9). Broome County ranked in the third quartile for this
indicator (Appendices C103-C106). The age-adjusted hospitalization rate for self-inflicted injury was
significantly higher for Broome County (8.0 per 10,000) than for NYS (3.5 per 10,000) and Upstate NY
(4.2 per 10,000). For the 15–19 age category, the hospitalization rate for self-inflicted injury was 14.5
per 10,000 in Broome County, and was significantly higher than both NYS (7.6 per 10,000) and Upstate
NY (8.7 per 10,000). Broome County was ranked in the fourth quartile overall and in the 15-19 age group
(Appendices C107-C109). The age-adjusted assault-related hospitalization rate in Broome County (2.9
per 10,000) was similar to NYS (3.2 per 10,000) and slightly higher than Upstate NY (2.2 per 10,000).
Broome County was ranked in the fourth quartile for this indicator (Appendices C110-C111).
Healthy People 2020 Objectives — Injury Prevention
IVP-9 Prevent an increase in poisoning deaths.
IVP-9.1 Among all persons (13.1 deaths per 100,000 population)
IVP-11 Reduce unintentional injury deaths.
Target: 36.0 deaths per 100,000 population
IVP-12 Reduce nonfatal unintentional injuries.
Target: 9.2 deaths per 100,000 population
IVP-13 Reduce motor vehicle crash-related deaths.
IVP-13.1 12.4 deaths per 100,000 population
IVP 23 Prevent an increase in fall-related deaths.
IVP-23.2 Among adults age 65 and older (45.3 deaths per 100,000 population)
OA-11 Reduce the rate of emergency department (ED) visits due to falls among older adults.
Target: 4,711.6 ED visits per 100,000
IVP-29 Reduce homicides.
Target: 5.5 homicides per 100,000 population

Broome County
Community Health Assessment 2019-2024 43
For unintentional injuries, the age-adjusted mortality rate per 100,000 in Broome County from 2014-
2016 was 50.2 per 100,000 and was significantly higher than both NYS (30.2 per 100,000) and Upstate
NY (41.7 per 100,000). Broome County ranked in the fourth quartile for this indicator. The age-adjusted
hospitalization rate for unintentional injuries in Broome County was 72.0 per 10,000, which was
significantly higher than NYS and Upstate NY (55.7 and 57.0 respectively) and Broome County was
ranked in the fourth quartile for this indicator. The unintentional injury hospitalization rate was highest
in the 65 years and older age category (312.6 per 10,000), significantly higher than both NYS (260.9) and
Upstate NY (239.3). The unintentional injury hospitalization rate was also high in the 25–64 age group
(61.8 per 10,000) and was statistically higher than statewide rates NYS (41.3) and Upstate NY (42.7). The
unintentional injury hospitalization rate was lowest in 10-14 age group (12.3 per 10,000) and slightly
lower rates were observed for Broome County in the 15-24 age bracket (18.5 per 100,000) compared
with 23.1 per 100,000 for both NYS and Upstate NY (Appendices C112-C122).
In Broome County, the age-adjusted hospitalization rate for poisoning was 10.0 per 10,000 from 2014-
2016 and was significantly higher than both NYS (6.9) and Upstate NY (7.0). For this indicator, Broome
County ranked in the fourth quartile. For traumatic brain injury, the age-adjusted hospitalization rate
was 7.8 per 10,000 from 2014-2016 and was similar to the state averages (Appendices C140-C141).
Notably, the age-adjusted hospitalization rates for self-inflicted injury have shown a decrease in Broome
County from 2012- 2014 from 11.6 in 2012 to 8.0 in 2014. Similar trends were observed for
unintentional injury hospitalizations among those age 25-64 years as well as 65 and older. Finally, the
age-adjusted hospitalization rate for poisoning from 2012-2014 trended downward from 16.2 in 2012 to
10.2 in 2014. Although these rates appear to trend downward between 2012-2016, valid interpretations
cannot be made to the change in ICD codes. Despite these limitations in the trend data, the significantly
higher rates for the various injury indicators for Broome County when compared to NYS should suggest
that efforts be focused on improving mental and emotional health in Broome County.
The age-adjusted hospitalization rate related to falls was slightly higher for Broome County than for the
state (36.1 per 10,000 vs 32.2 or NYS and 32.8 for Upstate NY). Broome County ranked in the fourth
quartile for this indicator. The rates of fall hospitalizations for age <10 and age 10-15 were lower in
Broome County than in NYS. For the three oldest age groups (65–74, 75–84, and 85+ years), the
hospitalization rates were higher than NYS, and these differences were significant for those 65-74 and
85+ years of age. Broome County ranked in the first quartile for fall hospitalizations among children age
10-14 years. The county ranked in the fourth quartile for falls hospitalizations for ages 25-64, 65-74, 75-
84, and 85+. Trends in fall-related hospitalizations across multiple age groups appear in Appendix C124-
C133. In general, no appreciable patterns were observed for younger age groups. In 2016, the
percentage of adults who had a fall that resulted in an injury in Broome County was significantly higher
(59.3%) when compared with NYS (42.0%). For falls occurring in the past 12 months, females age 65+
experienced a higher percentage of falls when compared with males (32.8% vs. 28.8%). Again, due to
the change in ICD codes, assessment of trends in fall hospitalization rates from 2014-2016 cannot be
made. However, due to the significant differences between falls resulting in injury in Broome County for
2016 compared with NYS, and other 2016 data showing higher percentages of falls among various age
groups, it is apparent that continuing effort is needed to reduce falls among residents of Broome
County.

Broome County
44 Community Health Assessment 2019-2024
Basic Service Area: Disease Control
Sexually Transmitted Diseases
Information on sexually transmitted diseases (STDs) appears in Appendices D1-D35. For the time period
2014-2016, there were 26 cases of early syphilis (primary, secondary or latent of less than one-year
duration) in Broome County, which corresponds to a rate of 4.4 cases per 100,000 population. This rate
was significantly lower than for NYS or Upstate NY (25.1 and 9.1 respectively). Because of the small
number of cases, the local rate is considered unstable and demonstrates more fluctuation over time
(Appendices D14 & D15). This rate is just slightly above the Healthy People 2020 objective of 1.7 cases
per 100,000 population.
For gonorrhea, there was a 3-year total (2014-2016) of 234 cases across all age groups for males (199.3
per 100,00 population) and 198 for females (174.3 per 100,000 population). These indicators were
mostly similar to NYS and Upstate NY. For the 15–19 age group specifically, there was a total of 46 cases
for a case rate of 144 per 100,000 population, which was significantly lower than NYS (305.8 per
100,000) and Upstate NY (238.3 per 100,000). Broome County was in the second quartile for early
syphilis and in the fourth quartile for gonorrhea in both genders (age 15-44 years). For gonorrhea among
15–19 year-olds, Broome County ranked in the third quartile. The gonorrhea rate in Broome County is
well below the Healthy People 2020 rate of 251.9 per 100,000 population. Gonorrhea rates had
decreased in 2004 and 2005, increased significantly between 2007 and 2014, and appears to have
leveled off. (Appendices D16-D21).
Healthy People 2020 Objectives — Sexually Transmitted Diseases
STD-1 Reduce the proportion of adolescents and young adults with Chlamydia trachomatis
infections.
STD 1.1 Females aged 15 to 24 years attending family planning clinics (6.7%)
STD 1.2. Females aged 24 years and under enrolled in National Job Training Program (11.5%)
STD 1.3 Males aged 24 years and under enrolled in National Job Training Program (6.3%)
STD-5 Reduce the proportion of females aged 15-44 years who have ever required treatment for
pelvic inflammatory disease (PID)
Target: 3.8%
STD-6 Reduce gonorrhea rates.
STD 6.1 Females aged 15 to 44 years (251.9 new cases per 100,000 population)
STD-7 Reduce sustained domestic transmission of primary and secondary syphilis.
STD 7.1 Females (1.3 new cases per 100,000 population)
STD 7.2 Males (6.7 new cases per 100,000 population)

Broome County
Community Health Assessment 2019-2024 45
For this same time period, there were 700 cases of Chlamydia among males and 1,312 cases among
females (age 15-44 years). For males, this equates to a case rate of 596.3 per 100,000 population, which
was significantly lower than NYS (875.7 per 100,000) but not Upstate NY (618.0 per 100,000). For
females, this equates to a case rate of 1,155 per 100,000 population, which was also significantly lower
than both NYS (1,577.4) and Upstate NY (1,351.6). Among males in the 15–19 age group and 20–24 age
group, case rates were appreciably higher (499.4 per 100,000 and 918.2 per 100,000 respectively). For
females, the age-specific rates were 2,080.8 per 100,000 for 15–19 year-olds and 1,795.7 per 100,000
for 20–24 year-olds. For both males and females across all age categories, the Chlamydia rate was
significantly lower than statewide rates. The Chlamydia rates for males placed Broome County in the
fourth quartile for the 15-44 age group, the third quartile for the 15-19 age group, and the second
quartile for the 20-24 age group. For females, Broome County ranked in the second (ages 20-24, and 15-
44 years) or third quartile (age 15-19) among NYS counties. Chlamydia rates have been steadily climbing
for males, though at a slower rate for Broome County than for NYS overall and remained relatively
stable for females (Appendices D22-D33).
The pelvic inflammatory disease (PID) hospitalization rate for Broome County was suppressed between
2014 and 2016 (see Appendix D34 & D35).
Tuberculosis
The incidence of tuberculosis in Broome County ranked in the third quartile for the state at a rate of 1.0
per 100,000 population (excluding prison inmates) representing only 6 cases for the 3-year period 2014–
2016 (see Appendices D36 & D51-D52). The tuberculosis rate in NYS was 3.9 per 100,000, which is
clearly much higher than the county. In this area, Broome County ranked in the third quartile. Because
of the small number of cases (<20), the rate is considered unstable and demonstrates more fluctuation
over time. The incidence of tuberculosis infection met the Healthy People 2020 objective of 1.0 new
case per 100,000 population.
Healthy People 2020 Objectives — Tuberculosis
IID-29 Reduce tuberculosis.
Target: 1.0 new case per 100,000 population

Broome County
46 Community Health Assessment 2019-2024
Communicable Diseases
Pertussis
In Broome County, from 2014 to 2016, the incidence of pertussis (whooping cough) was 3.4 per 100,000
with a total of 20 cases (see Appendices D30 & D39-D40). This rate was slightly lower than the rate for
NYS (5.1 per 100,000) and significantly lower than Upstate NY (5.9 per 100,000). For pertussis incidence,
Broome County ranked in the second quartile. Trend data from 2001 to 2016 reveal three spikes. One
outbreak occurred during 2004 when the incidence rose to 56.1 per 100,000 population, another during
2006 with an incidence of 23.4 per 100,000, and the most recent spike occurred in 2012 with an
incidence of 49.5 per 100,000. Rates have remained low since 2013. Pertussis is spread through airborne
contact with respiratory droplets or discharges. Most fatalities occur in children less than 1 year of age,
and even then the case fatality rate is low. Pertussis is a vaccine-preventable disease but protection
often only lasts through childhood. A resurgence of disease in adults and adolescents poses a public
health threat to infants who have not been vaccinated.
Mumps
In Broome County from 2014 to 2016, there were 2 reported case of mumps for a crude rate of 0.34 per
100,000 (Appendices D36 & D41-D42). The incidence rate was 1.1 per 100,000 for NYS and 1.9 per
100,000 for Upstate NY. The low number of cases results in an unstable rate and meaningful
comparisons to statewide rates cannot be made. Although trend data from 2001 to 2016 reveals a small
increase in 2007, the incidence of mumps has remained very low for most of this period.
Meningococcal Disease
In Broome County from 2014 to 2016, there were 4 reported cases of meningococcal disease (Appendix
D36 & D43-D44). This rate was 0.7 per 100,000 for Broome County as compared to 0.1 per 100,000 for
Healthy People 2020 Objectives — Communicable Diseases
IID-3 Reduce meningococcal disease.
Target: 1,094 cases per 100,000 population
IID-23 Reduce hepatitis A.
Target: 0.3 cases per 100,000 population
IID-25 Reduce hepatitis B.
Target: 1.3 cases per 100,000 population (age 19 and older)
IID-26 Reduce new hepatitis C infections.
Target: 0.25 new cases per 100,000 population
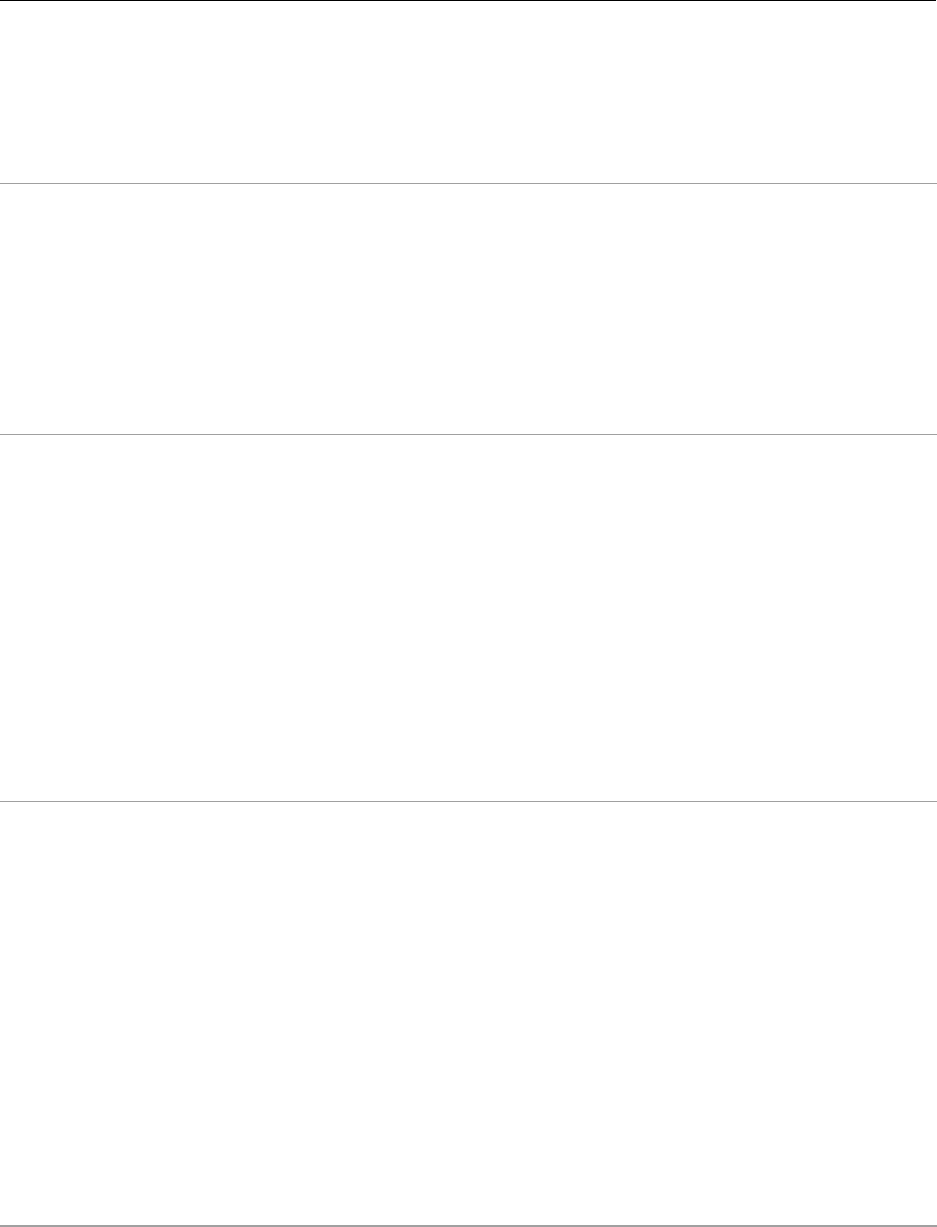
Broome County
Community Health Assessment 2019-2024 47
both NYS and Upstate NY. The low number of cases results in an unstable rate and meaningful
comparisons to statewide rates cannot be made. Although trend data between 2001 and 2016 show
considerable variability, the three-year averages suggest that there has been a general upward trend in
incidence between 2005 and 2016.
Haemophilus influenzae
Haemophilus influenzae type b (Hib) causes infections of the blood, pneumonia, and acute bacterial
meningitis. Fifteen cases of Haemophilus influenzae were diagnosed during 2014 to 2016 in Broome
County for an incidence of 2.5 per 100,000 population (Appendices D36 & D45-D46). It is just slightly
higher than the rates observed across NYS (1.5) and Upstate NY (2.1). Immunization against Hib can
reduce the incidence of invasive diseases and, in particular, early childhood meningitis.
Hepatitis A
Hepatitis A is an acute, self-limiting infectious disease caused by the Hepatitis A virus (HAV), which is
transmitted by the fecal-oral route via contaminated food or drinking water. This illness is often
associated with travel to areas with poor hygiene standards. Infection with the virus confers lifelong
immunity and can be prevented by vaccination. From 2014 to 2016, there was only one reported case of
Hepatitis A in Broome County with an incidence 0.2 per 100,000 population, which was similar to the
rate for NYS (0.5) and Upstate NY (0.4). The low number of cases results in an unstable rate. Broome
County ranked in the first quartile among NYS counties for this metric. Trend data shows the rare
instances of cases from 2006-2016. The rate was lower than the Healthy People 2020 objective for this
indicator (0.3 per 100,000 population). (Appendices D36 & D47-D48)
Hepatitis B
Hepatitis B is caused by infection with the Hepatitis B virus (HBV) and transmission results from
exposure to infectious blood or body fluids via unprotected sexual contact, blood transfusions, re-use of
contaminated needles and syringes, and vertical transmission from mother to child during childbirth.
The disease causes an inflammation of the liver that can result in cirrhosis or cancer and potentially
death. This infection may be acute or chronic and can be prevented by administering a series of
vaccinations. Post-exposure prophylaxis with immunoglobulin is also available. From 2014 to 2016,
three cases of Hepatitis B were diagnosed in Broome County (Appendices D36 & D49-D50). Due to the
small number of cases, the incidence rate of 0.5 per 100,000 population is unstable and trend data
shows considerable variability. Broome County ranked in the second quartile with statewide rates just
slightly higher. The overall incidence was lower than the Healthy People 2020 target of 1.3 cases per
100,000 population.

Broome County
48 Community Health Assessment 2019-2024
Escherichia coli
Infection with Escherichia coli O157:H7, a foodborne illness, can cause severe bloody diarrhea and may
result in acute kidney failure from destruction of red blood cells. The young and elderly are particularly
susceptible with E. coli being the leading cause of kidney failure in children. A major source of infection
is undercooked ground beef. From 2014 to 2016, 15 cases of E. coli were diagnosed in Broome County
(Appendices D36 & D53-D54) yielding an incidence rate of 2.5 per 100,000 population. Broome County
ranked in the fourth quartile, and this rate was slightly higher than statewide rates. The incidence of E.
coli demonstrates considerable variability over time due to the small number of cases with minor
outbreaks evident in 2014, 2015, and 2016.
Salmonella
Salmonella infection may be caused by a number of different species which are pathogenic for both
animals and humans causing acute abdominal pain and diarrhea. Salmonellosis is considered a
foodborne illness and often goes unrecognized unless a point source outbreak occurs. Transmission can
be prevented by avoiding raw or undercooked eggs, poultry, and meat. For 2014–2016, there were 50
cases of Salmonella in Broome County. The incidence of salmonella infection was 8.5 per 100,000, which
was significantly lower than NYS (11.6 per 100,000) or Upstate NY (12.0 per 100,000). Trend data
suggests that the number of cases for salmonella has been decreasing since 2004. Broome County
ranked in the first quartile for this indicator (see Appendices D30 & D48-D49).
Shigellosis
Shigellosis infection also involves a number of different species and causes an acute bacterial diarrhea.
Transmission occurs via the fecal-oral route and prevention is directed at isolation during acute illness
and through safe food handling and hand hygiene. The incidence of Shigella (3-year estimate) in Broome
County was 1.4 per 100,000 population with 8 cases reported between 2014-2016. This rate was
significantly lower than both NYS (3.9 per 100,000) and Upstate NY (2.0 per 100,000). The small number
of cases results in an unstable rate with variability from small fluctuations in the number of cases
(Appendices D36 & D57-D58).
Lyme disease
Lyme disease, a tick-borne zoonosis caused by Borrelia burgdorferi, is characterized by a distinctive skin
lesion and has systemic neurologic, rheumatologic, and cardiac manifestations. Seasonal and geographic
patterns are evident with initial infection occurring primarily during summer months in the Northeastern
US. The 3-year estimate (2014-2016) of Lyme disease incidence for Broome County was 109.8 per
100,000 resulting from a reported 647 cases (Appendices D36 & D59). This rate was three times the rate
for NYS (38.0 per 100,000) though was similar to Upstate NY (110.3 per 100,000). Broome County
ranked in the fourth quartile for this indicator.

Broome County
Community Health Assessment 2019-2024 49
Pneumonia and Influenza
Comparison of pneumonia and influenza hospitalization rates among those 65 and older were higher for
Broome County than for NYS and Upstate NY (108.9 per 10,000 vs. 87.3 and 93.7 respectively)
(Appendices D36-D37). In comparison to other counties in the state, Broome County was in the third
quartile with a total of 389 hospitalizations for the 2014-2016 period. These data reflect International
Classification of Diseases (ICD) codes 480–487.
Immunizations
Information about immunizations for adults is located in Appendices D62-D66. For Broome County in
2016, the percent of adults age 65 and over who received a flu shot in the past year was 55.8% but was
significantly different than the 59.5% for NYS or 59.6% for Upstate NY. The percent of adults age 65 and
older who have ever received the pneumococcal pneumonia vaccine was 70.3% for Broome County,
which was also similar to NYS (69.3%) and Upstate NY (73.8%). While these proportions ranked Broome
County in the second and third quartiles respectively, they were well below the Healthy People 2020
objective of 90% and the Prevention Agenda 2017 objective of 66.2% for flu immunization among adults
age 65 and older.
Healthy People 2020 Objectives — Immunizations
IID-12 Increase the percentage of children and adults who are vaccinated annually against seasonal
influenza.
IID12.1 Children age 6 to 23 months (80%)
IID12.2 Children age 2 to 4 years (80%)
IID12.3 Children age 5 to 12 years (80%)
IID12.4 Children age 13-17 years (80%)
IID12.5 Noninstitutionaled adults age 18 to 64 (80%)
IID12.6 Noninstitutionaled high-risk adults age 18 to 64 (90%)
IID12.7 Noninstitutionaled adults age 65 and older (90%)
IID12.8 Institutionaled adults age 18 and older (90%)
IID12.9 Healthcare personnel (90%)
IID12.10 Pregnant women (80%)
IID-13 Increase the percentage of adults who are vaccinated against pneumococcal disease.
IID-13.1 Pneumococcal vaccine (90%)

Broome County
50 Community Health Assessment 2019-2024
Chronic Diseases: Cancer
Cancer data are presented in Appendices D67-D151. These data are based on select County Health
Assessment Indicators from the NYS Department of Health which are drawn from the NYS Cancer
Registry for the years 2013-2015. Early stage cancer is defined as invasive cancers that are limited to the
tissue of origin. Small area analyses were available for colorectal, lung, breast and prostate cancers.
These analyses calculated the expected incidence as the number of people in a given zip code that
would be expected to develop cancer within a 5-year period if the zip code had the same rate of cancer
as the state as a whole. Zip codes with small numbers are combined with larger neighboring zip codes.
Each year an estimated 1,229 people are diagnosed with cancer, and it is responsible for 432 deaths per
year in Broome County. Incidence and mortality is somewhat higher for males than females. Between
2000 and 2015, overall cancer rates in Broome County remained relatively stable. For the period 2013-
2015, the crude mortality from all cancers was 218.7 per 100,000 population and the age-adjusted
mortality was 156.9 per 100,000 population. Although the overall rate is significantly higher than NYS as
a whole (149.2 per 100,000), it ranks Broome County in the third quartile. The crude rate is higher than
the Healthy People 2020 objective of 160.6 deaths per 100,000 population.
Healthy People 2020 Objectives — Cancer
C-1 Reduce the overall cancer death rate.
Target: 160.6 deaths per 100,000 population
C-2 Reduce the lung cancer death rate.
Target: 45.5 deaths per 100,000 population
C-3 Reduce the female breast cancer death rate.
Target: 20.6 deaths per 100,000 females
C-4 Reduce the death rate from cancer of the uterine cervix.
Target: 2.2 deaths per 100,000 females
C-5 Reduce the colorectal cancer death rate.
Target: 14.5 deaths per 100,000 population
C-6 Reduce the oropharyngeal cancer death rate.
Target: 2.3 deaths per 100,000 population
C-7 Reduce the prostate cancer death rate.
Target: 21.2 deaths per 100,000 males
C-8 Reduce the rate of melanoma cancer deaths.
Target: 2.4 deaths per 100,000 population
C-11 Reduce late stage female breast cancer.
Target: 41.0 new cases per 100,000 females

Broome County
Community Health Assessment 2019-2024 51
Cancer incidence and mortality by gender are provided in Appendices D68-D70. The greatest burden of
disease based on absolute number of cases results from prostate cancer in men with an average 120
cases per year and breast cancer in women, with an average 184 cases per year. An estimated 46
persons are diagnosed each year with colon, rectal, or colorectal cancer and 89 persons with lung
cancer. Lung cancer is responsible for an estimated 110 deaths per year; colon, rectal, or colorectal
cancer for 38 deaths per year; breast cancer for 28 deaths per year in women and prostate cancer for 20
deaths per year in men.
For the period 2013-2015, the incidence of cancer of the oral cavity and pharynx was 16.7 per 100,000
for Broome County (third quartile) and the age-adjusted mortality rate was 2.5 per 100,000. Incidence
rates were significantly higher than NYS (10.9 per 100,000). Early diagnosis occurs in about one-third of
cases for both males and females. The age-adjusted mortality was slightly higher than the Healthy
People 2020 objective of 2.3 per 100,000 population. (Appendices D79-D86)
For colorectal cancer in Broome County, the age-adjusted incidence rate was 34.7 per 100,000
(first/second quartile) and the age-adjusted mortality rate was 13.9 per 100,000 (third quartile) for the
period 2013-2015. The age-adjusted incidence rate for Broome is less than NYS and Upstate (39.3 and
37.2 respectively). Almost half of all colorectal cancers are diagnosed at an early stage for both males
and females. For the period 2000-2015, both the incidence and mortality have been relatively stable.
Colorectal cancer mortality was lower than the Healthy People 2020 objective of 14.5 per 100,000
population.
In Broome County, the age-adjusted incidence of cancer of the lung and bronchus was higher than NYS
(66.2 vs. 59.2 per 100,000). Broome County was similar to Upstate NY and ranked in the first/second
quartile statewide. Only about 15% of lung cancers are diagnosed at an early stage. Lung and bronchial
cancer mortality was not significantly higher in Broome County (40.3 per 100,000 population) than for
NYS (36.9 per 100,000). County rankings within the state placed Broome County in the second quartile.
Both the incidence and mortality remained level over the period 2013-2015. Broome County is currently
meeting the Healthy People 2020 objective of reducing the lung cancer death rate to below 45.5 per
100,000 population. The incidence of lung and bronchial cancer among males was 67.0 per 100,000 as
compared to 53.2 per 100,000 among females. Gender-specific mortality rates were 44.5 per 100,000
for males and 30.8 per 100,000 for females. (Appendices D99-D106)
Broome County ranked in the third quartile for mortality from melanoma, a highly malignant form of
skin cancer. The mortality rate for Broome County was 2.4 per 100,000 population compared to the NYS
rate of 2.3 per 100,000. In this area, Broome County did meet the Healthy People 2020 objective of 2.4
per 100,000. Melanoma incidence was nearly twice as high for males as for females (23.2 vs. 14.6 per
100,000) and two times as high for mortality (2.9 vs. 1.3 per 100,000). Given the small number of deaths
(n=14), these rates should be interpreted cautiously. Fortunately, given the aggressive nature of this
form of cancer, approximately 83.3% of malignant melanomas are diagnosed at an early stage.
(Appendices D95-D98)
The age-adjusted incidence of female breast cancer in Broome County was 143.0 per 100,000 females,
which was higher than NYS (132.8) and not significantly different from Upstate NY (133.8). More than
two-thirds of these are diagnosed at an early stage. The age-adjusted mortality rate for female breast
cancer was 20.1 per 100,000 and was similar to both NYS and Upstate NY. Broome County has met the

Broome County
52 Community Health Assessment 2019-2024
Healthy People 2020 objective of reducing the female breast cancer death rate to less than 20.6 per
100,000. In Broome County, only 43.0 per 100,000 female breast cancers were diagnosed at a late stage
(similar to NYS and Upstate NY), which was also above the incidence set by Healthy People 2020 of less
than 41.0 new cases per 100,000 females. Broome County ranked in the third quartile for incidence and
in the fourth quartile for mortality and late stage diagnosis. (Appendices D107-D118)
Broome County ranked in the first and third quartile for age-adjusted incidence of cancer of the cervix or
uterus (6.0 per 100,000) and age-adjusted mortality (2.0 per 100,000). Compared to NYS, Broome
County experienced similar rates and no temporal pattern was evident. Though the number of deaths
due to this type of cancer was small, making the mortality rate unstable, it was nonetheless below the
target rate of 2.2 per 100,000 females set by Healthy People 2020. Broome County ranked in the third
quartile for age-adjusted incidence of ovarian cancer (13.4 per 100,000 females) and in the first quartile
for age-adjusted mortality (5.4 per 100,000 females). The incidence for Broome County was higher than
both Upstate NY and NYS (12.2 per 100,000 for both). Early stage diagnosis for cervical and uterine
cancer is 50.0% and 78.1% respectively. In comparison, prompt diagnosis of ovarian cancer remains
elusive with only 19.4% of cases being recognized in its earliest stages. (Appendices D119-D126 for
cervical cancer and D127-D134 for ovarian cancer)
The age-adjusted incidence of prostate cancer in Broome County was 88.2 per 100,000 males, and this
figure was significantly lower than NYS (123.4) and Upstate NY (122.2). This rate placed the county in the
first/second quartile. Prostate cancer has the highest rate of early diagnosis at almost 90%. The age
adjusted prostate cancer mortality was 16.6 per 100,000 males, which was similar to NYS and Upstate
NY, ranking Broome County in the first/second quartile. Diagnosis of prostate cancer at a late stage
occurred at for 5.8 per 100,000 males, which was similar to NYS and Upstate NY. Broome County is
currently meeting the Healthy People 2020 objective of reducing the prostate cancer death rate to
below 21.2 per 100,000 males. (see Appendices D135-D146)
Information about childhood cancers can be found in Appendices D147-D151. The overall incidence of
childhood cancer is lower for Broome County (200.0 per 100,000 children age 0–19) than NYS (213.9 per
100,000) and Upstate NY (213.5 per 100,000). In NYS, the most common cancers in children age 0–4 are
leukemias, malignant central nervous system tumors, and renal tumors. For children aged 5–9, cancers
with the highest incidence are leukemias, non-Hodgkin lymphomas, soft tissue sarcomas, and malignant
bone tumors. For children aged 10-14 and 15-19, cancers with the highest incidence are leukemias,
lymphomas, soft tissue and osteosarcomas. In addition, for children aged 15–19, gonadal neoplasms are
more common than for younger aged children. Cancer is responsible for approximately 30–40 deaths
per year in NYS. Across all age groups, childhood cancers with the highest mortality are leukemias and
malignant central nervous system tumors. In the 15–19 year-old age group, tumors of the bones and
joints also have a relatively high mortality, but in all cases the rate does not exceed 10 deaths per
100,000 children.

Broome County
Community Health Assessment 2019-2024 53
Chronic Diseases: Cardiovascular Disease
Data for cardiovascular disease mortality and morbidity appear in Appendices D152-D200 and are based
on selected County Health Assessment Indicators for 2014-2016 from the NYS Department of Health.
Mortality data are derived from Vital Records and morbidity from the Statewide Planning and Research
Cooperative System (SPARCS) both located at the Bureau of Biometrics and Health Data, NYS
Department of Health. The category of cardiovascular disease includes International Statistical
Classification of Diseases and Related Health Problems 10th Revision (ICD-10) codes I00–I99. Disease of
the heart include ICD-10 codes for rheumatic heart disease (codes I00–I09), hypertensive heart disease
(code I11), hypertensive heart disease and hypertensive renal disease (code I13), ischemic heart
disease, coronary heart disease and disease of pulmonary circulation, pericarditis and endocarditis, and
cardiomyopathies (codes I20– I51).
In Broome County, cardiovascular disease is responsible for an average of 654 deaths per year, almost
twice as many as for all cancers combined, and is the leading cause of death. Specific data for crude and
age-adjusted mortality rates were presented previously and will not be repeated here. Rather, this
section will describe in greater detail premature deaths (ages 35–64) and pre-transport mortality as well
as hospitalization rates.
The mortality rate for premature death is higher in Broome County than in NYS for all cardiovascular
diseases (132.4 vs. 102.4 per 100,000), for diseases of the heart (107.6 vs. 83.4 per 100,000), and for
coronary heart disease (68.9 vs. 66.4 per 100,000). These differences are significant for all
cardiovascular disease and diseases of the heart, but not for coronary heart disease. Moreover, the
mortality rate for premature death was significantly higher in Broome County than Upstate NY in all
three categories. Premature death from heart failure is relatively uncommon; and there were only 8
cases in Broome County over the 3-year period from 2014-2016. Since these rates are age specific rates,
differences in premature death are not likely accounted for by variability in age distribution of the
populations.
Healthy People 2020 Objectives — Cardiovascular Disease
HDS-2 Reduce coronary heart disease deaths.
Target: 100.8 deaths per 100,000 population
HDS-24 Reduce hospitalizations of older adults with congestive heart failure as the principal
diagnosis.
HDS-24.1 Adults aged 65 to 74 years (8.8 per 1,000 population)
HDS-24.2 Adults aged 75 to 84 years (20.2 per 1,000 population)
HDS-24.3 Adults aged 85 years and older (38.6 per 1,000 population)
HDS-12 Reduce the proportion of adults with hypertension whose blood pressure is under control.
Target: 61.2%
HDS-20 Increase the proportion of adults with coronary heart disease who have their low density
lipoprotein (LDL)-cholesterol at or below recommended levels.
Target: Developmental

Broome County
54 Community Health Assessment 2019-2024
In relation to pre-transport mortality, the rates were significantly higher in Broome County than NYS for
all cardiovascular diseases (207.7 vs. 153.2 per 100,000), for diseases of the heart (170.7 vs. 131.0 per
100,000), and for coronary heart disease (110.0vs. 105.0 per 100,000). Because of the large distances
required for emergency responders to reach rural county residents, response times in these areas are
typically longer. Thus, comparisons against Upstate NY rates may be more appropriate. Even considering
similar geography; however, premature death from all cardiovascular disease, diseases of the heart,
coronary heart disease, and heart failure are significantly higher in Broome County relative to the rest of
the state. Broome County ranked in the third and fourth quartile for nearly all indicators. This finding
suggests that there may be reasons, other than rurality that account for the higher pre-transport
mortality rates.
Disparities in hospitalizations for cardiovascular disease were previously described. This section will
discuss cardiovascular morbidity in relation to the county as a whole. On average in Broome County,
there are 3,239 hospitalizations per year related to cardiovascular disease, 2,152 hospitalizations per
year for diseases of the heart, 732 hospitalizations per year for coronary heart disease, and 508
hospitalizations per year for heart failure. Age-adjusted hospitalization rates in Broome County are
significantly lower than both NYS and Upstate NY for all comparison categories. The age-adjusted
hospitalization rate for all cardiovascular disease was 123.1 per 10,000 for Broome County versus 125.6
for NYS and 120.3 for Upstate NY. For diseases of the heart, the age-adjusted hospitalization rate for
Broome County was 81.7 per 10,000 versus 83.7 for NYS and 81.6 for Upstate NY. For coronary heart
disease, the age-adjusted hospitalization rate for Broome County was 28.7 per 10,000 versus 29.0 for
NYS and 27.4 for Upstate NY. And finally for heart failure, the age-adjusted hospitalization rate for
Broome County was 18.0 per 10,000 versus 20.4 for NYS and 19.4 for Upstate NY. In relation to the
county rankings within NYS, Broome County placed in the second and third quartile for many
cardiovascular hospitalization rate indicators. Broome County did not meet the Prevention Agenda 2017
targets in relation to the age-adjusted heart attack hospitalization rate (19.3 vs. 14.0 per 10,000).
Hospitalization rates for this disease are considered “ambulatory sensitive” meaning that, with
appropriate outpatient management, hospitalization may be avoidable. Healthy People 2020 provides
only age-specific targets for congestive heart failure and not overall, but comparison indicates that the
hospitalization rate for this condition in Broome County would only meet the current objective if all or
most of the hospitalizations were among residents age 85 or older. While Broome County outperformed
NYS on hospitalization rates and both hospitalization and mortality rates appear to be declining, the
number of deaths per year and high mortality rates warrant continued focus on the cardiovascular
health of Broome County residents.

Broome County
Community Health Assessment 2019-2024 55
Chronic Diseases: Cerebrovascular Disease (Stroke)
Data for cerebrovascular disease mortality and morbidity appear in Appendices D201-D215 and are
based on selected County Health Assessment Indicators for 2014 to 2016 from the NYS Department of
Health. Mortality data are derived from Vital Records and morbidity from the Statewide Planning and
Research Cooperative System (SPARCS) both located at the Bureau of Biometrics and Health Data, NYS
Department of Health. The category of cerebrovascular disease includes ICD-10 codes I60–I69.
In Broome County, approximately 81 deaths per year are attributable to cerebrovascular disease and
there is an average 598 hospitalizations each year. The age-adjusted mortality rate in Broome County
was 27.5 per 100,000 population and was higher than both NYS (25.6 per 100,000) and lower than
Upstate NY (29.1 per 100,000). Broome County ranked in the first quartile for age-adjusted
cerebrovascular mortality and has met the Healthy People 2020 objective of 33.8 deaths per 100,000.
The pre-transport cerebrovascular disease mortality rate for Broome County (18.8 per 100,000) was
significantly higher than for NYS (12.4 per 100,000) and similar to Upstate NY (17.4 per 100,000).
Broome County ranked in the third quartile in the state for this indicator. The age-adjusted
hospitalization rate for cerebrovascular disease was 22.3 per 10,000 population in Broome County,
which was higher than both NYS (21.2 per 10,000) and Upstate NY (20.8 per 10,000). Broome County
ranked in the third quartile for this indicator. The high pre-transport mortality for stroke suggests that a
focus on public health interventions directed toward raising awareness of stroke symptoms, early
recognition of evolving stroke, and early activation of emergency medical services continue to be critical
public health messages.
Healthy People 2020 Objectives — Cerebrovascular Disease
HDS-3 Reduce stroke deaths.
Target: 33.8 deaths per 100,000 population

Broome County
56 Community Health Assessment 2019-2024
Healthy People 2020 Objectives — Diabetes Mellitus
D-1 Reduce the annual number of new cases of diagnosed diabetes in the population.
Target: 7.2 new cases per 1,000 population age 18-84
D-3 Reduce the diabetes death rate.
Target: 65.8 deaths per 100,000 population
D-4 Reduce the rate of lower extremity amputations in persons with diagnosed diabetes.
Target: [not applicable]
D-5 Improve glycemic control among persons with diabetes
D-5.1 Reduce the proportion of persons with diabetes with an A1c value greater than 9%
D-5.2 Increase the proportion of the diabetic population with an A1c value < 7%
D-6 Improve lipid control among persons with diagnosed diabetes.
Target: 58.4%
D-7 Increase the proportion of persons with diagnosed diabetes whose blood pressure is under
control.
Target: 57.0%
D-8 Increase the proportion of persons with diagnosed diabetes who have at least an annual
dental examination.
Target: 61.2%
D-9 Increase the proportion of adults with diabetes who have at least an annual foot
examination.
Target: 74.8%
D-10 Increase the proportion of adults with diabetes who have an annual dilated eye
examination.
Target: 58.7%
D-11 Increase the proportion of adults with diabetes who have a glycosylated hemoglobin
measurement at least twice a year.
Target: 71.1%
D-12 Increase the proportion of persons with diagnosed diabetes who obtain an annual
microalbumin measurement.
Target: 71.1%
D-13 Increase the proportion of adults with diabetes who perform self-blood glucose-monitoring
at least once daily.
Target: 70.4%
D-14 Increase the proportion of persons with diagnosed diabetes who receive formal diabetes
education.
Target: 62.5%
D-15 Increase the proportion of persons with diagnosed diabetes whose condition has been
diagnosed.
Target: 80.1%

Broome County
Community Health Assessment 2019-2024 57
Chronic Diseases: Diabetes Mellitus
Data for diabetes mortality and morbidity appear in Appendices D216 and D225-D239. These data are
based on selected County Health Assessment Indicators for 2014 to 2016 from the NYS Department of
Health. Mortality and morbidity data sources have been previously described. The ICD-10 codes for
diabetes mellitus mortality include E10 to E14.
In Broome County, there is an average of 56 deaths per year due to diabetes mellitus. The age-adjusted
diabetes mortality rate was estimated to be 20.6 per 100,000 population, and this rate was higher than
both NYS (17.0 per 100,000) and Upstate NY (15.4 per 100,000). Among NYS counties, Broome County
ranked in the third quartile for diabetes. The diabetes mortality was less than the 65.8 deaths per
100,000 population objective set by Healthy People 2020.
The average number of hospitalizations per year was 350 for diabetes as a primary (admitting) diagnosis
and 4,971 for any diabetes diagnostic code associated with the hospitalization. The age-adjusted
hospitalization rate for those with a primary (admitting) diagnosis of diabetes was 16.7 per 10,000
population compared with 15.9 per 10,000 for NYS and 13.8 per 10,000 for Upstate NY. The age-
adjusted hospitalization rate for those with any diagnosis of diabetes was 213.2 per 10,000 population
for Broome County compared to 209.9 per 10,000 for NYS and 188.9 per 10,000 for Upstate NY. In both
of these areas (primary or any diagnosis of diabetes), Broome County was higher than both NYS and
Upstate NY for hospitalizations of individuals with diabetes.
Based on the BRFSS conducted by NYS in 2016, the age-adjusted prevalence of diabetes among adults in
Broome County was 8.6%, which is somewhat lower than the 9.5% for NYS. In relation to diabetes
prevalence, Broome County ranked in the second quartile. Based on Prevention Agenda 2017 indicators,
the hospitalization rate for short-term complications of diabetes among 6-17 year-old children was 5.4
per 10,000 for Broome County between 2014-2016 which was higher than NYS (3.2 per 10,000) and
higher than the target of 3.06 per 10,000 set by the NYS Department of Health. For short-term
complications among adults age 18 or older, the hospitalization rate for short-term complications of
diabetes was 6.4 per 10,000 as compared to 4.0 for NYS and the target of 4.86 in the NYS Prevention
Agenda 2017. While the hospitalization rates for diabetes as a primary diagnosis have been relatively
stable over the time period 2001-2016, the trend line for hospitalization rates for diabetes (any
diagnosis) has been leveling off.
Chronic Diseases: Cirrhosis
Data for cirrhosis mortality and morbidity appear in Appendices D216-D24 and are based on selected
County Health Assessment Indicators for 2014-2016 from the NYS Department of Health. Mortality and
Healthy People 2020 Objectives — Cirrhosis
SA-11 Reduce cirrhosis deaths.
Target: 8.2 deaths per 100,000 population

Broome County
58 Community Health Assessment 2019-2024
morbidity data sources have been previously described. The ICD-10 codes for cirrhosis mortality are K73
and K74.
In Broome County, there were, on average, 32 deaths per year attributable to cirrhosis of the liver. The
age-adjusted mortality rate for cirrhosis in Broome County was 13.4 per 100,000 population, which was
significantly higher than the 6.8 per 100,000 for NYS and the 8.1 per 100,000 for Upstate NY. Broome
County ranked in the fourth quartile for this indicator. In Broome County, cirrhosis of the liver accounted
for approximately 92 hospitalizations per year. The age-adjusted cirrhosis hospitalization rate in Broome
County was 4.6 per 10,000 population compared to 3.0 per 10,000 for NYS and 2.8 per 10,000 for
Upstate NY. Like other hospitalization rates, Broome County was lower than statewide rates though this
difference was not statistically significant. Between 2001 and 2016, the mortality and hospitalization
rates have been rising consistently. Broome County has not met the Healthy People 2020 target of 8.2
deaths per 100,000 population for this indicator.
Chronic Diseases: Asthma
Data for asthma mortality and morbidity appear in Appendices D240 and D249-D272. These data are
based on selected County Health Assessment Indicators for 2014 to 2016 from the NYS Department of
Health. Mortality and morbidity data sources have been previously described. The ICD-10 codes for
asthma mortality are J45 and J46.
In Broome County, an average of 4 deaths per year were due to asthma. The age-adjusted asthma
mortality rate for Broome County at 1.6 per million population was similar to NYS (1.3 per million) and
Upstate NY (0.9 per million), though the Broome County rate is unstable due to fewer than 20 events.
Although the mortality is low, the morbidity for this disease is relatively high. The number of
hospitalizations for asthma in Broome County was an estimated 217 per year. The age-adjusted asthma
hospitalization rate for Broome County was 5.4 per 10,000 population. The asthma hospitalization rate
for Broome County was significantly lower than NYS (11.4 per 10,000) but higher than Upstate NY (6.8
Healthy People 2020 Objectives — Asthma
RD-1 Reduce asthma deaths.
RD-1.1 Children and adults under age 35 (not applicable)
RD-1.2 Adults aged 35 to 64 years (6.0 per million)
RD-1.3 Adults aged 65 years and older (22.9 per million)
RD-2 Reduce hospitalizations for asthma.
RD-2.1 Children under age 5 years (18.1 per 10,000)
RD-2.2 Children and adults aged 5 to 64 years (8.6 per 10,000)
RD-2.3 Adults aged 65 years and older (20.3 per 10,000)
RD-3. Reduce hospital emergency department visits for asthma.
RD-3.1 Children under age 5 years (95.6 per 10,000)
RD-3.2 Children and adults aged 5 to 64 years (49.7 per 10,000)
RD-3.3 Adults aged 65 years and older (13.8 per 10,000)

Broome County
Community Health Assessment 2019-2024 59
per 10,000). Stratification of asthma hospitalizations by age group shows the highest morbidity for the
0–4 age group (9.7 per 10,000) and the 5-14 age group (7.2 per 10,000). Broome County ranked in the
third quartile for asthma hospitalizations overall as well as across most age groups. They were in the
fourth quartile for the asthma hospitalization rate for the 25-44 age group. Moreover, Broome County
met all of the age-specific Healthy People 2020 objectives for asthma hospitalizations. The asthma
hospitalization rate of 7.8 per 10,000 for the 0–17 age group also met the Prevention Agenda 2017 goal
of 17.3 per 10,000. Trend data from 2003–2016 shows a steady decrease in hospitalizations for asthma.
Based on NYS Prevention Agenda indicators, emergency room visits for asthma were 71.2 per 10,000 for
children age 0-4 which one-third the rate for NYS and well below the target of 205.7 per 10,000. In
addition, Broome County’s hospitalization rate for all asthma-related emergency department visits was
54.0 per 10,000 which was almost half the rate for NYS and 40% less than the 75.1 target for the NYS
Prevention Agenda.
Based on the BRFSS conducted by NYS in 2016, the age-adjusted prevalence of asthma in Broome
County was 12.2%, higher than the 9.6% for NYS and 10.4% for Upstate NY. In relation to asthma
prevalence, Broome County ranked in the third quartile. Like diabetes management, asthma
management has been a targeted focus for local community intervention and the success of these
efforts is evident in the lower asthma morbidity experienced by residents of Broome County relative to
the rest of the state.
Chronic Diseases: Chronic Obstructive Pulmonary Disease
COPD refers to a condition of chronic airway obstruction associated with permanent remodeling of the
airway as well as chronic symptoms and possible exacerbations. This condition includes the categories of
chronic bronchitis and emphysema. Although many individuals with COPD also experience asthma
symptoms, pure asthma is defined by its reversible nature. Thus, the ICD-9 codes for COPD included only
chronic bronchitis and emphysema. With the 10
th
revision of the ICD codes COPD was renamed to CLRD
and expanded to include other conditions of the lower respiratory tract such as asthma, status
asthmaticus, and tracheitis.
Mortality and morbidity data for chronic lower respiratory disease (CLRD, formerly COPD) appear in
Appendix D240-D248 and are based on selected County Health Assessment Indicators for 2014-2016
Healthy People 2020 Objectives — Chronic Obstructive Pulmonary Disease
RD-10 Reduce deaths from chronic obstructive pulmonary disease (COPD) among adults.
Target: 98.5 deaths per 100,000
RD-11 Reduce hospitalizations for chronic obstructive pulmonary disease (COPD).
Target: 50.1 hospitalization per 10,000
RD-12 Reduce emergency department (ED) visits for chronic obstructive pulmonary
disease (COPD).
Target: 57.3 visits per 10,000

Broome County
60 Community Health Assessment 2019-2024
from the NYS Department of Health. Mortality and morbidity data sources have been previously
described. The ICD-10 codes for CLRD mortality include J40 to J47.
CLRD accounted for, on average, about 1,177 deaths and approximately 566 hospitalizations per year in
Broome County. The age-adjusted mortality rate for CLRD in Broome County was 40.3 per 100,000
population, which was significantly higher than NYS (28.9 per 100,000) and Upstate NY (34.4 per
100,000). The age-adjusted hospitalization rate for CLRD in Broome County was 23.6 per 10,000, which
was lower than NYS (27.6 per 10,000) but not Upstate NY (23.4 per 10,000). Broome County ranked in
the second quartile for both CLRD mortality and hospitalization rate. For all three indicators (deaths,
hospitalizations, and emergency department visits), Broome County was well below the Healthy People
2020 objectives. Although the temporal patterns for mortality remained relatively stable from 2001 to
2016, the hospitalization rates for CLRD have increased from a low of 19.6 per 10,000 in 2005 to a high
of 23.6 in 2016. Thus, continued efforts for managing chronic lung disease in the community will be
needed to maintain this rate below the Healthy People 2020 objective.
Human Immunodeficiency Virus (HIV) & Acquired Immunodeficiency Syndrome
(AIDS)
The newly diagnosed HIV case rate (age-adjusted) for Broome County was 8.8 per 100,000 population,
which was higher than Upstate NY (7.0 per 100,000) and was half the NYS rate (16.0 per 100,000). The
AIDS case rate (age-adjusted) for Broome County was 4.8 per 100,000 population, which was lower than
NYS (7.7 per 100,000) but higher than Upstate NY (3.2 per 100,000). Broome County’s case rate was in
the fourth quartile for HIV and AIDS. Although the age-adjusted AIDS mortality rate was lower in
Broome County than in NYS (1.4 vs. 2.6 per 100,000), the age-adjusted rate was higher than the Upstate
area (0.9 per 100,000). The HIV case rate was approximately one-half of the target set by the Prevention
Agenda 2017 (14.7 per 100,000). The AIDS case rate was one-third the target set by the Healthy People
2020 objective of 16.1 new cases per 100,000. The trend chart for the AIDS case rate in Broome County
shows that the rate appears to have peaked in 2006 and has been stable ever since. It is uncertain
whether this represents normal variability due to small numbers or a reversal of the previous increase
between 2003 and 2016. (Appendices D1-D13)
Healthy People 2020 Objectives — HIV & AIDS
HIV-4 Reduce new AIDS cases among adolescents and adults.
Target: 12.4 new cases per 100,000 population
HIV-12 Reduce deaths from HIV infection.
Target: 3.3 deaths per 100,000 population

Broome County
Community Health Assessment 2019-2024 61
Optional Service Areas
Dental Health Services
The Oral Health Survey of third grade children covers the 3-year period from 2009–2011. Data from this
survey showed significant differences between Broome County and Upstate NY (Appendix D273-D279).
The percent of third grade children with dental caries experience was 56.7% for Broome County which
was significantly higher than the 45.4% for Upstate NY. And, the dental caries experience of third grade
children in Broome County exceeds the Healthy People 2020 target of 49.0% by an appreciable amount.
The proportion of third grade children with untreated dental caries was 42.3% for Broome County as
Healthy People 2020 Objectives — Dental Health
CH-1 Reduce the proportion of children and adolescents who have dental caries experience in
their primary or permanent teeth.
CH-1.1 Children age 3 to 5 years with dental caries experience in their primary teeth.
(30%)
CH-1.2 Children age 6 to 9 years with dental caries experience in their primary and
permanent teeth. (49.0%)
CH-1.3 Adolescents age 13 to 15 with dental caries experience in their permanent teeth.
(48.3%)
CH-2 Reduce the proportion of children and adolescents with untreated dental decay.
CH-2.1 Children age 3 to 5 with untreated dental decay in their primary teeth (21.4%)
CH-2.2 Children age 6 to 9 with untreated dental decay in their primary and permanent
teeth (25.9%)
CH-2.3 Adolescents age 13 to 15 with untreated dental decay in their permanent teeth
(15.3%)
CH-6 Increase the proportion of oral and pharyngeal cancers detected at the earliest stage.
Target: 35.8%
CH-8 Increase the proportion of low income children and adolescents who received any
preventive dental service during the past year.
Target: 33.2%
CH-12 Increase the proportion of children and adolescents who have received dental sealants on
their molar teeth.
CH-12.1 Children aged 3 to 5 years who have received dental sealants on one or more of
their primary molar teeth (1.5%)
CH-12.2 Children age 6 to 9 years who have received dental sealants on one or more of
their permanent first molar teeth (28.1%)
CH-12.3 Adolescents age 13 to 15 who have received dental sealants on one or more of
their permanent molar teeth (21.9%)

Broome County
62 Community Health Assessment 2019-2024
compared to 24.0% for Upstate NY, a statistically significant difference. Broome County ranked in the
third quartile for percent of third grade children with caries and in the fourth quartile for untreated
caries. The prevalence of untreated tooth decay in children in Broome County (42.3%) was considerably
higher than the Prevention Agenda 2017 target of 21.6% and the Healthy People 2020 Objective of
25.9%.
Although the oral health of children in Broome County is well below the rest of the state, the percent of
third grade children with dental sealants was significantly higher in Broome County (64.9%) than in
Upstate NY (41.9%). Insurance coverage for dental care was also significantly different with a higher
percentage of third grade children having dental insurance in Broome County than in the rest of the
state (88.5% vs. 81.8%). In relation to having at least one dental visit in the last year, Broome County
was significantly lower than Upstate NY (80.6% vs. 83.4%). Just over half of third grade children in
Broome County reported taking fluoride tablets on a regular basis, which was significantly higher than
the statewide average (41.9%).
Oral health data related to Medicaid clients in Appendix D273. Additional charts and graphsfor Medicaid
clients and for outpatient visits can be found in Appendices D280-D290. Among children ages 3 to 5
years, the emergency department visit rate specifically for dental caries was 100.6 per 10,000 children,
which was similar to NYS (90 per 10,000) and upstate NY (119.7 per 10,000). For this indicator, Broome
County ranked in the fourth quartile for the state. In addition, three-year averages for dental caries
emergency department visits among children age 3 to 5 years have increased steadily from 107.1 per
10,000 in 2006 to 182.0 per 10,000.
In the low income population, 33.2% of Medicaid enrollees in Broome County had at least one dental
visit within the last year; this figure was 47.6% for those between the age of 2 and 20. More than 25% of
Medicaid enrollees in Broome County had at least one preventive dental visit within the last year. For
these three indicators, Broome County was ranked in the first quartile and preventive care in particular
was above the Healthy People 2020 target of 25.4%. In 2016, the age-adjusted percentage of all adults
who had a dentist visit within the past year was 67.9% and was similar to Upstate NY. Broome County
ranked in the third quartile for this indicator.
As well, Broome County ranked in the third quartile for oral cancer with an age-adjusted incidence of
16.7 per 100,000 and an age-adjusted mortality of 2.5 per 100,000. These rates were similar to both NYS
and Upstate NY. In Broome County, the proportion of oral cancers diagnosed at an early stage was
33.3% for females and 31.6% for males, which nears the Healthy People 2020 target of 35.8%. While use
of dental care services were generally higher and showed improving trends, the dental health of
children and adults in Broome County was below statewide averages suggesting that expansion of, or
enhancements to, current public health efforts may be needed to reduce morbidities associated with
poor oral health.

Broome County
Community Health Assessment 2019-2024 63
Home Health Services
Under the Maternal Child Health and Development division, the Broome County Health Department
operates a Licensed Home Care Services Agency for Maternal Child Health. Under this program,
registered nurses provide home visits to growing families. Home visiting services include: a skilled
nursing assessment, provision of prenatal guidance and birthing information, assistance with obtaining
health insurance, and linking families to resources in the community such as prenatal care, family
planning, well-child exams, immunizations, breastfeeding, and child care. The nurses are trained to
recognize if a child or family has special needs and promote optimal physical, psychosocial and
developmental health and well-being for childbearing and child-rearing families. Thus, this program is
designed to help families receive the evaluation and treatment services they need.
Optional Other Service Areas / Programs
Medical Examiner
The county does not have a medical examiner. No information is submitted for this section.
Emergency Medical Services
The Emergency Medical Services (EMS) is a department within the county government. Information
about EMS can be found in Section 3B under “Access to Care.”
Laboratories
The Broome County Health Department does not operate a full-service laboratory, though limited
microscopy is performed as part of the clinic services. Therefore, no information is submitted for this
section.

Broome County
64 Community Health Assessment 2019-2024
B. Behavioral Risk Factors
The Leading Health Indicators, selected from the Healthy
People 2020 objectives, are used as measures of population
health reflecting the major health concerns in the United
States. These indicators are of public health importance
because of their ability to influence disease morbidity and
mortality. There are a total of 26 indicators that cover 12
topic areas which are listed in the box to the left. These
indicators depend to some extent on behavioral factors
and access to health care as well as environmental,
economic, and social conditions. As sexually transmitted
diseases, injury, and immunization have been previously
discussed, this section will address physical activity,
overweight and obesity, tobacco use, substance abuse, and
mental health. Access to Health Care is covered in Section
Three.
Data for this section are drawn primarily from the NYS
Expanded Behavioral Rick Factor Surveillance System
(BRFSS). This national survey is conducted annually statewide using probability sampling and random
digit dialing to permit calculation of point estimates. This telephone-based surveillance system is used to
monitor modifiable behaviors and other risk factors contributing to the leading causes of morbidity and
mortality in the adult population.
Leading Health Indicators
Access to Health Services
Clinical Preventive Services
Environmental Quality
Injury and Violence
Maternal, Infant and Child
Health
Mental Health
Nutrition, Physical Activity,
and Obesity
Oral Health
Tobacco Use
Reproductive and Sexual
Health
Social Determinants
Substance Abuse
Tobacco

Broome County
Community Health Assessment 2019-2024 65
Healthy People 2020 Objectives — Physical Activity
PA-1 Reduce the proportion of adults who engage in no leisure-time physical activity.
Target: 32.6%
PA-2 Increase the proportion of adults who meet current Federal physical activity guidelines for
aerobic physical activity and for muscle strengthening activity.
PA-2.1 Aerobic physical activity of at least moderate intensity for 150 minutes/week, or 75
minutes/week of vigorous intensity, or an equivalent combination (47.9%)
PA-2.2 Aerobic physical activity of at least moderate intensity for more than 300
minutes/week, or more than 150 minutes/week of vigorous intensity or an
equivalent combination (31.3%)
PA-2.3 Muscle-strengthening activities on 2 or more days of the week (24.1%)
PA-2.4 Aerobic physical activity and muscle strengthening activity (20.1%
PA-3 Increase the proportion of adolescents who meet current Federal physical activity guidelines
for aerobic physical activity and for muscle strengthening activity.
PA-3.1 Aerobic physical activity (20.2%)
PA-3.2 Muscle strengthening (developmental)
PA-3.3 Aerobic physical activity and muscle strengthening activity (developmental)
PA-4 Increase the proportion of the Nation’s public and private schools that require daily physical
education for all students.
PA-4.1 Elementary schools (4.2%)
PA-4.2 Middle and junior high schools (8.6%)
PA-4.3 High schools (2.3%
PA-5 Increase the proportion of adolescents who participate in daily school physical education.
Target: 36.6%
PA-6 Increase regularly scheduled elementary school recess
PA-7 Increase the proportion of school districts that require or recommend elementary recess for
an appropriate period of time.
PA-8 Increase the proportion of children and adolescents who do not exceed recommended limits
for screen time. [no more than 2 hours per day]
PA-8.1 Age 0-2, no television or videos on an average weekday (44.7%)
PA-8.2.1 Age 2-5 (83.2%)
PA-8.2.2 Age 6-14 (86.8%)
PA-8.2.3 Grades 9-12 (73.9%
PA-9 Increase the number of states with licensing regulations for physical activity in child care.
PA-10 Increase the proportion of public and private schools that provide access to physical spaces
and facilities outside of school hours for physical activity
PA-11 Increase the proportion of physician’s office visits that include counseling or education
related to physical activity
EH-2 Increase use of alternative modes of transportation for work. [Trips to work made by]
EH-2.1 Bicycling (0.6%)
EH-2.2 Walking (3.1%)
EH-2.3 Mass transit (5.5%)

Broome County
66 Community Health Assessment 2019-2024
Physical Activity
Data for physical activity comes from the 2013-2017 Expanded Behavioral Risk Factor Surveillance
System (BRFSS) for adults. These data are presented in Appendices E24-E31. The 2008 Physical Activity
Guidelines recommend moderately intense physical activity for at least 150 minutes per week,
vigorously intense physical activity for 75 minutes per week, or an equivalent combination distributed
throughout the week. Moderate intensity is exemplified by brisk walking, and means working hard
enough to raise heart rate and break a sweat, yet still being able to carry on a conversation. Vigorous
intensity is exemplified by jogging, and causes rapid breathing and a substantial increase in heart rate.
This recommendation applies to healthy adults aged 18-65 and is considered a minimum requirement
for maintaining health and reducing the risk of chronic disease. Additional health benefits can be gained
by increasing aerobic physical activity to 300 minutes per week of moderate intensity, or 150 minutes
per week of vigorous intensity, or equivalent combination. Importantly, adults should avoid inactivity
and perform muscle strengthening activities for all major muscle groups on 2 or more days per week.
In 2014-2016, 26.4% of Broome County adults reported no leisure-time physical activity which was
higher than NYS (23.7%). Stratified analyses indicate that women are almost twice as likely as men to
report no leisure time physical activity (22.7% for females vs. 13% for males). Individuals who are
between the ages of 35 and 44 are the most active age group with only 11.2% reporting no leisure-time
physical activity. Individuals over the age of 45 are twice as likely to have no leisure-time physical
activity. Between 22% and 25% of adults above age 45 report no leisure-time physical activity. In
addition, those with lower levels of both education and income are more likely to report no leisure-time
physical activity.
For older adults who cannot perform 150 minutes per week of moderate intensity physical activity due
to chronic health conditions, the Physical Activity Guidelines recommend that they be as physically
active as the extent of their capabilities permit. In addition, older adults should perform physical
activities to improve or maintain muscle strength and balance in order to reduce risk of falls.
For children and adolescents, the Physical Activity Guidelines recommend 60 minutes of physical activity
daily including moderate or vigorous intensity aerobic activity (3 days a week of vigorous intensity),
muscle strengthening (3 days per week), and bone strengthening (3 days per week).
Recent county-level data for physical activity among children and adolescents is lacking. The Youth Risk
Behavior Surveillance System (YRBSS) is a national school-based survey conducted by the Centers for
Disease Control and Prevention and administered to high school students. Similar to the BRFSS, this
survey is used to monitor health risk behaviors that contribute to the leading causes of death and
disability. Data from this survey are available at the state, local (major municipalities) and territorial
levels as well as for native populations, but are not available at the county level. (Appendices E30-E31)
In 2017, 23.2% of students in grades 9 through 12 in NYS reported being physically active for at least 60
minutes per day for 7 days per week indicating that three-fourths of all adolescents are not meeting the
current guidelines for physical activity. Nearly 42.4% reported being physically active for at least 60
minutes per day on less than 5 days per week and 15.0% of students were not physically active for 60
minutes on any day. Over 80% did not attend physical education classes five days per week, over 50%
did not play on a sports team, and over 40.8% watched television or used computers more than 3 hours

Broome County
Community Health Assessment 2019-2024 67
per day. A significantly larger proportion of females are not meeting current guidelines and they were
less likely than males to play on sports teams. Trends in three or more hours of television viewing
appear to be decreasing in NYS at a faster pace than the rest of the nation. Among WIC participants in
Broome County, a lower percentage of children had less than 2 hours of television viewing as compared
to NYS (83.9% vs. 85.0%).

Broome County
68 Community Health Assessment 2019-2024
Healthy People 2020 Objectives — Nutrition
NWS-1 Increase the number of states with nutrition standards for foods and beverages provided
to preschool-aged children in child care.
Target: 34 states
NWS-2 Increase the proportion of schools that offer nutritious foods and beverages outside of
school meals.
NWS-2.1 Schools that do not sell or offer calorically sweetened beverages to students
(21.3%)
NWS-2.2 School districts that require schools to make fruits or vegetables available
whenever other food is offered or sold (18.6%)
NWS-3 Increase the number of states that have state-level policies that incentivize food retail
outlets to provide foods that are encouraged by the Dietary Guidelines for Americans.
Target: 18 states
NWS-6 Increase the proportion of physician office visits that include counseling or education
related to nutrition or weight.
NWS-6.1 Adult patients with a diagnosis of cardiovascular disease, diabetes, or
hyperlipidemia (22.9%)
NWS-6.2 Adult patients who are obese (22.9%)
NWS-6.3 All children or adult patients (15.2%)
NWS-14 Increase the contribution of fruits to the diets of the population aged 2 years and older.
Target: 0.9 cup equivalent per 1,000 calories
NWS-15 Increase the variety and contribution of vegetables to the diets of the population aged 2
years and older.
NWS-15.1 Total vegetables (1.1 cup equivalent per 1,000 calories)
NWS-15.2 Green and orange vegetables and legumes (0.3 cup equivalent per 1,000
calories)
NWS-16 Increase the contribution of whole grains to the diets of the population aged 2 years and
older.
Target: 0.6 ounce equivalent per 1,000 calories
NWS-17 Reduce consumption of calories from solid fats and added sugars in the population aged 2
years and older.
NWS-17.1 Solid fats (16.7%)
NWS-17.2 Added sugars (10.8%)
NWS-17.2 Solid fats and added sugars (29.8%)
NWS-18 Reduce consumption of saturated fat in the population aged 2 years and older.
Target: 9.5%
NWS-19 Reduce consumption of sodium in the population aged 2 years and older.
Target: 2,300 mg

Broome County
Community Health Assessment 2019-2024 69
Diet & Nutrition
Data for diet and nutrition come from the NYS Expanded BRFSS (adults). There is evidence to suggest
that consumption of fresh fruits and vegetables not only provides important macro- and micro-nutrients
for good health, but also decreases the risk for certain types of cancers, cardiovascular disease, and
stroke as well as overweight and obesity.
The Dietary Guidelines for Americans 2010 recommend balancing calories to manage weight,
reducing/increasing specific foods and food components, and building healthy eating patterns. To
manage body weight, the guidelines recommend controlling caloric intake, particularly for people who
are overweight or obese, as well as increasing physical activity. In relation to specific foods to reduce,
the guidelines recommend decreasing daily sodium intake to less than 2,300 mg/day, consuming less
than 10% of calories from saturated fatty acids, consuming less than 300 mg/day of cholesterol,
reducing intake of calories from solid fats and added sugar, and limiting consumption of refined grains.
In relation to specific foods to increase, the guidelines recommend consuming more fruits and
vegetables especially dark green and red/orange ones, whole grains, and low- or fat-free fat dairy
products as well as eating a greater variety of protein sources including seafood, lean meats,
beans/peas, soy products, and nuts/seeds. Finally, attention to healthy eating patterns throughout the
day can ensure that all of the foods and beverages that are consumed fit the caloric and nutrient needs
of an individual over time.
The Expanded BRFSS data from 2013-2017 revealed only 31.9% of adults in NYS ate 1 or less servings of
fruits and vegetables per day. This value was similar to NYS in which only 31.5% of adults consumed 1 or
less servings of fruits and vegetables. (Appendices E32-E33)
Like physical activity, county-level data for nutrition among children and adolescents is currently lacking.
The Youth Risk Behavior Surveillance System (YRBSS) provides one of the few sources of data about
dietary intake for adolescents; however this survey is conducted only every two years with limited
information for specific localities. (Appendices E34-E36)
In 2017, 19.3% of students in grades 9 through 12 reported eating fruit or drinking 100% fruit juice 3 or
more times per day, 32% reported 2 or more, and 60.8% reported one or more than once a day. 7.3%
reported not eating fruit or fruit-drinks at all. 36.3% reported not drinking a can, bottle or glass of soda
or pop within the past week, 13.7% drank soda/pop at least once a day, 8.6% twice a day, and 4.9%
three times per day. Dietary consumption of fruits and vegetables as well as sugary drinks was similar
across age groups and grade levels. Trend data indicate that, for the US, the proportion of students who
report eating fruit or drinking 100% fruit juice less than three times per day has been decreasing since
2005 as compared to NYS which experienced its first decline in this indicator in 2009.

Broome County
70 Community Health Assessment 2019-2024
Overweight and Obesity
A healthy weight in adults is defined as a Body Mass Index (BMI) greater than or equal to 18.5 but less
than 25 kg/m
2
. Overweight is defined as a BMI greater than or equal to 25 but less than 30 kg/m
2
and
obesity is defined as a BMI greater than or equal to 30 kg/m
2
. BMI is calculated as weight (in kilograms)
divided by square height (in meters) and is used as a body weight standard and an indicator of the
degree of adiposity. This index is also used to provide an estimate of relative risk for disease such as
heart disease, diabetes, and hypertension. Information about obesity related indicators are located in
Appendix E38 and additional tables, charts, and maps appear in Appendices E39-E62 for both adults and
children.
In 2016, the prevalence of overweight among adults was 29.0% and the prevalence of obesity was
25.5%, yielding a combined total of 54.5%, with an increase over the period between 2004 and 2016.
Based on the 2013-2017 Expanded BRFSS survey data reported by the NYS Department of Health,
Broome County ranked in the second quartile in the state for obesity and in the third quartile for the
combined categories of overweight and obesity. The rate of obesity among adult residents of Broome
County exceeded the Prevention Agenda 2017 objective of 23.2%, but was below the target of 30.5% for
Healthy People 2020. In previous surveys, only 23.2% of adults reported receiving advice about their
weight by a health professional. While this figure is similar to the proportion who are obese, 64% of
individuals are overweight or obese, have increased risk based on weight status, and could be
considered potential candidates for counseling about weight. Of those who reported receiving advice
Healthy People 2020 Objectives — Overweight & Obesity
NWS-5 Increase the proportion of primary care physicians who regularly assess the body mass
index of their patients.
NWS-5.1 Adults (53.6%)
NWS-5.2 Children and adolescents (54.7%)
NWS-6 Increase the proportion of physician office visits that include counseling or education
related to nutrition or weight.
NWS-6.2 Adult patients who are obese (22.9%)
NWS-8 Increase the proportion of adults who are at a healthy weight.
Target: 33.9%
NWS-9 Reduce the proportion of adults who are obese.
Target: 30.5%
NWS-10 Reduce the proportion of children and adolescents who are considered obese.
NWS-10.1 Children aged 2 to 5 years (9.6%)
NWS-10.2 Children aged 6 to 11 years (15.7%)
NWS-10.3 Adolescents aged 12 to 19 years (16.1%)
NWS-10.4 Children and adolescents aged 2 to 19 years (14.5%)

Broome County
Community Health Assessment 2019-2024 71
about their weight, 87.7% were advised to lose weight. Thus, in the majority of cases when weight
status is addressed, clinicians seem to be providing clear advice to lose weight.
In children, BMI standards are based on growth chart percentiles with overweight defined as a BMI at or
above the 85
th
percentile but below the 95
th
percentile for BMI by age and gender, and obese as a BMI
at or above the 95
th
percentile for BMI by age and gender.
Until recently, the Youth Risk Behavior Surveillance System data was the only source of information
about weight status for adolescents. BMI and weight category were based on self-reported height and
weight. Biannual data was available at the state but not county level, and no data were available for
children in elementary school. Now, weight category data can be drawn from the NYS Student Weight
Status Category Reporting System (SWSCR). BMI data are collected for pre-kindergarten, kindergarten,
second and fourth grade students from elementary schools, for seventh grade from middle schools, and
for tenth grade from high schools. Data are reported in aggregate as weight status category and middle
and high school data are reported together. These data are available for 2015-2017, the last two years
of reporting with this new system.
Among elementary schools, the prevalence of overweight was 15.5% and the prevalence of obesity was
15.7% for a combined total of 31.3% for the category overweight or obese. For these indicators, Broome
County was similar to Upstate New York and ranked in the second quartile for obesity and in the third
quartile for the combined overweight/obese category. These data for obesity among elementary school
children indicate that Broome County meets the 15.7% target for the Healthy People 2020 among
children age 6 to 11 and the 16.7% objective for the NYS Prevention Agenda 2017.
Among middle/high schools, the prevalence of overweight was 18.3% and the prevalence of obesity was
20.7% for a combined total of 39.1% for the category overweight or obese. For these indicators, Broome
County was similar to Upstate New York and ranked in the third quartile for the state. These data for
obesity among middle/high school adolescents indicate that Broome County fell above the 16.1% target
for the Healthy People 2020 among children age 6 to 11 and the 16.7% objective for the NYS Prevention
Agenda 2017.
Because actual height and weight data are used to calculate BMI data reported to the state by schools
instead of self-report, these data may provide a more valid estimate of prevalence than self-report.
However, another important consideration is the opt out option parents may choose in relation to data
submission by NYS schools. Parents of children who are overweight or obese may be more likely to opt
out leading to estimates that are lower than the true prevalence of obesity and overweight among
school-age children. Although the YRBS includes data from high school students only, noticeable
differences can be seen in the weight status categories for SWSCR as compared to the self-report
measures from the YRBS for a similar time period. As might be expected, the data collected from the
SWSCR reveals a higher prevalence of overweight and obesity than the self-reported data from the
YRBS. The obesity epidemic, especially among youth, raises concerns about its health consequences
including the metabolic syndrome, diabetes, and associated short- and long-term complications.
Information about student weight status category by school district is presented in table format and
includes identification of each school district’s Need to Resource Capacity category as defined and
designated by the NYS Department of Education (Appendix E48). These data are also presented in
graphic format for both elementary schools (Appendix E49) and middle/high schools (Appendix E50).

Broome County
72 Community Health Assessment 2019-2024
Four out of the six school districts with the highest rates of obesity (above the 50
th
percentile) are also
categorized as high need to resource capacity.
For women participating in the WIC program, a significantly lower percentage of pregnant women were
overweight prior to pregnancy in Broome County as compared to NYS and Upstate NY (22.3% vs. 26.6%
and 26.4% respectively) and Broome County was in the second quartile for this indicator. However, an
appreciably higher percentage was obese prior to pregnancy for Broome County than for NYS and
Upstate NY (33.5% vs. 24.2% and 28.6% respectively) and Broome County ranked in the fourth quartile
for this indicator. (Appendices C44-C49) For Obesity among children aged 2-4 who participated in the
WIC program, Broome County ranked in the second quartile for the state (13.9%). This figure was not
significantly different than the state as a whole or the upstate area. Obesity among preschool age
children was below the Prevention Agenda 2017 goal of 16.7% for children and adolescents, but it is well
above the 9.6% target for obesity among children age 2 to 5 years old set by Healthy People 2020.
(Appendix E51)

Broome County
Community Health Assessment 2019-2024 73
Healthy People 2020 Objectives — Tobacco Use
TU-1 Reduce tobacco use by adults. [current smoker]
TU-1.1 Cigarettes (12%)
TU-1.2 Smokeless tobacco (0.3%)
TU-1.3 Cigars (0.2%)
TU-2 Reduce tobacco use by adolescents. [past month]
TU-2.1 All tobacco products (21%)
TU-2.2 Cigarettes (16%)
TU-2.3 Smokeless tobacco (6.9%)
TU-2.4 Cigars (8%)
TU-3 Reduce the initiation of tobacco use among children, adolescents, and young adults.
Adolescents age 12 to 17 years
TU-3.1 All tobacco products (5.7%)
TU-3.2 Cigarettes (4.2%)
TU-3.3 Smokeless tobacco (0.5%)
TU-3.4 Cigars (2.8%)
Young adults age 18 to 25 years
TU-3.5 All tobacco products (8.8%)
TU-3.6 Cigarettes (6.3%)
TU-3.7 Smokeless tobacco (0.2%)
TU-3.8 Cigars (4.1%)
TU-4 Increase smoking cessation attempts by adult smokers.
Target: 8%
TU-5 Increase recent smoking cessation success by adult smokers.
Target: 80%
TU-6 Increase smoking cessation during pregnancy.
Target: 30%
TU-7 Increase smoking cessation attempts by adolescent smokers.
Target: 64%
TU-9 Increase tobacco screening in health care settings.
TU-9.1 Office-based ambulatory care (68.6%)
TU-9.2 Hospital ambulatory care (66.2%)
TU-9.3 Dental care (developmental)
TU-9.4 Substance abuse (developmental)
TU-10 Increase tobacco cessation counseling in health care settings.
TU-10.1 Office-based ambulatory care (21.1%)
TU-10.2 Hospital ambulatory care (24.9%)
TU-10.3 Dental care (developmental)
TU-10.4 Substance abuse (developmental)
TU-11 Reduce the proportion of nonsmokers exposed to secondhand smoke.
TU-10.1 Age 3 to 11 (47%)
TU-10.2 Age 12 to 17 (41%)
TU-10.3 Age 18 and older (33.8%)

Broome County
74 Community Health Assessment 2019-2024
Tobacco Use
Data for smoking behaviors come from the BRFSS (adults), the YRBS (high school students), and the 2018
Prevention Needs Assessment Survey (grades 7-12). Information about tobacco use can be found in
Appendices E63 and E64-E75. Based on the 2016 NYS Expanded BRFSS, smoking prevalence among
adults in Broome County was 26.8% which was somewhat higher than NYS (29.9%) and slightly lower
than Upstate NY (38.8%). Broome County ranked in the fourth quartile for this indicator. This rate is
higher than the Healthy People 2020 objective of 12%. The percentage of adults living in homes where
smoking is prohibited was 79.3% for Broome County (second quartile) and not significantly different
than statewide.
Trend analysis for BRFSS data between 1995 and 2017 showed that prevalence peaked in 1998 at 24.1%
and that there was a steady decrease in prevalence from 23.2% in 2001 and to 15.5% in 2010.
Unfortunately, the prevalence of smoking appears to be increasing with a prevalence of 18.1% in 2012
and 21.2% in 2017.
For Broome County, Prenatal Care Assistance Program (PCAP)/Medicaid Obstetrical and Maternal
Services (MOMS) Program data related to smoking during pregnancy showed a prevalence (3-year
average) of 32% in 2007, 29% in 2008-2010, and 23.0% in 2017. Although three-year averages provide
more stable rates, these data are collected from new patients at the first prenatal visit and smoking
during pregnancy is often underreported. Thus, these data may not provide a true estimate. Smoking
during pregnancy and environmental exposure to tobacco smoke are associated with perinatal and
infant morbidity and mortality, including higher rates of pre-term labor, low birth weight, premature
rupture of membranes, abruption placentae, placenta previa, miscarriage, and fetal death. Pregnant
women should be counseled at the earliest point, preferably preconception, about the potential dangers
of smoking during pregnancy. Decreasing smoking during pregnancy may represent a leverage point for
reducing the county’s infant mortality.
Data for smoking behaviors among youth is available through the YRBSS though not at the county level.
In 2018 for NYS, 29.3% of high school students reported ever trying cigarette smoking even one or two
puffs. In addition, during the 30 days before the survey, 11.5% reported smoking cigarettes on at least
one day (past month), 3.5% reported smoking on 20 or more days (frequent smoker), and 3.7% reported
smoking more than 10 cigarettes per day (heavy smoker). Among the students who reported they were
currently smoking, 54.9% had not tried to quit in the past year. Over 7% of high school students
reported using chewing tobacco, snuff, or dip in the past month. Trend analysis indicates that although
the percentage of students who report ever trying cigarettes has decreased steadily between 1999 and
2018, the proportion of students who report smoking more than 10 cigarettes per day in the past month
(heavy use) has been increasing since 2006.
Local data was available from the 2006 and 2018 Prevention Needs Assessment county-specific reports
through the KYDS Coalition in Broome County. Data from the Prevention Needs Assessment Survey is
presented in Appendix E57 for cigarette use (past month) and Appendix E59 for heavy cigarette use.
With each higher grade, there is a monotonic increase in both cigarette use in the past month and heavy
cigarette use. In 2018, the proportion of students who reported smoking on at least one day during the
previous 30 days (past month) was 2.4% overall. The proportion of students who reported heavy

Broome County
Community Health Assessment 2019-2024 75
cigarette use was less than 1% for 7
th
and 8
th
grade students. For high school adolescents, the
prevalence of heavy use was 0.4% for 9
th
grade, 0.6% for 10
th
, 0.3% for 11
th
and 0.6% for 12
th
grade.
Although conclusions drawn from comparisons across different surveys should be interpreted
cautiously, there is some evidence to suggest that Broome County has lower prevalence of heavy
smoking among adolescents than NYS. For cigarette smoking in the past month, Broome County was
below the Healthy People 2020 target of 16% for cigarettes across all grade levels.
Substance Abuse
Based on data from the Statewide Planning and Research Cooperative System (SPARCS), between 2014-
2016 there were 219 alcohol-related motor vehicle injuries and deaths among adults equating to a rate
of 37.2 per 100,000, which is significantly higher than NYS (29.9 per 100,000) but similar to Upstate NY
Healthy People 2020 Objectives — Substance Abuse
SA-2 Increase the proportion of adolescents never using substances.
SA-2.1 Alcohol among adolescents age 12 to 17 (11%)
SA-2.2 Marijuana among adolescents age 12 to 17 (88.9%)
SA-2.3 Alcoholic beverages among high school seniors (30.5%)
SA-2.4 Illicit drugs among high school seniors (58.6%)
SA-3 Increase the proportion of adolescents who disapprove of substance abuse.
SA-3.1 Having one or two alcoholic drinks nearly every day among 8
th
graders (86.4%)
SA-3.2 Having one or two alcoholic drinks nearly every day among 10
th
graders (85.4%)
SA-3.3 Having one or two alcoholic drinks nearly every day among 12
th
graders (77.6%)
SA-4 Increase the proportion of adolescents who perceive great risk associated with substance
abuse.
SA-4.1 Consuming five or more alcoholic drinks at a single occasion once or twice a week
among adolescents age 12 to 17 (44%)
SA-13 Reduce past-month use of illicit substances.
SA-13.1 Use of any alcohol or any illicit drugs during the past 30 days among adolescents
age 12 to 17 (16.6%)
SA-13.2 Use of marijuana during the past 30 days among adolescents age 12 to 17 (6%)
SA-13.3 Use of any illicit drug during the past 30 days among adults age 18 years and older
(7.1%)
SA-14 Reduce the proportion of persons engaging in binge drinking of alcoholic beverages.
SA-14.1 Binge drinking (past 2 weeks) among high school seniors (22.7%)
SA-14.2 Binge drinking (past 2 weeks) among college students (37%)
SA-14.3 Binge drinking (past month) among adults age 18 and older (24.4%)
SA-14.4 Binge drinking among adolescents age 12 to 17 years (8.6%)

Broome County
76 Community Health Assessment 2019-2024
(39.6 per 100,000). For this indicator, Broome County ranked in the first quartile. For this same time
period, there were 46 discharges among neonates due to drug related causes equating to a rate of 29.8
per 10,000 newborn discharges. This rate was significantly higher for Broome County than for NYS
(10.1.0 per 10,000 newborn discharges) but not for Upstate NY. For this indicator Broome County
ranked in the fourth quartile. Broome County’s three-year age-adjusted estimate for drug-related
overdose hospitalizations was 94.0 per 10,000, which was significantly lower than both NYS (64.2 per
10,000) and Upstate NY (71.5 per 10,000). Trend data seem to show that for all three of these indicators
(alcohol-related motor vehicle injuries and deaths and newborn drug-related hospitalization rates, and
drug-related hospitalizations); Broome County rates appear to be increasing.
Data from the Expanded BRFSS for 2016 indicate that 20.1% of adults engaged in binge drinking (5 or
more drinks in a row) compared to 18.3% for NYS and 19.1% for Upstate NY. For binge drinking, Broome
County ranked in the third quartile. For this indicator, Broome County is not only ranked below the
county-level median with this health behavior, but is also below the Healthy People 2020 objective of
24.4% for binge drinking among adults. The prevalence of binge drinking is higher among males than
females with males being 2.2 times more likely to binge. Binge drinking among males is above the
Healthy People target. Prevalence is also higher among adults age 35-44 than among older adults (age
65+) and among those with lower educational attainment. Men in the younger age group are 5 times
more likely to binge than men 65 and older, and those with a high school diploma or less education are
2 times more likely to binge that men with a college degree. Trend data for binge drinking was relatively
stable from 2004 to 2012, but more recent data suggest this pattern is changing towards an increase.
Although Broome County is below the Healthy People 2020 target for binge drinking, continued
observation may be warranted given recent shifts in prevalence. (Appendices E76-E79)
Heavy drinking in the past month is defined as an adult male having more than two drinks per day or
adult female having more than one drink per day. Among adults in Broome County, 7.2% of adults
report heaving drinking in the past month. Like binge drinking, heavy drinking is higher among males in
the 35-44 age group. Trend data for heavy drinking follows a similar pattern to binge drinking with
stable rates until 2010 followed by an upward trajectory. Between 55% and 60% of adults in NYS have
had at least one drink in the past month without considerable variation in this indicator over time.
Data from the 2018 Prevention Needs Assessment Survey revealed that 10.4% of students engaged in
binge drinking and there was a monotonic increase in the percent of students who engaged in binge
drinking by grade level (Appendix E81). The percent binge drinking among 12–17 year-olds (7
th
through
12
th
grade) was higher than the Healthy People 2020 objective of 8.6%. In 2018, the percent of 12
th
graders who reported binge drinking was 23.7%, however comparisons to the Healthy People 2020
objective cannot be made as this objective refers to binge drinking in the past two weeks (versus past
month), which will inflate the proportion.
In 2018, 20.4% of 7
th
to 12
th
grade students reported using alcohol in the past month, 20.4% reported
using marijuana, 2.4% reported using cigarettes, 22.3% reporting using E-cigarette use, 3.3% reported
chewing tobacco use, 1.7% reported using amphetamines, 1.9% reported using sedatives, 1.9% reported
using other narcotics, and 3.6% reported using inhalants. Overall, 16.6% of students reported using any
drug, which is above the Healthy People 2020 target of 16.6 percent. There was a similar gradient by
grade level observed for lifetime use of alcohol, with 34.1% of all 7
th
to 12
th
grade students in Broome
County using alcohol at some time during their life. For lifetime use of any drug, 10.2% had smoked
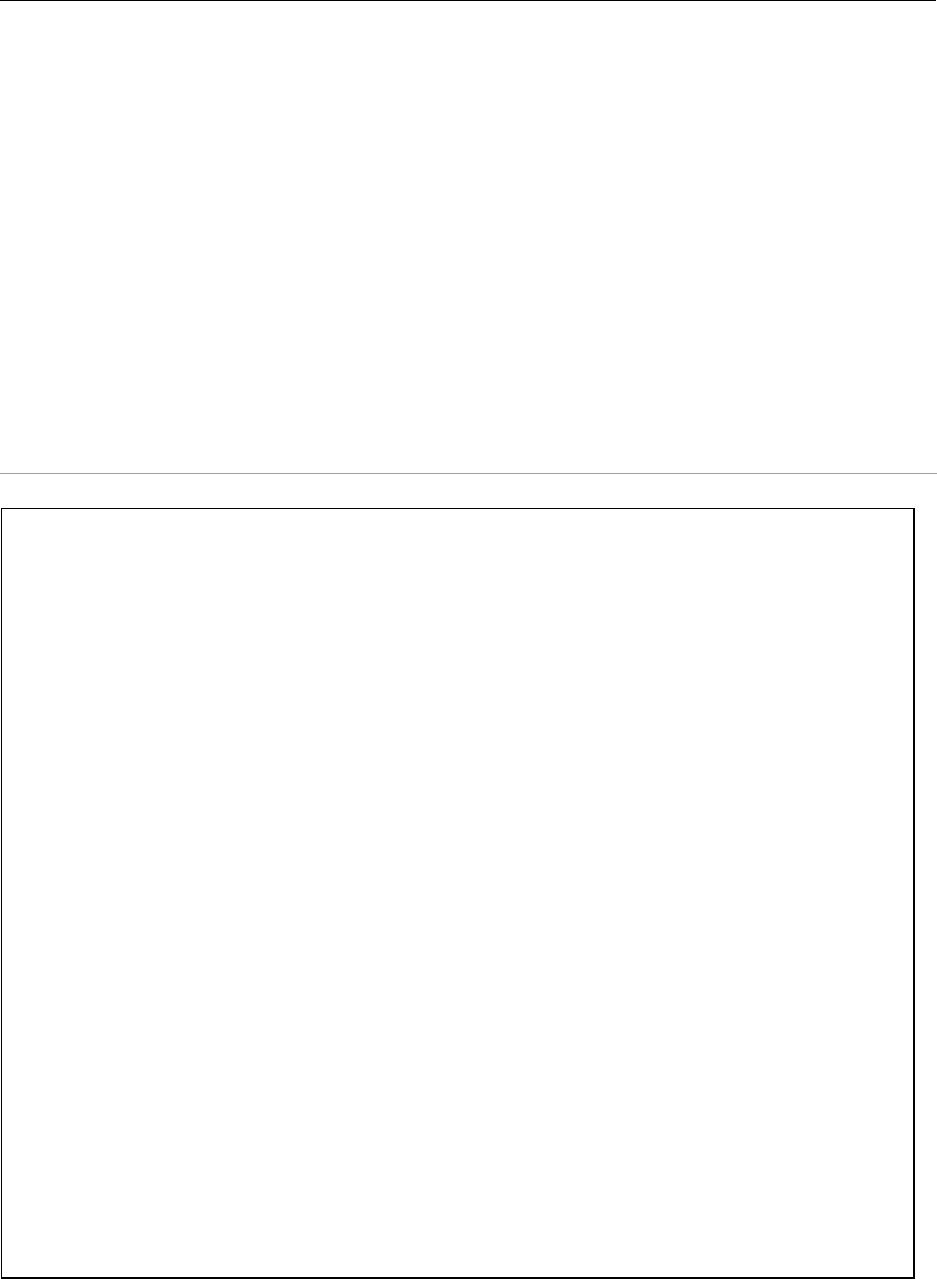
Broome County
Community Health Assessment 2019-2024 77
cigarettes, 26.5% had used E-cigarettes, 20.4% had used marijuana, 7.0% had used chewing tobacco,
1.9% had used inhalants, 1.7% had used amphetamines, 1.9% had used other narcotics, and 1.9% had
used sedatives. While comparisons to a similar survey conducted by Monitoring the Future indicate that
the rates are not significantly higher than those observed across the country, they are nonetheless
disturbing, particularly for parents. Marijuana use now equals or exceeds the prevalence of cigarette
smoking and is 3 times greater than the target objective for Healthy People 2020. (Appendix E80 for
alcohol use, Appendix E83 for marijuana use)
Data from the 2018 Prevention Needs Assessment also show that 72.3% of 7
th
through 12
th
grade
students think people risk harming themselves if they have five or more drinks of an alcoholic beverage
once or twice a week. This figure is higher than the Healthy People 2020 objective (SA-4.1 target 44%). In
addition, 71.1% of 8
th
graders, 60% of 10
th
graders, and 66% of 12
th
graders either strongly or somewhat
disapprove of having someone their age having one or two drinks of an alcoholic beverage nearly every
day. These figures are considerably lower than the Healthy People 2020 objective SA-3 (targets are
86.4%, 85.4%, and 77.6% respectively).
Healthy People 2020 Objectives — Mental Health
MHMD-1 Reduce the suicide rate.
Target: 10.2 suicides per 100,000 population
MHMD-4 Reduce the proportion of persons who experience major depressive episodes.
MHMD-4.1 Adolescents age 12-17 (7.4%)
MHMD-4.2 Adults age 18 and older (5.8%)
MHMD-5 Increase the proportion of primary care facilities that provide mental health treatment
onsite or by paid referral.
Target: 87%
MHMD-6 Increase the proportion of children with mental health problems who receive treatment.
Target: 75.8%
MHMD-9 Reduce the proportion of adults with mental health disorders who receive treatment.
MHMD-9.1 Serious mental illness (64.6%)
MHMD-9.2 Major depressive episodes (78.2%)
MHMD-10 Increase the proportion of persons with co-occurring substance abuse and mental
disorders who receive treatment for both disorders.
Target: 3.0%
MHMD-11 Increase depression screening by primary care providers.
MHMD-11.1 Adults age 19 and older (2.4%)
MHMD-11.2 Youth age 12-18 (2.3%)

Broome County
78 Community Health Assessment 2019-2024
Mental Health
Based on the 2016 Expanded BRFSS, 9.9% of Broome County adults reported 14 or more days with poor
mental health (Appendix E11-E15). This proportion was 10.7% for NYS and 11.2% for Upstate NY. Adults
in Broome County were 1.2 times more likely to report poor mental health for at least 2 weeks out of
the past month. Similarly, 11.4% of adults in Broome County reported that their physical health was not
good for 14 or more out of the past 30 days (Appendix E7). In 2016, over 30% of Broome County adults
reported having arthritis and more than half of those with arthritis were over 65 years of age. Almost
25% of adults reported having a disability (Appendix E17) and 68.8% of those with a disability were over
the age of 55. For all of these indicators, higher percentages were reported for those who were older (≥
age 55), less educated (high school education or less), and had incomes less than the Broome County
median individual income (<$25,000). Physical health and mental health share a dyadic relationship with
reciprocal interactions. Individuals with chronic conditions often experience depression, and those with
depression often have physical manifestations. It is interesting to note that as many adults reported
poor mental health as did poor physical health. Among children, data from the 2018 Prevention Needs
Assessment Survey indicated that 37.2% of adolescents (7
th
-12
th
grade) reported depressive symptoms.
Poverty, Crime, & Delinquency among Youth
Economic security means living in a household where there is enough money and resources to meet
basic needs. Children living in poverty experience food insecurity and compromised physical health
associated with poor nutrition. Extreme economic deprivation is the single most important risk factor
associated with problem behaviors in youth, substance abuse, violence, sexual acting out and teenage
pregnancy, delinquency, poor academic performance, and dropping out of school.
In 2018, 21.2% of children in Broome County ages birth to 17 years lived in poverty, a 3.2% decrease
from 2011, though lower to Upstate NY and NYS (19.9% and 15.7%). In addition, the percentage of
Broome County children receiving food stamps increased from 17.9% in 2005 to 27.7% in 2016. The
percentage of Broome County youth in families receiving public assistance also rose over this same time
period (from 7.2% to 8.4%), and is higher than for Upstate NY and NYS (6.3% and 4.1%). 3.5% of children
and youth in Broome County receive supplemental security income (SSI) as compared to 2.1% in the rest
of the state. Approximately 53% of Broome County children received free or reduced lunches in 2016,
compared with 47.5% in Upstate NY and NYS. In three of the five indicators of economic security
(poverty level, public assistance, and supplemental security income), Broome County has a higher
percentage of children in poverty than NYS. (Appendix E89)
Physical health and emotional health are interdependent, as evidenced by self-inflicted injuries, such as
suicide attempts. Between 2012-2014, 22 children age 15-19 had self-inflicted injuries that required
hospitalization (110.3 per 100,000 youth aged 15–19). The suicide mortality rate in 2012-2014 was
favorable. One suicide occurred among adolescents age 10-19 for the three-year period. (Appendix E90)
Still, the numbers of children who experience depression, anxiety, or bipolar disorder and the impact
these have on their emotional, cognitive, and academic abilities remains concerning.

Broome County
Community Health Assessment 2019-2024 79
Data for youth arrests and violent crime can be found in Appendix E91. Broome County youth aged 16 to
21 had a lower rate of arrests for driving while intoxicated (15.3 per 10,000) than NYS (17.5 per 10,000)
but lower than Upstate NY (25.2 per 10,000). In Broome County, this same age group also has a higher
rate of arrests for property crime (146.7 per 10, 000) than NYS (106.7 per 10,000) or Upstate NY (99 per
10,000). There were 57 intakes for juvenile delinquency among Broome County youth ages 7 to 15
years, which was less than half the number of intakes in 2005 (Appendix E92).
Results from the 2018 Prevention Needs Assessment Survey revealed a disturbing array of antisocial
behaviors in school (past year) among 7
th
through 12
th
graders (Appendix E84). In 2018, 8.7% reported
being drunk or high at school, 6.4% reported being attacked by another person with intent to harm,
8.4% of students were suspended from school, 4.5% reported gang involvement, 3.5% reported selling
illicit drugs, 2.3% reported having been arrested, 4.1% reported having carried a handgun, though only
1.0% reported carrying a handgun to school. Opportunities and rewards for pro-social involvement with
peers, school, family, and community act as protective factors. In contrast, poor family management,
family conflict, and exposure to adult antisocial behavior can contribute to delinquent behaviors.
National Data indicate that 1 in 10 children suffer from serious emotional disturbance, only 30% of them
graduate with a high school diploma and suicide is the third leading cause of death in 15-24 year olds.
According to the NYS Office of Mental Health, approximately 5% of NYS children have emotional
disturbances with intensive need for specialty services and 12% have at-risk behaviors with need for
early identification and intervention.
Depression in the Elderly
Along with children, elders are members of our community considered among the most vulnerable to
mental health problems and their consequences. Factors such as social isolation, cognitive changes,
financial stressors, and diminished physical capacity can exacerbate mental and emotional problems. In
the most serious situations, these conditions leave elders highly vulnerable to abuse and/or neglect.
Population studies among the elderly indicate a prevalence of depression ranging from 1% to 20%.
Consequences of depression include reduced life satisfaction and quality of life,
social deprivation and
loneliness, increased use of health and
home care services, cognitive decline and impairments in
activities
of daily living as well as suicide and non-suicide mortality.
Social Determinants of Health
County Health Indicators by Race/Ethnicity (CHIRE) for 2012-2016 were made available by the New York
State Department of Health (see Appendix B61). These indicators provide information about
racial/ethnic differences in socio-demographic, general health, birth- and injury-related indicators as
well as differences across multiple health conditions including respiratory diseases, heart disease and
stroke, diabetes, cancer, and substance abuse/mental health.

Broome County
80 Community Health Assessment 2019-2024
Based on census data, non-Hispanic Blacks/African Americans comprised 6.0% of the county population,
non-Hispanic Asian/Pacific Islanders comprised 4.8%, and Hispanics 4.1%. Income was lower and poverty
was higher among these minority populations. Median household income (2012-2016) was $2,680 for
non-Hispanic Blacks/African Americans, $39,837 for non-Hispanic Asian/Pacific Islanders, and $24,463
for Hispanics as compared to $50,20 for non-Hispanic Whites. The percent of families below poverty
(2012-2016) was 3.5 times higher for non-Hispanic Blacks/African Americans, 1.5 times higher for non-
Hispanic Asian/Pacific Islanders, and 3.5 times higher for Hispanics than for non-Hispanic Whites (32.7%,
13.8%, 32.6% respectively vs. 948%). These data indicate that minority populations in the county face
more difficult economic circumstances than Whites.
While total mortality rates were similar for non-Hispanic Blacks/African Americans and non-Hispanic
Whites, the percentage of premature deaths (< 75 years) for non-Hispanic Blacks/African Americans was
almost double that for non-Hispanic Whites (69.1% vs. 36.8%). The premature deaths among this
minority group contributed to more years of productive life lost (10,167 vs. 7,279 per 100,000). And
while the overall mortality rate for non-Hispanic Asian/Pacific Islanders was less than half that of non-
Hispanic Whites, the percentage of premature deaths among this minority group was higher than that of
non-Hispanic Whites (44.4% vs. 36.8%). For Hispanics, the total mortality was slightly lower than that for
non-Hispanic Whites, but the percent of premature deaths was larger (38.1% vs. 36.8%). Based on the
Indicators for Tracking Public Health Priorities (Appendix 167), the ratio of premature deaths (before age
65) was 2.5 for non-Hispanic Blacks and 2.3 for Hispanics as compared to non-Hispanic Whites. These
ratios were higher than NYS and higher than the 2018 NYS Prevention Agenda objective of 1.87 and 1.86
respectively.
Natality indicators showed similar disparities. The percent of births with early (1
st
trimester) prenatal
care and the percent of births with adequate prenatal care (Kotelchuk Index) was considerably lower for
non-Hispanic Blacks/African Americans than for non-Hispanic Whites (early prenatal care 61.5% vs.
76.8% and adequate prenatal care 69.7% vs. 82.2%). These differences in prenatal care may account for
the higher percentage of premature births and low birthweight births among non-Hispanic
Blacks/African Americans than among non-Hispanic Whites (premature births 12.1% vs. 7.9% and low
birthweight births 12.6% vs. 6.4%). Although the ratio of preterm births for non-Hispanic Blacks as
compared to non-Hispanic Whites in Broome County was lower than NYS (1.7 for Broome County vs. 1.6
for NYS), it was nonetheless slightly higher than the 2018 NYS Prevention Agenda objective (1.42 ratio).
The teen pregnancy rate among females aged 15-17 was 4.1 times higher for this minority group than
for non-Hispanic Whites (52.9 vs. 13.2 per 1,000). Among Hispanics, the teen pregnancy rate for females
aged 15-17 was 4.4 times higher than that for non-Hispanic Whites (58.8 vs. 13.2 per 1,000).
With respect to disease morbidity, the number of events among specific minority populations is often
less than 20, creating unstable rates even for three-year averages. Because of the small number of
cases, comparisons for non-Hispanic Asian/Pacific Islanders and for Hispanics cannot be made. For non-
Hispanic Blacks/African Americans, differences are evident in asthma hospitalizations. The age-adjusted
hospitalization rate (all ages) for non-Hispanic Blacks/African Americans was 2.2 times the rate for non-
Hispanic Whites (20.0 vs. 9.3 hospitalizations per 10,000). Moreover, the asthma hospitalization rate
among youth aged 0-17 years was 19.6 per 10,000 for non-Hispanic Blacks/African Americans compared
to 12.0 per 10,000 for non-Hispanic Whites.

Broome County
Community Health Assessment 2019-2024 81
Similar differences exist for diabetes. The age-adjusted hospitalization rate for diabetes as a primary
diagnosis was 35.3 per 10,000 for non-Hispanic Blacks/African Americans compared to 12.9 per 10,000
for non-Hispanic Whites. For hospitalizations in which diabetes was coded as a co-morbidity (any
diagnosis), non-Hispanic Blacks/African Americans experienced higher hospitalization rates than non-
Hispanic Whites (358.0 vs. 182.2 per 10,000). Further, the age-adjusted hospitalization rate for short-
term complications secondary to diabetes was likewise higher for non-Hispanic Blacks/African
Americans than for non-Hispanic Whites (19.9 vs. 5.4 per 10,000).
Economic disadvantage, poverty, and minority status can affect health and well-being. These social
determinants likely reflect disparities in mortality and morbidity within Broome County. Minority
populations experience a disproportionate share of early deaths, poor birth outcomes, and disease
burden due to asthma and diabetes.
C. The Local Healthcare Environment
The Physical Environment - Geography & Climate
Broome County includes the upper regions of the Appalachian Mountain Chain. Although the county is a
small metropolitan area, with a Rural Urban Continuum Code (RUCC) of 2, it is often referred to as rural
particularly at the upper and eastern edges. According to the 2019 Broome County Agricultural
Economic Development Plan, farmland accounts for 18% of the land mass within Broome County. The
number of farms in Broome County has continued to decline. The most recent statistics from the 2012
USDA Census of Agriculture indicated there were 563 farms covering 79,676 acres within the county.
These figures represent a 3% decrease in the number of farms and an 8% decrease in acreage since
2007.
The county has two large population centers, surrounding suburban areas, and, for the largest portion of
the land area, predominantly rural townships with small village centers. The roadways in these latter
areas lack sidewalks except in the small villages. Many, if not most, of the residential suburban areas
lack sidewalks as well. This deficit has made “walk-to-school” programs difficult. However, even in the
more populated areas where sidewalks are present, traffic and safety issues often prevent parents from
allowing their children to walk to school. Residents have also expressed concerns about sidewalk
maintenance, particularly in the winter, due to snow and ice. The risk of falling is of particular concern
among the elder population.
On the other hand, the community has made significant investment in a “Greenway” Project as well as
walking trails such as can be found in Otsiningo Park, the “Rail Trail” in Vestal, and a newly completed
trail in Whitney Point. The Greenway Project follows the natural contours of the area’s waterways and
provides opportunities for both walking and bicycling in addition to beautifying the community and
preserving green space. Most of these sites have the added benefit of being located in relatively flat
areas in contrast to the surrounding hills. Creating alternative indoor options for walking such as schools
that are readily accessible in rural areas was achieved through past innovative chronic disease
initiatives.

Broome County
82 Community Health Assessment 2019-2024
Travel distances make accessibility to health services located largely in urbanized areas more difficult
both for those who seek health care services as well as for those who deliver them such as home care,
hospice, and emergency medical services. The northern climate with its mixture of snow and ice deters
travel on roadways during winter and often late fall and early spring. Public transportation is available in
urbanized areas, but there are limited transit services outside these areas, most of which are “on-
demand.” BC Lift provides a transportation option for handicapped riders, though this service is also by
request. These services may be cost-prohibitive for the rural poor. Public transportation in rural areas
was rated as the second most important concern by emergency medical personnel. An intersection of
two major highways, I-81 and the recently developed I-86, previously Highway 17, brings economic
benefits as well as challenges such as traffic congestion and motor vehicle accidents.
Like many areas, residents express concern about air and water quality, industrial waste contamination
in soil and groundwater, as well as lack of inspection of private wells. The discovery of natural gas within
the Marcellus Shale formation and its potential extraction raised many environmental concerns. In 2014
however, high-volume hydraulic fracturing was banned and currently is not permitted in New York
State. Environmental issues remain a top priority with a desire for a “greener environment,” more eco-
friendly buses, and greater recycling. Most urbanized areas, excluding Johnson City, have municipal
water systems that are fluoridated; however, most residences in rural areas have private wells, so
access to and consistent use of fluoride supplements creates a challenge for dental care in this county.
Topography and location influence the climate of Broome County. Broome County is primarily pleasantly
cool with an average annual temperature of 45.8⁰ F and moist. This area has about 48% of the annual
average available sunshine, primarily in the summer months. The area has a reported 212 cloudy days
with 80% or greater overcast per year. Inclement weather is often cited as a barrier to being more
physically active. In relation to regional climate, the impacts of global warming continue to be a concern
with its potential for more severe weather events and devastating floods. Mitigation in response to the
severe flooding that occurred in 2005, 2006, and 2011 continues, and information about flooding as well
as response to other weather-related hazards by the county and its municipalities can be found in the
2019 Broome County Hazard Mitigation Plan.
Legal Aspects - Laws & Regulations
The Broome County Legislature is composed of 15 elected legislators representing county residents. The
Legislature is the policy-making body and taxing authority of Broome County Government. Through its
power is to legislate and approve appropriations, the County Legislature shapes the direction of Broome
County Government. The Broome County Charter defines the duties and powers of the Legislature. The
County Legislature is responsible for the adoption of all local legislation and levy of property taxes. The
county operates the county legal systems, handling the prosecution of crimes committed within the
county with sole authority over felony trials and shares authority with local courts in misdemeanor
cases. The county operates the sheriff’s office and probation services; provides social services, maintains
public records, is responsible for the delivery of public health, oversees the county landfill, maintains
and constructs county highways, and provides public transportation.

Broome County
Community Health Assessment 2019-2024 83
Social Aspects
Social isolation, particularly for rural elders, is a major issue. Census data from 2013-2017 reports 11,279
elders, 65 years of age and older live alone. A comparison between the 2009 Census data and 2017 in
the age range of and 65 above continue to increase. The lower end of this age spectrum reflects the
initial impact of the aging of the “Baby Boom.” Unfortunately, the core volunteers for senior centers and
vital services such as Meals on Wheels tend to be in their middle ages, which is a shrinking cohort in
Broome County. Another issue of concern is the potential increase in the need for in-home services
resulting from the predicted growth of the very old (85+ years) population.
In 2018-2019, the Broome County Office for Aging conducted nine focus groups and collected over 2,000
surveys. The data revealed that almost 28% of older adults reported feeling socially isolated, especially
those with incomes less than $19,999 and between the ages of 55-65 years. Previous surveys in Broome
County indicated that 19% of seniors living alone did not socialize with family, friends, or neighbors in
the past week and experienced decreased motivation to cook for self, which raises concerns about their
nutritional status. The outmigration of younger family members, often to seek employment in more
urban settings contributes to the social isolation of elders. Lack of social networks contributes to
isolation of elders, particularly among the oldest cohort and those living in poverty. Intergenerational
concerns related to elders include but are not limited to the issue of grandparents caring for
grandchildren and the stress on family caregivers for the elderly, particularly with chronic and
debilitating health issues.
Health Care and Economics
Diminishing funding from both private and public sources along with a rise in the number of
unemployed and uninsured/underinsured are placing an ever increasing strain on health care resources.
As cost control measures are being undertaken in the health care sector, more of the cost burden for
care is being shifted to the county level. A concern is the resulting strain on the portion of the system
that serves as a safety net within our county including The Dr. Garabed A. Fattal Community Free Clinic
(Community Free Clinic). Many governmental agencies and offices are functioning with tight budgets.
Although Broome County has been successful in running many health promotion and education
programs that are grant funded, both public and private foundation grant funding has been curtailed
and successful programs may be less sustainable without these types of funding. Efforts to ensure
sustainability of existing services have focused on expanding and diversifying funding sources.
Institutions - Schools
There are 12 public school systems serving K-12 in Broome County in addition to Catholic and other
religious related systems. These school systems serve parts of four counties in addition to Broome. The
Board of Cooperative Educational Services (BOCES) serves 15 school districts in Broome and Tioga

Broome County
84 Community Health Assessment 2019-2024
counties. Post-secondary education is offered in colleges and technical schools located in Broome
County including: Binghamton University, State University of New York at Binghamton, Broome
Community College, Davis College, and Ridley-Lowell Business and Technical Institute. Fourteen colleges
and universities are located within a one-hour drive of Binghamton.
Care and education of very young children is an important part of the community. Because childcare is
provided in both formal and informal settings, the ability to accurately determine service providers and
service usage is limited. Preschools in NYS provide early childhood education, laying a solid foundation
for future growth and learning. NYS is involved in an ongoing effort to have preschools approved by the
Department of Education. According to the NYS Education Department (NYSED) State Education
Department Reference File (SEDREF) database, there are 37 preschool programs operating in Broome
County, however only six of these programs are on the approved list of special education programs
pursuant to section 4410 of the NYS Education Law.
Agriculture
Agricultural issues continue to have ramifications for the health of citizens of Broome County. Dairy and
fruit and vegetable farming remain the mainstays of the local agricultural picture. Farm workers have
distinct risks for health issues as well as access to health care services. Rural dwellers, particularly
farmers often define health as the ability to work, delaying health care until unable to work. This cultural
aspect of how health is defined is compounded by the preference for use of informal networks, the
nature of self-employment, which limits access to health insurance, and the hands-on nature of farming
which leads many agricultural workers to seek health care only when they can no longer ignore the
problem. This delay may result in an emergent situation, raising the cost of treatment. One advantage of
a strong agricultural system within the region is the ability to accentuate the use of locally
grown/produced foods. The Cornell Cooperative Extension (CCE) along with may regional partners
including the Rural Health Network of South Central New York (RHNSCNY) are focusing on bringing
locally grown/produced foods to public institutions within the county. Growing Health, a food tasting
symposium has served to help raise awareness about the advantages of using locally grown foods. Food
safety is of concern throughout the country with many recent examples of food contamination.
Moreover, in an era of mass production and distribution of food supplies, the source is often difficult to
discern. Food safety concerns may encourage the use of locally grown/produced foods.
Media Messages
Broome County has four local television stations serving the area. Cable television services also include a
regional news channel, with one focus area being the Southern Tier of New York. In addition, the area
has multiple radio stations. The Press and Sun Bulletin is the local daily newspaper and provides an
electronic site entitled pressconnects.com. Each of these media outlets is a source for health
information and public service announcements (PSAs). These PSAs have provided support for several
programs including Sodium Reduction in Communities, Steps to a HealthierNY, BC Walks, and the Rock

Broome County
Community Health Assessment 2019-2024 85
on Cafe. Use of social marketing and media for health messages are a means of effecting changes in diet,
physical activity, and tobacco use making healthy choices normative and creating a healthy lifestyle
culture.
Laws and Regulations
New York State has been highly successful in promoting tobacco free environments through laws and
regulations regarding tobacco use in public areas, use of taxes to deter tobacco consumption, and focus
on enforcement of regulations on tobacco sales to minors. The most recent success was demonstrated
through the amendment to the Adolescent Tobacco Use Prevention Act (ATUPA), in effect as of
November 13, 2019, which has raised the minimum age of sale from 18 to 21 for tobacco products,
including electronic cigarettes. The greatly reduced access of these products to minors will ideally
prevent a generation from acquiring costly and potentially deadly addictions. For almost two decades,
tobacco-free workplace regulations have been in place and have become more stringent, now covering
entrances to public institutions such as hospitals and libraries prohibiting individuals from congregating
just outside doorways to smoke. Smoking is prohibited at New York Playgrounds between sunrise and
sunset if anyone under the age of twelve is present. Many recent amendments to these laws have
included electronic cigarettes otherwise known as vaping into their jurisdiction as well. In 2017,
Binghamton University was also recognized as a Tobacco Free Campus, as part of a Tobacco Free
initiative.
Environmental Management
Broome County enjoys the active participation of its citizens in shaping environmental policy through
the Broome County Environmental Management Council (EMC). Initially established by the Broome
County Legislature, the EMC seeks to preserve, protect, and enhance the local environment. Its
members include members of the community with environmental concerns who serve as Broome
County’s government citizen advisory board on environmental matters. Since 1971, volunteer members
of the EMC have conducted meetings and public information sessions in addition to preparing reports,
plans, and advisory resolutions. Topics of concern to the EMC include natural resource management,
water resource protection, land use planning, and sustainable development as well as hazardous and
solid waste management.

Broome County
86 Community Health Assessment 2019-2024
Section Two — Local Health Unit Capacity
Profile
Introduction
Public health responsibilities encompass preventing epidemics and the spread of disease, protecting
against environmental hazards, preventing injuries, encouraging healthy behavior, helping communities
to recover from disasters, and ensuring the quality and accessibility of health services.
Public health employees are dedicated to providing safe environments and services to help the people
who are most at risk to thrive. While the core functions of public health are health assessment, policy
development as it relates to matters pertaining to health, and assurance of a healthy environment
through surveillance, the end result of these functions is to improve the health of our residents and
communities. Private and public organizations, individuals, government officials and public health
employees work together to accomplish this mission.
The focus of health programming in our community is determined by the needs of the population and is
data driven and evidence based. Public health employees monitor the health status of the community
through surveillance of local information regarding disease states and environmental hazards.
Additionally, employees review data collected by the New York State Department of Health and the
needs assessments of various community agencies to compile a Broome County Community Health
Assessment. Health related issues are diagnosed and investigated with the intent to inform, educate,
and empower the community, thereby giving residents the voice and responsibility for action. In support
of community efforts, the Health Department then develops policies and plans in response to the
identified areas of action.
Public health response also includes enforcement of laws and regulations that protect health. Food
service inspections, along with compliance checks for retail tobacco outlets are two examples of how
public health employees monitor areas of concern to protect the health and safety of community
members.
Working with at-risk populations, those who are uninsured or underinsured, the Health Department
links people to necessary services and assures the availability of healthcare options.
Operational planning is an important part of public health. To assure a competent public health
workforce, the Health Department will continue to work with institutions of higher education to train
and develop expertise in employees, ensuring that they meet or exceed established standards.
The department will continue to evaluate effectiveness, accessibility and the quality of both personnel
and population-based health programming, and will use data to research innovative, community
focused solutions to health problems.
Broome County Health Department
Mission: The Broome County Health Department is committed to working proactively in
collaboration with the community to preserve, promote and protect the public health and quality
of life of all Broome County Residents.
Vision: Leading the community to the promise of a healthy future

Broome County
Community Health Assessment 2019-2024 87
The Broome County Health Department has adopted ten essential public health services that are integral
to assuring the health of the community (see also Appendix F2).
Organization
The Broome County Health Department is a full-service health department. In addition to state-
mandated core basic services, a range of preventive and population-based services is provided to ensure
public health and wellness. The ability of the health department to provide preventive services and
chronic disease support and education (e.g., breast cancer screening) strengthens the existing health
care delivery system with the goal of taking a proactive role in helping to improve the overall health
status of community residents. Divisions within the Broome County Health Department include Clinic
Services, Administration, Environmental Health Services, Health Promotion and Disease Prevention,
Children with Special Health Care Needs, Maternal Child Health and Development. The Fiscal Services
Unit and Health Promotion and Outreach (grants) are part of the Administration Division (refer to
Organizational Chart in Appendix F1).
Local health departments in New York State are required by NYS Public Health Law to conduct
Community Health Assessments as part of the application to obtain state aid for local public health
services. Priorities and recommendations identified in the Community Health Assessment are the basis
for measuring and evaluating the array and quality of local public health services provided to county
residents. Health Department administration is responsible for this important activity. A complete
description of the process used to conduct the community health assessment can be found in Section 3
d. of this report.
Broome County Health Department is committed to heightening public awareness of preventable health
conditions through community health education and promotion. Lifestyle choices and personal health
habits are important factors in the prevention of disease.
The Ten Essential Public Health Services
1. Monitor health status to identify community health problems.
2. Diagnose and investigate health problems and health hazards in the community.
3. Inform, educate, and empower people about health issues.
4. Mobilize community partnerships to identify and solve health problems.
5. Develop policies and plans that support individual and community health efforts.
6. Enforce laws and regulations that protect health and ensure safety.
7. Link people to needed personal health services and assure the provision of health care when
otherwise unavailable.
8. Assure a competent public health and personal healthcare workforce.
9. Evaluate effectiveness, accessibility, and quality of personal and population-based health services.
10. Research for new insights and innovative solutions to health problems.

Broome County
88 Community Health Assessment 2019-2024
Several programs are designed to assist and motivate individuals to voluntarily practice and sustain
positive changes in their health-related behaviors are available. Staff specializing in health education and
disease prevention within various Health Department Divisions described below is available to provide
educational materials and presentations to the public on a variety of topics. The programs listed within
each Division provide an array of health education and promotion activities throughout Broome County.
Many programs offer health education and promotion throughout multiple counties.
County taxes help support health department services. Although some services are free to Broome
County residents, most services have a fee based on cost, with fees adjusted on ability to pay. Medicaid,
Medicare, and private insurance may be used to pay for care. Fees are also charged for most
Environmental Health Division services.
Staffing & Skill Level
The health department is headed by a Public Health Director and staffed with 60 full time-equivalent
(FTEs) employees. The health department employs a part-time Medical Director and a Health Advisory
Board provides administrative consultation. The Public Health Director is responsible for initiating and
managing the local public health programs and has the general powers and duties specified in Section
352 of the NYS Public Health Law. The Director is responsible for maintaining a high standard of public
health services in accordance with the general policies and objectives of the County Executive and
County Legislature and with applicable State and local health laws and ordinances. General supervision
is exercised over the environmental health, sanitation, medical and public and/or community health
nursing services.
There are six division directors: Environmental Health Division Director, Director of Clinic Services, WIC
Nutrition Services Director, Director of Children with Special Health Care Needs, Director of Maternal
Child Health and Fiscal Services Administrator. In addition, there are Supervising Public Health
Educators, Supervising Public Health Nurses, part-time physicians (practicing in the sexually transmitted
disease clinic, chest clinic, and employee health), full-time and part-time Nurse Practitioners, Registered
Professional Nurses in a variety of roles, Public Health Engineers, Senior Public Health Sanitarians
Groundwater Management Specialists, and a Public Health Preparedness Coordinator. Descriptions of
the administration and divisions are detailed in the sections that follow.
Expertise & Technical Capacity
The Director is responsible for the conduct of the Community Health Assessment. The Health
Department has the privilege of having tenured staff member, Yvonne Johnston, DrPH, MPH, MS, RN,
FNP, also an Associate Professor and the Founding Director Master of Public Health Program
Binghamton University, direct and author the last two Broome Community Health Assessments. In
addition to her above-mentioned roles, this individual has served as the local evaluator for multiple
NYSDOH and CDC grant projects led by the Health Department. Many of these local program evaluation
analyses provided input to the document and informed the decision-making process.
A variety of data sources were used to conduct this assessment in addition to the use of pencil-and-
paper surveys, online surveys using Survey Monkey, and focus groups. Access to online data has
improved the ability to obtain relevant and meaningful local statistics, many of which are available

Broome County
Community Health Assessment 2019-2024 89
through the NYS Department of Health website including the NYSDOH Prevention Agenda Dashboard,
Community Health Assessment Indicators, Community Health Data Set, Delivery System Reform
Incentive Program (Care Compass Network), which are publicly available, as well as SPARCS data and
other sources available through the Regional Health Information Organization; HealtheConnections and
the Health Commerce System.
Expansion of data that is geocoded and which can be mapped provides rich information for public health
assessment and planning. In addition, the county provides Geographic Information System and Mapping
Services through an online portal, and this service was used for developing some of the maps in this
document. The conduct of the Community Health Assessment and the preparation of this document is a
daunting task and requires a considerable amount of human resources. This process, however, is
invaluable in relation to development of collaborative efforts with local hospital systems. Fortunately,
the Southern Tier Population Health Improvement Program (PHIP); through HealtheConnections,
provided tremendous support and financial resources. The Health Department was able to hire and train
several part-time, temporary public health representatives to assist with gathering and updating data
and writing sections of the 2019-2024 CHA/CHIP. Continued efforts to build the capacity of local health
departments to conduct comprehensive, meaningful and user-friendly Community Health Assessments
are still necessary. Constrained by its budget, increasing service demands, and need to respond to
emerging public health threats, the local health department look to the state for direction and support
of these efforts.
Adequacy & Deployment of Resources
Administration
Administrative services include: coordination of community health assessment; public health planning;
annual reports; preparation and analysis of complex financial and statistical reports; provision of
information and guidance in fiscal matters; coordination of departmental budget process; payroll and
personnel processing; accounts payables/receivables; cash management; statistical and financial
analysis; billing; claiming; grants management; representing the department to the public; general
distribution of communications and written materials from Administration and the outside community
to the department; and preparing departmental staff and the community to respond to public health
emergencies. Health Department staff regularly participates in emergency preparedness drills/exercises
designed to test response protocols and procedures. Staff routinely provides presentations to
Administration
Mission: Administration exists to establish and maintain the necessary infrastructure to assure the
quality and consistency of public health services provided to the community in a cost-effective
manner. The department strives to reduce inefficiencies, provide economies, and ensure
compliance with regulations, accreditation standards and laws established by governing bodies.
Administration serves as a “hub” between external recipients and internal recipients of services.

Broome County
90 Community Health Assessment 2019-2024
community groups on emergency preparedness and emerging public health topics. The Emergency
Preparedness Program, explained at the end of this Administration Division section, also oversees the
development of the Broome County Medical Reserve Corps—a cadre of medical and non-medical
professionals that have volunteered to provide various services during emergencies and disasters. In
addition, the contracted services of the Public Health Medical Director are based in Administration.
Description of Services
The Administration Division is composed of three units: Fiscal, Departmental Support, and Administration.
➢ Fiscal is responsible for all facets of the Health Department’s finances. Under the direction of the
Fiscal Services Administrator, the fiscal staff provide payroll and personnel processing, accounts
payable and receivables, cash management, statistical and financial analysis, billing, claiming and
grants management. In addition, the unit prepares complex financial and statistical reports
including cost reports, state aid applications, and various reports for Health Department
programs. Staff provides information and guidance on fiscal matters to the other divisions. Fiscal
staff act as liaisons to agency and non-agency staff regarding fiscal and program operations,
departmental budget requests, and grant programs. The Fiscal Services Administrator coordinates
the budget process, fiscal procedures, and personnel activities for the entire Health Department.
➢ Administration:
○ Plans, directs, and administers all public health programs and services according to
applicable laws and regulations as described in the Broome County Charter, Public Health
Law and federal regulations.
○ Serves as a primary and expert resource for establishing and maintaining public health
policies, practices and capacity.
○ Conducts public health surveillance, investigates public health issues, and evaluates
public health interventions targeting chronic disease prevention and control, emerging
infectious disease outbreaks, toxic exposures, environmental health problems, injuries,
unintentional child fatalities, injuries or deaths due to motor vehicle, pedestrian and
bicycle crashes, communicable diseases, maternal child health morbidity, and tobacco
control and preventive cancer services.
○ Directs the 2019-2024 Community Health Assessment and Community Health
Improvement Plan process and functions as a community liaison in the process.
○ Provides direct supervision and direction of departmental community health education
and promotion activities. Coordinates and administers health education and health
promotion activities in collaboration with other community agencies, stakeholders,
residents and elected officials.
○ Provides direct supervision and direction to the fiscal and departmental support staff.
➢ Administration:
Public Health Standards:
Investigate health problems and environmental public health hazards to protect the community
➢ Conduct timely investigations of health problems and environmental public health hazards.
➢ Contain/mitigate health problems and environmental public health hazards.
➢ Analyze public health data to identify trends in health problems, environmental public health
hazards, and social and economic factors that affect the public’s health.

Broome County
Community Health Assessment 2019-2024 91
➢ Maintain a plan with policies and procedures for urgent and non-urgent communications.
➢ Inform and educate about public health issues and functions.
➢ Provide health education and health promotion policies, programs, processes, and interventions
to support prevention and wellness.
➢ Provide information on public health issues and public health functions through multiple methods
to a variety of audiences.
➢ Develop public health policies and plans.
➢ Serve as a primary and expert resource for establishing and maintaining public health policies,
practices, and capacity.
➢ Conduct a comprehensive planning process resulting in a Community Health Improvement Plan.
➢ Maintain a Public Health Emergency Preparedness and Response Plan for all threats and hazards.
➢ Enforce public health laws.
➢ Review existing laws and work with governing entities and elected/appointed officials to update
as needed.
➢ Educate individuals and organizations on the meaning, purpose, compliance, and benefit of public
health laws and how to comply.
➢ Conduct and monitor public health enforcement activities and coordinate notification of
violations among appropriate agencies.
➢ Evaluate and continuously improve processes, programs and interventions.
➢ Use a performance management system to improve organizational practice, processes, programs,
and interventions.
➢ Develop and implement quality improvement processes integrated into organizational practice,
programs, processes and interventions.
➢ Maintain administrative and management capacity.
➢ Develop and maintain an operational infrastructure to support the performance of public health
functions.
➢ Establish effective financial management systems.
➢ Maintain capacity to engage the public health governing entity.
➢ Maintain current operational definitions and statements of the public health roles,
responsibilities, and authorities.
➢ Provide information to the governing entity regarding public health and the official responsibilities
of the health department and of the governing entity.
➢ Encourage the governing entity’s engagement in the public health department’s overall
obligations and responsibilities.
2020 Administration Objectives
➢ Engage in meaningful research of community health status, measured by jurisdictional
mortality, incidence, or prevalence. Assess county characteristics such as poverty, health
disparities, and health literacy to determine health behaviors, adverse health events, and
populations at risk.
➢ Coordinate stakeholders from all sectors to participate in the Community Health Improvement
Plan.

Broome County
92 Community Health Assessment 2019-2024
➢ Develop a well-trained and competent workforce through assessing training needs and
collaborative planning with institutions of higher learning to maintain the technological tools of
the public health infrastructure that are necessary to support all essential public health services.
➢ Increase awareness of chronic disease prevention through evidence-based health promotion
and education activities and strategies that encourage lifestyle changes and engages community
members where they live, learn, work, play, and pray.
➢ Build the capacity of community organizations to provide health information and programming
as part of “doing business” offering cost-effective programs that impact health outcomes and
are easy to replicate.
➢ Collaborate with institutions of higher learning to bring in expertise in planning and evaluation,
epidemiologic studies, data collection, and management.
➢ Continue to support and coordinate and develop the Broome Opioid Abuse Council (BOAC)
along with strengthening the planning capacity of the county to reduce the social and health
harms related to the misuse of opioid drugs. The multidisciplinary council, led by the Broome
County Opioid Overdose Coordinator seeks to improve the county’s response to the growing
opioid abuse crisis facing residents and to reduce the incidence and prevalence of opioid
addiction and death. Goals have been established within the structure of subcommittees
intending to: educate the public about addiction and available services; facilitate the
development of appropriate treatment and prevention services; and strengthen the capacity of
law enforcement and the courts to protect the community.
➢ The Public Health Emergency Preparedness Program will utilize grant funding to enhance
infrastructure for responding to emerging infectious diseases such as Ebola and the Zika Virus
which may affect the health and safety of Broome County residents. This may include meeting
with hospital personnel, convening drills, practicing donning and doffing of personal protective
equipment, and communication exercises with EMS, hospital CMOs, and the County Executive
Office.
2020 Administration Program Highlights
➢ Continue to maintain emphasis on reducing the opioid crisis with the direction of the Broome
County Opioid Prevention Coordinator and Overdose Data to Action Grant to help build and
support the county response infrastructure.
➢ Maintain health education activities to provide for coordination of efforts to prevent diseases and
encourage healthy lifestyles by building the capacity of community organizations and by seeking
insurance reimbursement where appropriate.
➢ Improved community health assessment and surveillance activities through coordination with
other community agencies.
➢ Continued maximization of grant funding to support operating budget as the focus of public
health shifts from direct services provision to surveillance, assurance, and policy development.
➢ Prioritization of expenses to reflect identified staff needs for education and technology, while
focusing on equitable salary levels for recruiting and retaining staff.
Public Health Emergency Preparedness/ Medical Reserve Corps
The Broome County Health Department, under the direction of both state and federal governments, is
responsible for emergency response plans and active response to any type of emergency affecting the

Broome County
Community Health Assessment 2019-2024 93
public health including: natural events (i.e., floods, ice storms) and deliberate malicious acts (terrorism).
Additionally, the Emergency Preparedness Program provides training and exercises to test and train
public health response staff. The Program also oversees the Medical Reserve Corps (MRC) which consists
of medical professionals and non-medical volunteers who donate their time and expertise to prepare for
and respond to emergencies of any kind. The MRC also engages in chronic disease initiatives and
programs offered by the Health Department.
The Broome County Public Health Emergency Preparedness and Response Plan is developed by the
Public Health Emergency Management Program within the Broome County Health Department. The
Plan is an annex of the Broome County Comprehensive Emergency Management Plan Emergency
Support Function #8 – Public Health and Medical Services.
The Plan utilizes an all-hazards approach to planning and is based upon standards and guidance
provided by the New York State Department of Health, the Centers for Disease Control and Prevention,
the National Association of County and City Health Officials Project Public Health Ready, and the Public
Health Accreditation Board.
While Broome County’s Emergency Support Function - Public Health and Medical Services establishes
the strategy for public health emergency management in Broome County, the Public Health Emergency
Preparedness and Response Plan expands upon the strategy by defining tactical and operational
guidelines for utilization by the Broome County Health Department and its response partners. The Plan
includes annexes which further define the operational procedures of the Broome County Health
Department when providing public health emergency response.
This Plan is a living document continuously updated to reflect new evidence-based guidance, after-
action reports and improvement plans, and lessons learned from real world events. It is developed in
collaboration with partners across all phases of public health and medical emergency management.
The Broome County Health Department provides services focusing on improving the health and well-being
of individuals, families, and the greater community of Broome County. The Broome County Health
Department accomplishes this task by consistently assessing and addressing the health needs of the
community through the offering of routine services, policy and plan development and implementation,
and by preparing for and responding to emergencies.
An emergency can occur at any time, suddenly and without warning. Proper planning is essential to
minimize the impact of any emergency on the community. The PHEPRP is designed to facilitate a timely,
effective, efficient, and coordinated emergency response to events affecting the population within
Broome County.
Maternal Child Health and Development
Mission: Promote the growth and development of children with special needs and their families
through identification, assessment, education, and service provision. Improve the health of women,
infants and children through health teaching, health counseling, and early identification of real and
potential health problems.

Broome County
94 Community Health Assessment 2019-2024
Maternal Child Health and Development
Description of Services
Maternal Child Health and Development: The assurance of optimal physical, psychosocial and
developmental health and wellbeing for childbearing and child-rearing families is the goal through
maternal child programs designed to help families receive the evaluation and treatment services they
need. Some children may experience delays in their development, and early detection and treatment
may make a difference…for the child, the family, and the community.
The programs offered through the Maternal Child Health and Development Division help ensure
physical, psychosocial and developmental health and well-being for childbearing and child-rearing
families in Broome County. Some children may experience delays in their development. Early detection
and treatment of these delays may make a difference for the child, the family, and the community. This
division offers several programs designed to help families access the detection and treatment services
they need.
Early Intervention Program (EIP) service coordinators work closely with families of children with
developmental delays and/or diagnosed conditions with a high probability of delay, to identify the
families’ concerns and priorities for their children. Individualized family service plans are constructed by
the service coordinator with the family and agreed upon by the family and the Early Intervention
Official/Designee. Early Intervention service coordinators also offer referral information to families
regarding a variety of topics, including childhood lead poisoning, health insurance and community
events where families can connect with other families of children with developmental disabilities and
delays. The Early Intervention Program is a federally mandated statewide program offering evaluations
and therapeutic support services for infants and children (from birth up to three years of age) with
special needs and their families.
Child Find: component of the Early Intervention Program focuses on ensuring at-risk children are
engaged in primary health care, will receive appropriate developmental surveillance and screening from
a primary care provider, are referred to the Early Intervention Program for a multi-disciplinary
evaluation when indicated and have health insurance coverage. There were 76 new referrals to the
Child Find Program in 2018 with 207 children actively enrolled. There were 105 new referrals to the
Child Find Program in 2017 with 251 children actively enrolled. There were 532 new referrals to the
Early Intervention Program in 2018 with 842 children actively enrolled. There were 487 new referrals to
the Early Intervention Program in 2017 with 748 children actively enrolled. The decrease in referrals and
subsequent active enrollment in Child Find is likely reflective of the increase in Early Intervention referrals
and active enrollment.
Preschool Special Education Program: from Early Intervention, a child may transition into the for
children aged three to five with suspected or confirmed delays which will affect learning. Children aged
three to five may also be referred directly to the Preschool Special Education Program. Resources
including special education and therapy (occupational, physical, and speech), are available to assist
parents of preschool children with disabilities to help them prepare their children for the transition to

Broome County
Community Health Assessment 2019-2024 95
school (kindergarten). Participation in quality learning experiences is important for all children to
achieve high educational standards. Allowing children with and without disabilities opportunities to
learn together in the least restrictive environment, whenever possible, benefits all children. Outreach is
provided to community agencies, schools, and primary care providers to streamline the referral process
for children with and at risk for developmental delays.
Education to Handicapped Children’s Program (EHCP) Committee on Preschool Special Education
(CPSE) (ages 3–5 years): The Education to Handicapped Children’s Program is a federal and state
mandated program for children, ages three through five, with suspected or confirmed delays, that will
affect learning. This program is directed through the New York State Department of Education with the
objective being the transition of identified children into the formal school system.
As with other programs, the family is an important part of the team in developing a plan based on the
identified needs of their child. The EHCP process determines placement opportunities and services to
benefit both the child and the family.
Children with Special Health Care Needs (CSHCN) Program: assists families in ascertaining community
resources, as well as providing outreach throughout the community to increase awareness of resources
available, to identify unmet health and related needs, and to collaborate with community partners to
develop plans to overcome barriers and increase access to services. Outreach activities include
participation in community health fairs and events, presentations at meetings of community and health
organizations, and informational sessions sponsored by the CSHCN grant.
Healthy Families Broome (HFB): is part of a statewide initiative, Healthy Families New York. This
program is a comprehensive prevention program that focuses on the safety of children while supporting
families. A Public Health Educator (PHE) trained by Prevent Child Abuse New York serves as a Family
Resource Specialist. The PHE offers eligible expectant families a home visit. During the home visit, the
PHE completes an in-depth psychosocial assessment with the expectant parents to assess their
strengths, needs, and challenges. The PHE provides referrals to community agencies, and eligibility is
determined for the long-term home visiting program.
Broome County Child Fatality Review Team: established in 2008, recently expanded to become the
Broome-Tioga Regional Child Fatality Review Team. This is a multidisciplinary team of
professionals established in 2019 pursuant to New York State Social Services Law (SSL) to
review the death of any child under the age of 18 whose death is unexpected or unexplained.
The Team is authorized to review any unexpected or unexplained death, but priority is given to
instances where.
➢ any child for whom Child Protective Services has an open case.
➢ any child for whom at the time his/her death has an open preventive services
case in Broome County or Tioga County.
➢ any child who at the time of his/her death was in the care and custody or
guardianship and custody of Social Services or a voluntary authorized agency.
➢ a report was made to the New York Statewide Central Register of Child Abuse
and Maltreatment involving the death of a child.

Broome County
96 Community Health Assessment 2019-2024
The mission of the B-T CFRT is to improve our understanding of how and why children die,
develop and promote a regional system of child death review and response, and to identify
systemic and policy issues, and public health interventions to improve child health, safety and
protection. Our ultimate goal is to prevent future deaths and to promote child safety through a
confidential review process which is thorough, comprehensive, and multidisciplinary.
The Broome County Health Department and key stakeholders from Tioga County Public Health
and both counties’ departments of Social Services, County Attorney, District Attorney, Sheriff,
Emergency Medical Services, and Coroners; as well as New York State Police; UHS Pediatrician;
and representatives from several community agencies meet monthly for case review. The
Broome County CFRT has discussed 104 child fatality cases from 2009 through December 2018
and has developed a formal process to identify system-based impediments to child health and
safety that will ultimately reduce the number of child deaths. The B-T CFRT adopted this same
strategy. Some interventions targeted at preventing child deaths have been recommended and
implemented by the Family Violence Prevention Council, Mothers and Babies Perinatal
Network, Broome County Health Department Maternal Child Health Division, and the Sheriff’s
Department.
Licensed Home Care Services Agency (LHCSA): home visits are made to prenatal, postpartum, and
pediatric clients. The Public Health Nurses (PHN) provide skilled nursing assessments, discuss concerns
and answer questions about health care, childcare, and child growth and development. One of the PHN
staff is a certified lactation counselor to better serve and support breastfeeding efforts in the
community. Additional areas of expertise include: home safety, psychosocial assessment, community
referrals for substance abuse, domestic violence, mental health, and ongoing parent education.
Certified Medication Administration Training (MAT): is available for child-care providers to educate
them on appropriate medication administration techniques utilizing the curriculum developed by SUNY
Training Strategies Group.
Maternal and Child Health Nursing: Broome County’s commitment to families begins before the birth
of a child, with a home visit available to expectant families from a Maternal Child Health Nurse.
Receiving high quality prenatal and postnatal care increases the likelihood that each child has a solid
foundation of health from the beginning of life. Our nurses offer care that is essential to this mission,
including skilled psychosocial assessments of maternal and child health, including breastfeeding support,
monitoring infant growth and development, providing referrals to providers and community agencies,
and promoting healthy behaviors and practices. Working closely with other Health Department
programs, such as WIC, Early Intervention, and Environmental Health, our nurses help ensure that all of
the resources provided by Broome County are mobilized to support our young families. The physical,
psychosocial, and developmental wellbeing of our childbearing and childrearing families is critical to the
overall viability and health of our community, and Maternal Child Health nurses are instrumental in
achieving that goal.
The Health Department has sponsored the Women, Infants and Children’s (WIC) Program in Broome
County since 1979. The WIC Program is a supplemental food program that services approximately 5,000

Broome County
Community Health Assessment 2019-2024 97
participants throughout the county. Clinics are held almost daily with evening and weekend hours to
meet the needs of the families enrolled. WIC nutrition staff provides nutrition education and support to
families who receive a prescribed food package every month to assist with growth and proper
development during pregnancy, lactation, infancy and early childhood up to the child’s fifth birthday.
Staff makes referrals to community agencies to assist the families with meeting their needs and goals.
The program offers an enhanced peer counseling program to support and promote breastfeeding.
Anthropometric measurements and hemoglobin levels are obtained to assist with assessment of the
clients’ health status and the staff communicates with health care providers as needed. WIC staff also
screens for elevated lead levels for children in collaboration with the Maternal Child Health and
Environmental Health staff.
Table 16. Broome County Women, Infants, Children (WIC) Program Data, 2018
Program Data
YTD 2012
(N)
Total # of Participants Served
17187
# Clinic Days
264
Average # of Participants/Day
786
# New Pregnant Women
255
# New Women (Postpartum and Breastfeeding)
95
# New Infants
109
# New Children
95
Total New Participants
554
2020 Maternal Child Health and Development Objectives
➢ Increase the number of prenatal visits to ensure early and continuous comprehensive prenatal
care to reduce infant mortality, decrease low-birth-weight babies, and increase positive birth
outcomes.
➢ Increase the number of evaluation visits to postpartum/ newborn clients to minimize
environmental hazards to reproduction/growth/development through evaluation of home
settings, health habits and nutrition status.
➢ Continue to improve breastfeeding initiation rates and duration through education provided to
prenatal clients and through support of postpartum women and infants as soon after delivery as
possible.
➢ Continue to provide home visiting, nursing assessment and education to children with identified
elevated blood lead levels and refer at risk dwellings for assessment.
➢ Train PHN staff as Certified Lactation Counselors.
➢ Train PHN to offer bereavement support to families dealing with the loss of a child.
➢ Ensure appropriate newborn bloodspot screening, follow-up testing, and referral to services.
➢ Continue to provide training in medication administration to child-care providers.
➢ Reduce fetal, infant and child death by early identification of problems, developing and
implementing interventions and providing community education.
➢ Increase the number of children screened for lead poisoning at age one and two by providing
information to parents, communicating with physicians and providing referrals to the
Environmental Health division and continuing screening of children enrolled in WIC.

Broome County
98 Community Health Assessment 2019-2024
➢ Continue to meet nutritional demands of women, infants and children through the WIC
program, continue to improve breastfeeding initiation and duration through support of the WIC
Nutrition and peer counseling staff and breast pump program.
➢ Maximize use of preventive health services through education and collaboration with local
health care providers, the Clinic Division, Department of Social Services, schools, New York State
Department of Health, and child-care providers.
➢ Expand Healthy Family Broome (HFB) program throughout Broome County and increase the
number of families served.
➢ HFB’s Public Health Educator offers assessments to expectant and new families to assess their
strengths and needs. Offer families information regarding local community resources and
connect eligible families to Healthy Families Broome home visiting program.
➢ Continue to review and update Quality Assurance Corporate Compliance Plan in the division to
ensure program integrity, accuracy, appropriate authorization of service and quality of care.
➢ Ongoing and increasing need for services in both the Early Intervention Program and the
Preschool Special Education Program demands assurance of adequate capacity of needed
services for infants and children identified as having developmental and/or learning delays
and/or being at risk for developmental delays. Continue working to identify new service
providers, including expansion of individual contracts in the Preschool Special Education
Program.
➢ Continue to work successfully to accommodate billing changes in the Early Intervention
Program, working with families and providers to obtain all information required to maximize
third party insurance payments.
➢ Develop procedures to monitor and review the payment of Early Intervention Program services
not covered by third party insurance through the Escrow account billed to the county.
➢ Continue to strive to meet both federal and state performance standards in the Early
Intervention Program.
➢ Collecting and reporting child outcomes is a requirement of the Individuals with Disabilities Act
(IDEA). The performance of the New York State Part C Early Intervention Program on improving
child outcomes is now reported in the Annual Performance Report. Strive to improve child
outcomes for children enrolled at least six months in the Broome County Early Intervention
Program.
➢ Improving family perceptions and outcomes of the Early Intervention Program is now also
included in the Annual Performance Report. Actively participate in the Improving Family
Centeredness Together State initiative to identify and address needs to help Early Intervention
families fee more connected.
➢ Identify and participate in various community organizations to better foster collaboration and
increase awareness of available services.
➢ Continue conservative fiscal management of the Children with Special Needs Programs while
meeting Federal and State regulations.
➢ Continue to work with and utilize the preschool software program intended for billing Medicaid
to maximize reimbursement of eligible services and efficiently capture data that will be useful in
completing reports to assist in better program management.
➢ Work with the preschool software program to develop procedures to review and address denied
Medicaid claims.
Broome County
Community Health Assessment 2019-2024 99
➢ Continue to develop procedures for monitoring of services provided in the Early Intervention
and Preschool Special Education Program to ensure that plans developed for each child match
both their needs and their ability to participate.
➢ Continue dialogue with Committee on Preschool Special Education Chairpersons, tuition-based
programs, and NYS Education Regional Associates to ensure that eligible children are receiving
Free Appropriate Public Education (FAPE) in the Least Restrictive Environment (LRE).
➢ Continue to identify models and procedures which will promote efficient use of providers’ time
as well as maximizing desired results for children and families.
➢ Work with New York State BEI and regional/local agencies to determine the impact of Health
Homes for Children and respond accordingly.
2020 Maternal Child Health and Development Budget Highlights
➢ Continue to identify vulnerable families and implement areas of collaboration with Department
of Social Services and other human service providers to prevent child abuse/neglect.
➢ Continue to develop better infrastructure to supplement operating budget costs with third party
insurance revenue, state aid and grant funding.
➢ Continue to assist families in ascertaining community resources to meet their health care needs,
through referrals and linkages with community agencies.
➢ Use local data to expand resources and motivate action toward elimination of lead poisoning in
collaboration with the Environmental Health Division and more community agencies.
➢ Review salary of PHN position in order to be more competitive and better able to recruit
registered nurses for employment.
➢ The New York State Department of Health still does not have a target date when system reports
in NYEIS will be fully operational. The Bureau of Early Intervention has been routinely providing
reports not currently available in NYEIS to municipalities to improve the ability to meet federal
and state performance standards.
➢ The New York State Early Intervention State Fiscal Agent continues to work to maximize
insurance payments for covered services in the Early Intervention Program. Third party
insurance coverage of services in the Early Intervention Program remains marginal, with
Medicaid and Escrow funds bearing the majority of the costs. Work to ensure that Medicaid
coverage is fully utilized before payments are made from Escrow funds.
➢ Ongoing and increasing requirements of children with disabilities and developmental delays will
continue to challenge the department to find resources to meet their needs. As the national
incidence of young children diagnosed as having Autism rises, the increase is being seen at the
local level as well. This will continue to present a challenge to identify appropriate services that
will adequately support them and meet their needs.
➢ Understanding of the effects of Adverse Childhood Experiences is emerging. Focus efforts to
increase awareness and develop ways to support survivors

Broome County
100 Community Health Assessment 2019-2024
Environmental Health
Description of Services
The Division of Environmental Health conducts routine inspections of approximately 1,500 regulated
facilities, responds to complaints of public health nuisances, rabies control, enforces the Clean Indoor
Air Act and the Adolescent Tobacco Use Prevention Act, reviews plans for public water and private
sewage disposal systems, permitting and regulation of swimming pools, bathing beaches, mobile home
parks, hotels/motels, food facilities, campgrounds, children camps, coordinates lead poisoning
prevention efforts and the Healthy Neighborhood Program, Lyme disease education, conducts
communicable disease outbreak investigations and educates facility operators with training courses and
the general public with appearances and media releases. The Division of Environmental Health also
responds to emergencies and participates in other department emergency planning initiatives.
The programs offered by the Environmental Health Division strive to preserve and protect the public and
the quality of the environment as it impacts the public health of Broome County and to prevent illness
and injuries caused by environmental factors. This division is charged with providing information on and
the necessary enforcement of state and local health laws, codes and standards that apply to various
facilities and systems. The services performed include the following:
Water quality (public supplies), Residential sewage systems, food safety, lead poisoning prevention,
public health nuisances, regulation of bathing beaches, public swimming pools, children’s camps, hotels
and campgrounds, Indoor Air Quality / Clean Indoor Air Act, Toxins / Environmental Assessments, Youth
Tobacco Use Prevention, Rabies, Emergency Preparedness and Response, Mobile Home Parks, Tick-
Borne Disease Prevention, Healthy Neighborhoods, Educational Materials Only on West Nile Virus,
Tattoos and Body Piercings, Bed Bugs, and Tanning.
Environmental Health
Mission: To promote the public health and prevent communicable disease, chronic conditions and
injury by providing technical assistance to the regulated community and education to the public in
various program areas, including but not limited to food service, emergency preparedness, water
and air quality, rabies control, lead poisoning prevention, swimming pool inspections and public
health nuisances. The Division is charged with the enforcement of the New York State Sanitary Code,
the Broome County Sanitary Code and sections of the Public Health Law.

Broome County
Community Health Assessment 2019-2024 101
Lead Poisoning Prevention:
Childhood Lead Poisoning Prevention: Lead poisoning is caused by eating, drinking or
breathing anything with lead in it. It can slow a child’s normal growth and development and can
cause mental retardation, kidney disease, liver damage, blindness or death. Regular testing on
children up to six years of age is required to identify the problem early. The Lead Poisoning
Prevention Program is managed by the Broome County Health Department with testing done
by health department clinic staff, private physicians, and medical clinics. Advice on cleaning the
child's environment, nutrition, housekeeping, working with landlords/property owners and
physicians, and retesting are part of the follow-up when an elevated lead level is found. Data
for the lead prevention program for 2018 are detailed below.
Childhood Lead: The Broome County Health Department offers services to all children with
elevated blood lead levels through the Childhood Lead Program. This program coordinates
appropriate follow-up for lead poisoned children. Staff members educate parents about
strategies to prevent lead exposure to reduce lead hazards as well as conduct environmental
investigations. Referrals are made to other agencies and programs as needed and staff coordinate
communications between the Regional Lead Poisoning Resource Center, health care providers
and parents.
Primary Prevention: Primary prevention staff educates, identifies, and requires correction of
lead-based paint hazards in high-risk housing prior to a child being diagnosed with an elevated
blood lead level.
Lead Hazard Control Grant (HUD): This program is designed to fund the cost of controlling lead
paint hazards in low-income housing. Grant funding is available in the form of five-year forgivable
loans for both rental and owner-occupied housing units built before 1978. This program accepts
referrals from partner agencies, property owners and tenants to inspect older homes with young
children. To be eligible, units must house or be regularly visited by at least one child age six or
younger or a pregnant woman. All work is completed by certified lead abatement contractors
selected by the program.
Table 17. Blood lead tests by age group of the child at testing during the selected time frame
01/01/2018 – 12/31/2018
Lead Values (mcg/dL)
0 to <5
5 to <10
10 to14
15 to 19
20 to 44
45 to 69
70+
# Children
2801
163
27
18
27
5
2

Broome County
102 Community Health Assessment 2019-2024
Table 18. Blood lead tests by age group of the child at testing during the selected time frame
01/01/2018 – 12/31/2018
Age Group (months)
Blood Lead
Level
(mcg/dL)*
< 9
months
9 to < 18
months
18 to < 36
months
36 to < 48
months
48 to < 60
months
60 to < 72
months
72+
months
0 to < 5
41
1225
1014
208
139
61
113
5 to < 10
1
48
72
25
9
2
6
10 to 14
0
4
15
3
0
0
5
15 to 19
0
2
7
4
3
0
2
20 to 44
0
3
8
8
7
0
1
45 to 69
0
0
1
4
0
0
0
70+
0
0
0
2
0
0
0
Healthy Neighborhoods: The Healthy Neighborhoods Program addresses the environmental and health
needs of residents living in geographically targeted neighborhoods within Broome County. Grant funds
are used to implement a program designed to reduce residential injuries, childhood lead poisoning,
hospitalizations due to asthma, and exposure to indoor air pollutants.
Water Supplies: Inspect, survey, educate and monitor the various public water supplies in accordance
with Part 5 of the NYS Sanitary Code. Review plans for the construction, addition, or modification of any
public water supply to assure compliance with State and Federal Regulations. Require correction of any
violations and provide technical assistance to water supply operators to comply with Part 5 of the NYS
Sanitary Code. Provide technical information to well owners.
Wastewater Treatment: Division of Environmental Health staff reviews, inspects, educates and takes
enforcement actions as needed, designs, and provides approval of existing residential systems seeking
modifications or corrections. Plan reviews are completed for new systems as well as enforcement of
nuisance complaints regarding failing systems. Permits and approvals are provided in accordance with
both New York State and Broome County Sanitary Codes. Staff review and provide approval of all
proposed wastewater disposal systems (10,000 gallons) for new construction or modifications to existing
systems. Approval is issued in accordance with NYS Department of Environmental Conservation SPDES
(State Pollutant Discharge Elimination System) Permits and Standards for Waste Treatment Works.
Emergency Response: Staff responds to events resulting in the discharge of liquid, gaseous or solid
materials that may produce an environmental hazard. Follow-up action is coordinated to eliminate
problems and determine that all public hazards are eliminated. Environmental Health is an active
member of the Local Emergency Planning Committee to plan and respond to natural and manmade
disasters.
Subdivisions: Review and provide approvals for plans and specifications for realty subdivisions. This
includes the development of water supplies and design of wastewater disposal systems.

Broome County
Community Health Assessment 2019-2024 103
Adolescent Tobacco Use Prevention & Clean Indoor Act: Staff enforces NYS Public Health Law
requirements for the sale of tobacco products including vaping products, provides community
awareness on tobacco issues, and enforces the Clean Indoor Air Act prohibiting smoking in enclosed
public areas.
Indoor Air Quality (non-tobacco): Investigate complaints of impacted indoor air quality. Provide
recommendations concerning corrective action and suggest laboratories for required analyses or
collection of necessary samples. Recent air quality problems have involved PCBs, asbestos, chlordane,
radon and chlorinated solvents.
Toxic/Solid Waste Dumpsites: Investigate and report on dumpsites in Broome County which may
present a potential public health problem. Review and comment on any reports completed concerning
remedial actions, hydrogeological data collected, and proposed construction. Respond to chemical
emergencies that may produce hazards; review remediation activities to reduce public health hazards.
Food Service: Inspect, investigate, educate and take enforcement action as needed over all regulated
food service facilities in Broome County.
Mobile Home Parks: Inspect, educate and take enforcement action on any violations for mobile home
parks per Part 17 of the NYS Sanitary Code including public water supplies and sewage systems.
Temporary Residences, Campgrounds and Children’s Camps: Inspect, educate and take enforcement
action on any violations for hotel/motels, travel trailer campgrounds and children's camps per Part 7 of
the NYS Sanitary Code. This includes reviewing and approving plans for construction, alteration and/or
modification of proposed or existing buildings as well as children’s camp supervision and safety
requirements. Regulation of sewage and water supplies as well.
Rabies Control: Staff members investigate reports of animal exposures, ship suspected rabid animals to
the state laboratory, and provide outreach and education. Staff enforce 10-day confinement periods and
quarantine, support free rabies clinics and provide authorization of rabies prophylaxis.
Swimming Pools and Beaches: The Division of Environmental Health inspects, educates and takes
enforcement actions as needed on all public swimming pools and bathing beaches in Broome County in
accordance with Part 6 of the NYS Sanitary Code.
Public Health Nuisances: The Division of Environmental Health responds to or makes referrals to
appropriate agencies to report rodents, outdoor burning, household garbage complaints, and sale of
Bath Salts and Synthetic Marijuana.
General Environmental Health educational information is available on the following topics: West Nile
Virus, Lyme disease, Mold, Bedbugs, Tattoo Guidance and Tanning.

Broome County
104 Community Health Assessment 2019-2024
2020 Environmental Health Objectives
➢ Continue to monitor and reduce public health hazards found during inspections within
program areas, along with increased education and enforcement actions.
➢ Implement new program policies and procedures to maintain accountability and efficiency.
➢ Modify Environmental Health staff roles to meet the increasing demands with limited staff
and funding.
➢ Prioritize program objectives to those of high risk. Cut or limit non-mandated programs to
meet budget constraints.
➢ Modify inspection protocols to increase program efficiency and minimize excessive travel.
➢ Increase educational awareness of Environmental Health issues via free in-house and on-line
training courses, smart phone apps and media.
➢ Develop partnerships with all municipal code enforcement officers to minimize residential
environmental hazards.
2020 Environmental Health Budget Highlights
➢ Continue to pursue grants to decrease net county support.
➢ Minimize unnecessary and costly human post exposure prophylaxis by providing health care
specialists the tools necessary to make sound judgments when providing treatment.
➢ Continue to meet all New York State Department of Health program deliverables with a
limited and static budget.
Clinic Services
Description of Services
The Clinic Division provides specialized clinic services in an outpatient care setting. The primary site is
located at 225 Front Street and immunization and outreach services are provided at several locations
throughout the County. The division is comprised of six basic program areas: Communicable Disease,
Employee Health, HIV Testing, Immunization, Sexually Transmitted Diseases, and Tuberculosis. The Clinic
Division currently manages three grants which enable the department to provide additional HIV testing,
both anonymous and confidential, outreach and education on HIV counseling, testing, referral, and
partner notification. The Immunization Action Plan grant is designed to increase immunization rates
through surveillance and education of local healthcare providers as well as outreach to homeless
shelters and the County corrections facility to improve Hepatitis A and B and Influenza immunization
rates. Descriptions of the services previously listed are explained further in the following section. The
addition of program Data will provide an understanding of the array of programs offered to the public
and the impact that this division has on the community.
Clinic Services
The Broome County Health Department Clinic Services Division focuses on prevention of the
transmission of infection and communicable diseases through the coordination of community
resources, surveillance, health education, consultation and direct care based on community need.

Broome County
Community Health Assessment 2019-2024 105
Communicable Disease Control: An important role of the local health department is to investigate
diseases that the New York State Department of Health designates as reportable. When an individual
contracts a disease such as measles, hepatitis, or meningitis, reports to the Health Department are
required from physicians, hospitals, and laboratories. The nurses who work in disease control speak with
the person or parent/ guardian to determine the source of the disease, identify others at risk, and
recommend needed treatment. All information is protected and treated confidentially. Fact sheets and
printed materials are also available to the public by request. Mandated diseased reported in 2016 was
496 and 551 in 2017. The largest reporting of any disease was 246 Chronic Hepatitis C cases. Lyme
disease cases increased from 66 to 105 in 2017. Group B Strep cases decreased from 35 in 2016 to 27 in
2017.
Table 19. Communicable Disease Investigation Report, 2018
COMMUNICABLE DISEASE REPORT -YEAR 2018
DISEASE
#
Reported
Amebiasis
1
Campylobacteriosis
16
Crytosporidia
4
E coli: Shiga toxin producing
3
Giardiasis
8
Salmonellosis
23
Shigellosis
4
Yersiniosis
Hepatitis A
1
Hepatitis B, acute
2
Hepatitis B, pregnant carrier
1
Hepatitis B, chronic unduplicated
15
Hepatitis C, acute
41
Hepatitis C, chronic unduplicated
208
Measles
Mumps
2
Rubella
Pertussis
5
Aseptic/ viral meningitis
8
Group A Strep, invasive
7
Group B Strep, invasive
28
Haemophilus influenzae, invasive
2
Meningococcemia, Meningococcal Meningitis
1
Pneumococcal infection, sensitive to penicillin
24
Pneumococcal infection, resistant to penicillin
1
Other bacterial meningitis
West Nile infection
2
Other viral encephalitis
Legionella
10
Listeriosis
1

Broome County
106 Community Health Assessment 2019-2024
COMMUNICABLE DISEASE REPORT -YEAR 2018
DISEASE
#
Reported
Anaplasmosis
12
Babesiosis
Ehrlichiosis
5
Lyme disease
58
Malaria
Rocky Mountain Spotted Fever
4
Miscellaneous
1
TOTAL
498
Tuberculosis Control Clinic: The Tuberculosis (TB) Control Clinic provides for the diagnosis, treatment,
prevention, and control of TB in Broome County. An individual who is suspected of having TB is
interviewed by a clinic nurse and referred for a chest x-ray and other tests, as indicated. The clinic
physician discusses treatment recommendations with the individual. Medication is provided through the
clinic and follow-up appointments are made for the client. As with other communicable diseases, it is
sometimes necessary for other family members, or close contacts of the client, to be tested/examined
at the clinic as well.
The Tuberculosis Control Clinic reaches out to identify individuals in targeted populations at high risk for
exposure to TB who have been infected but are not yet contagious. Staff will conduct outreach to find
these individuals and provide treatment before they become ill and contagious to others. The Clinic
serves as a resource for other health professionals, health care facilities, and congregate living
establishments in the community. Referrals from these sources are welcome. The clinic nurse is
available to answer questions and to provide educational presentations and materials.
Hepatitis C Testing: In accordance with NYS law, Hepatitis C testing is offered to all persons born
between 1945-1965. People in this age group account for the majority of those infected with Hepatitis
C. Risk factors specific to Hepatitis C include sharing a needle to inject drugs (even once many years
ago), receiving a blood transfusion before 1992, receiving clotting factors before 1987 or having been on
long tern kidney dialysis, having tattoos or piercings done in an unprofessional setting, or snorting drugs.

Broome County
Community Health Assessment 2019-2024 107
Table 20. Chest Clinic – Program Data, 2018
Program Data
2018
(N)
Clinic Visits
627
Patients Seen
314
Mantoux Administered
152
Patients Started on Preventative Treatment
58
Medication Refills
134
Suspect TB Cases and Investigations
0
Confirmed Active TB Cases
5
DOT (Directly Observed Therapy)
341
Immunization Action Plan Grant: The Immunization Action Plan is a grant that is funded by the New
York State Department of Health. The goals of the grant are to increase childhood, adolescent and adult
immunization rates in Broome County, to ensure that all vaccination records are completely and
accurately entered in NYSIIS (NYS Immunization Information System), and to increase immunization
focused education, information, and training opportunities to local health department staff, the public,
health care providers, local schools and day care centers. Our objectives are to increase 4:3:1:3:3:1:4
childhood immunization coverage among county children aged 19-35 month and increase HPV
vaccination coverage among county girls and boys aged 13 years according to targets described in the
vaccination coverage guidance document. In addition, we are commissioned with ensuring that
Perinatal Hepatitis B Prevention Program (PHBPP) case management is completed consistent with CDC
guidance and NYS public health law 2500e and regulations by 24 months of age; to increasing county
specific influenza vaccination coverage among adults aged 18+ years by five percentage points from the
2016 baseline as measured through eBRFSS; achieving a measurable improvement in underserved
population using evidence-based interventions.
Immunizations: There is a clinic at the Broome County Health Department that offers all of the routine
childhood immunizations: Polio, Hepatitis B, Hepatitis A, Diphtheria-Tetanus-Acellular Pertussis (DTAP),
HPV, Rotavirus, Hemophilus Influenzae B (Hib), Pneumococcal Conjugate, Measles-Mumps-Rubella
(MMR), and Varicella. Tetanus-diphtheria (Td), Tdap for adults, and meningococcal vaccine are offered
for college students. Flu vaccine is offered during flu season at the Broome County Health Department.
Flu vaccine is given to persons at risk on a seasonal basis.
Table 21. Immunization Clinics – Program Data, 2018
Program Data
Routine
(N)
Sessions
79
Visits
334
Immunizations
1,576

Broome County
108 Community Health Assessment 2019-2024
Table 22. Immunization/Vaccine Data, 2018
Type of Vaccine Administered
YTD 2018
(N)
Pediatric Pneumococcal
2
DtaP
12
Rotavirus
1
Varicella
38
TD
17
HIB
2
IPV
35
MMR
67
Flu
998
Pneumococcal
2
HPV
65
Pediatric Hep B
27
Adult Hep B
8
Tdap
112
Hep A/Hep B (Twinrix)
8
Pediatric Hep A
22
Typhoid
0
Yellow Fever
0
Meningitis 4
103
Meningitis B
9
Rabies
9
Adult Hep A
9
DTAP & IPV
10
DTAP, IPV & HIB
0
Pediarix (DTAP & Hep B & IPV)
2

Broome County
Community Health Assessment 2019-2024 109
Sexually Transmitted Disease (STD) Clinic: The Sexually Transmitted Disease (STD) Clinic is available to
those people who are at risk or may have come in contact with one or more sexually transmitted
diseases. There is no charge to Broome County residents for STD testing and treatment. A confidential
interview by a professional staff member includes asking about the clients’ symptoms, their sexual
activities and other information important to the diagnosis of their problem.
Following the interview is an examination, which will include getting samples of blood, discharges or
other specimens for laboratory testing. Some of the tests will be done at the time of the visit so the
results are known immediately. Other tests will take approximately 1 week to get back results. Once the
diagnosis has been made, medication is either prescribed or given at a time of the visit, depending upon
the diagnosis. Instructions will be given on how to take the medicine, how to prevent re-infection and
how to obtain lab results. Recommendations for partner treatment are made, if needed.
Rapid HIV testing is offered to anyone attending the STD Clinic. Both confidential and anonymous rapid
HIV testing is offered. Everything that is discussed in the STD Clinic, including test results, is confidential.
Nothing can be discussed with someone else without the client’s written consent.
Table 23. STD Clinic – Program Data, 2017
Program Data
2017
(N)
STD Clinic Visits
1,285
STD Clinic Total Sessions
171
Broome County Jail Clinic Visits
592
Table 24. STD Clinic Diagnosis – Program Data, 2017
Most Frequent Diagnoses
2017
(N)
Nongonococcal/Urethritis
85
Human Papilloma Virus
97
Chlamydia*
87
Gonorrhea**
31
Syphilis
15
Trichomoniasis
56
*605 cases diagnosed in Broome County, 87 of which were diagnosed at the Broome County Health Department
**114 cases diagnosed in Broome County, 31 of which were diagnosed at the Broome County Health Department

Broome County
110 Community Health Assessment 2019-2024
HIV Counseling and Testing Services: Clinical testing is the only way to determine if a person is infected
with HIV, the virus that leads to AIDS. Early diagnosis and treatment can improve the quality of life for a
person with the virus. Confidential and anonymous HIV testing is available through the STD Clinic (778-
2839), but there are also times set aside specifically for HIV testing with trained HIV test counselors. The
Broome County Health Department does rapid HIV testing and accurate results are available in 10-20
minutes. Call 1-800-562-9423 to make an appointment for anonymous HIV testing at the Health
Department, Southern Tier AIDS Program, or throughout the region. Specially trained staff can provide
information and programs about HIV/AIDS to individuals and groups.
PrEP Grant: This grant is funded through NY State and has been awarded to United Health Services
(UHS), we have been subcontracted to provide education and outreach services in Broome,
Tioga, and Chenango county. The focus of the grant is to educate, medical providers and
personnel as well as populations that are at very high risk for HIV, on PrEP (Pre-Exposure
Prophylaxis). PrEP is an evidence-based, biomedical intervention with proven efficacy to prevent
HIV infection in individuals at highest risk for HIV. PrEP is part of Governor Cuomo’s 3-point plan
to end the AIDS epidemic in NY State and decrease the number of new HIV infections by 2020.
Southern Tier AIDS Anonymous Program (STAP): The New York State Department of Health provides
funding with a Broome County match for a HIV Program Representative who provides the anonymous
testing at the Broome County Health Department, the Southern Tier AIDS Program (STAP) office, and
many community-based organizations that provide services to individuals at risk for HIV infection.
School Based Dental Sealant Program Grant: This grant is funded by the NYS Department of
Health. The Broome County Health Department has subcontracted with the Lourdes Hospital
Center for Oral Health to render services in five local school district elementary schools
(Thomas Jefferson, Horace Mann, Calvin Coolidge, MacArthur, and Woodrow Wilson) using
their mobile van units to enhance health promotion and disease prevention activities and
provide underserved children a point of entry into the dental health care system. The objectives
of the grant include establishing or expanding preventive service models for providing dental
prevention services (specifically dental sealants) to underserved populations, to improve
participation rates of dentists in public insurance programs, and to develop case management
models to address the needs of difficult-to-reach school-aged populations.
Table 25. School-Based Health Center Dental Program (SBHC-D), 2018-2019
Program Data
2018-2019
Grant Year
Number of consent forms returned
384
Number of children who received oral screening/ examination
194
Number of children who received oral prophylaxis
104
Number of children who received topical fluoride
149
Number of children who received sealants
35
Number of children who received oral health education
174
Number of children who received treatment services on site at the SBHC-D
26
Number of children who were referred for treatment to off-site dental services of the
Article 28 operator or in the community
44

Broome County
Community Health Assessment 2019-2024 111
Program Data
2018-2019
Grant Year
Number of 2nd and 3rd grade children who returned consent forms
101
Number of 2nd grade children who received sealants through the School Based Sealant
Program (SBSP)
6
Number of 3
rd
grade children who received sealants through the SBSP
1
Number of 3rd grade children whose sealants were applied by the SBSP were retained at
next reassessment (6-15 mos.)
1
Number of 2nd and 3rd grade children who received treatment services on site at the SBSP
12
Number of 2nd and 3rd grade children who were referred for treatment to off-site dental
services of the Article 28 operator or in the community
34
Number of 2nd and 3rd grade children who were referred for urgent dental treatment to
off-site dental services of the Article 28 operator or in the community
16
Number of 2nd and 3rd grade children who were referred for urgent dental treatment to
off-site dental services who completed a follow-up visit
1
Number of 2nd and 3rd grade children who received oral prophylaxis
34
Number of 2nd and 3rd grade children who received topical fluoride
49
2020 Clinics Objectives
➢ Through a coordinated effort, participate in and collaborate with community agencies in a
community-wide emergency preparedness response plan including development and
implementation of regional stockpile distribution and mass immunization/prophylaxis clinics.
➢ The community will continue to be served by a system to monitor infectious diseases by subgroup.
➢ Prevent and minimize vaccine-preventable diseases by providing education, surveillance and
direct service as needed.
➢ Reduce the transmission of sexually transmitted diseases by providing education, surveillance and
direct service as needed.
➢ Prevent HIV infection in individuals at highest risk for HIV, through outreach and education on
PrEP (Pre-exposure Prophylaxis). PrEP is part of Governor Cuomo’s 3-point plan to end the AIDS
epidemic in NY State and decrease the number of new HIV infections by 2020. Continue to offer
confidential and anonymous HIV testing.
➢ Evaluate for tuberculosis infection and reduce transmission by providing targeted testing,
education, surveillance and direct service to populations at risk.
➢ Provide oral health education and preventive dental services to elementary school children
through contracted services with Lourdes Center for Oral Health.
➢ Implement an electronic medical record system and become bi-directional with the local RHIO.
2020 Clinics Budget Highlights
➢ Continue to expand revenue collection procedures for all services, including sexually transmitted
disease services by establishing contracts with third party payers and continuing to bill for sexually
transmitted disease services with patient approval.
➢ Maximize grant revenues to support the operating budget. Several grants help maintain our
operating costs down, these include the IAP (Immunization Action Program) Grant, PrEP Grant,

Broome County
112 Community Health Assessment 2019-2024
the STAP (Southern Tier Aids Program) Anonymous Grant, and the Broome County Sheriff’s
Correctional Facility Grant.
➢ Increase staff development and training in their fields of expertise and programs, i.e. Tuberculosis,
sexually transmitted disease, immunizations, and communicable disease.
➢ Insight software training on the Electronic Medical Records (EMR) Modules to smoothly
implement the EMR system.
Chronic Disease and Injury Prevention Program Grants
Cancer Services Program of the Southern Tier (CSP): The Broome County Health Department has been
the lead agency for the Cancer Services Program, serving Broome and surrounding counties for over
twenty years. Currently, the Cancer Services Program of the Southern Tier serves Broome, Chemung,
Chenango, Schuyler, and Tioga Counties. This is a unique collaboration of government, community-
based organizations and health care partners that promote services through outreach, education, and
case management to overcome healthcare barriers and increase cancer screening rates in our area. The
NYS Department of Health and the Centers for Disease Control and Prevention (CDC) provide funding for
local community health care practitioners to offer clinical breast exams, mammograms, Pap tests/pelvic
exams, colorectal screenings, and limited diagnostic follow-up procedures.
The Medicaid Cancer Treatment Program provides Medicaid Health Insurance Coverage for CSP clients
utilizing the CSP income eligibility criteria. The CSP does not reimburse for prostate cancer screenings
but provides Medicaid Cancer Treatment Program coverage for uninsured men diagnosed with the
disease if they are eligible
Table 26. Cancer Services Program of the Southern Tier Data, 2018
Procedure
2018
Cancer Screenings Reimbursed Through Broome, Chemung, Chenango, Schuyler and Tioga
Counties
Clinical Breast Exams
213
Mammogram Screening / Diagnostic Mammograms
191/44
Pap Test/Pelvic Exam
63
Colorectal FIT
109
Medicaid Cancer Treatment Program Applications
New Breast Cancer/ Renewal 6n – 1.3 R
The Community Cancer Prevention in Action Grant (CPiA): is a five-year (2018-2023) public health
imitative funded by the New York State Department of Health’s Bureau of Chronic Disease with the goal
of supporting local cancer prevention and risk reduction interventions using a policy, systems, and
environmental change approach. Broome County was one of only four grantees in the state awarded the
grant and covers targeted areas in Broome and Tioga Counties. CPiA works within 6 school districts and
their respective communities, businesses, and health care organizations to promote the grant initiatives.
These areas include: Binghamton, Deposit, Harpursville, Johnson City, Maine-Endwell, and Owego-

Broome County
Community Health Assessment 2019-2024 113
Appalachian. The primary goals of CPiA include: increasing knowledge of the dangers of indoor tanning
and UV radiation, increasing sun safety policies, increasing policies for paid leave time for cancer
screenings, and increase community knowledge of the HPV vaccine.
Tobacco Free Broome & Tioga: Advancing Tobacco Free Communities Grantee, is working to change
the community environment to support New York State’s tobacco-free norm through youth action and
community engagement. Our goal is to educate, engage, and mobilize youth, parents, and community
leaders to take action in creating lasting changes that will decrease tobacco industry impact in our
community. Our Community Engagement and Reality Check coordinators work together to: reduce the
negative influence of tobacco product marketing on youth and adults at retail outlets, increase number
of public outdoor areas where tobacco use is prohibited (parks, public grounds) to promote clean air,
eliminate second hand smoke exposure in multi-unit housing with an emphasis on protection of low-
income residents, and promote policies that reduce tobacco use imagery in youth rated movies, on the
internet and social media.
Table 27. Recent Policies Enacted in Broome County
Policies Obtained in Broome County
Impact
Tobacco/Smoke Free Parks (partial or entire park)
15 municipalities
Tobacco/Smoke Free Grounds
(businesses/libraries/agencies)
55
Tobacco Free College Campus
4
Smoke Free Housing
6 low income Housing Management Companies have
adopted 100% tobacco free indoor policies
Letters of Support to Reduce the Density of
Tobacco Retailers or Their Proximity to
Schools/Playgrounds/Parks
Over 50
Broome County Traffic Safety/Injury Control: The Broome County Traffic Safety Community Education
Project seeks to reduce the number of traffic related injuries and fatalities through community
education programs and service. This program heightens public awareness on issues such as child
passenger safety, bike/pedestrian safety, teen safe driving, occupant restraint use, older driving safety,
veteran safety and motorcycle safety.
Table 28. Community Programs by the Broome County Traffic Safety
Community Education Project, 2018-2019
Traffic Safety Focus Area
Traffic Safety Measures
# between
10/1/18-9/30/19
Child Passenger Safety (CPS)
Child Safety Seat Misuse Percentage
81%
# Child Safety Seat Inspections
300
# Child Safety Seats Distributed
165
# Educational Programs
22
# Child Safety Seat Check Events
8

Broome County
114 Community Health Assessment 2019-2024
Traffic Safety Focus Area
Traffic Safety Measures
# between
10/1/18-9/30/19
# Certified CPS Technicians
30
Bike/ Pedestrian Safety
# Educational Programs
14
# Bicycle Helmets Distributed
158
# Elementary Schools that received Bike/ Ped Poster
37
Teen Driver Safety
Held the 7
th
Annual Teen Traffic Safety day (School
Districts; Students)
20; 650
# of teen driver safety presentations
25
Motorcycle Safety
# of Lawn Signs Distributed
125
Older Driver Safety
# of CarFit Events (Events; Drivers Evaluated)
3; 33
Creating Healthy Schools and Communities (CHSC): is a five-year (2015-2020), public health initiative of
the New York State Department of Health (NYSDOH) with the goal of reducing major risk factors of
obesity, diabetes, and other chronic diseases in 85 high-need school districts and associated
communities. In 2015, the Broome County Health Department was awarded the CHSC grant and has
worked with four high-needs school districts and their communities to decrease the risk of chronic
disease associated with poor diet and inactivity. The targeted areas include Binghamton, Deposit,
Harpursville, and Johnson City. The Broome County Health Department has worked with the CHSC
school districts and communities to improve access to healthy, affordable foods and opportunities for
physical activity. Examples of these measures include implementing Complete Streets policies;
increasing physical activity physical activity in the community, at child care centers, and before, during,
and after the school day; promoting healthful eating for all students in grades K-12 by increasing the
availability of local fruits and vegetables and increasing access to healthier foods and beverages;
increasing access to chronic disease preventative services and community-based resources; and
incorporating Safe Routes to School within CHSC school districts.
Older Adult Fall Prevention Grants: From 2010 until 2015, The Broome County Health Department was
the lead agency for a five-year Fall Prevention Grant funded by the New York State Department of
Health. The purpose of the program was to reduce falls among older adults by employing evidence-
based strategies within the community and health care delivery system. The grant program funded
three evidence-based community programs and one pilot project called STEADI (STopping Elderly
Accidents, Deaths and Injuries) that supports the implementation of health care provider fall risk
assessments into the local health care delivery system. The three evidence-based community programs
are Tai Chi-Moving for Better Balance, Stepping On Program, and Otago Program. Since April 2017, the
Broome County Health Department, Binghamton University and United Health Services were funded by
the National Network of Public Health Institutes (NNPHI) to evaluate the STEADI program. Broome
County served as an alpha test site for STEADI as requested by the Centers of Disease Control and
Prevention. As part of the evaluation, an initial manuscript article was published with the NYSDOH,
NNPHI, CDC, and Binghamton University. The link to the publication:
https://www.ncbi.nlm.nih.gov/pubmed/30239774

Broome County
Community Health Assessment 2019-2024 115
Child Fatality Review Team Report
Our vision is that all children live in safe and nurturing homes free from abuse, neglect or exploitation
This Community Report provides general findings of Broome County’s Child Fatality Review Team from
104 cases reviewed to date. These reviews occurred between March 2009 and December 2018. These
reviews involved child deaths occurring from 2007-2018. Case specific findings have also been identified.
Those specific findings are currently being followed up on in a variety of ways by Broome County’s Child
Fatality Review Team members and community partners.
Introduction
The Broome County Child Fatality Review Team (BC CFRT) is a multidisciplinary team of professionals
established in 2008 pursuant to Section 422-b and 20(5) of New York State Social Services Law (SSL),
“for the purpose of investigating the death of any child whose care and custody or custody and
guardianship has been transferred to an authorized agency, other than a vulnerable child as defined
in article eleven of this chapter, any child for whom child protective services has an open case, any
child for whom the local department of social services has an open preventive services case, and in
the case of a report made to the statewide central register of child abuse and maltreatment
involving the death of a child. A fatality review team may also investigate any unexplained or
unexpected death of any child under the age of eighteen.”
The mission of the BC CFRT is to improve our understanding of how and why children die, develop and
promote a countywide system of child death review and response, and to identify systemic and policy
issues, and public health interventions to improve child health, safety and protection. Our ultimate goal
is to prevent future deaths and to promote child safety through a confidential review process which is
thorough, comprehensive, and multidisciplinary. Our tasks include the following:
Examine the manner, cause and circumstances of a child’s death.
Examine the investigative actions of agencies as applicable.
Identify risk factors and trends in child deaths.
Identify specific barriers and systems issues involved in the deaths of children.
Increase public awareness, through education and advocacy, of the issues identified as affecting
the health and safety of children.
Promote policies, practices, and legislation (when appropriate) and expand efforts in child
health and safety to prevent child deaths.
Improve communication and linkages among local and state agencies and coordination of
efforts.
Develop strategies to improve the accurate identification and uniform consistent reporting of
the cause and manner of death, improve the death investigation process, and improve
responses to protect siblings and other children in the homes of deceased children.
Identify training needs for professionals.

Broome County
116 Community Health Assessment 2019-2024
Team membership is defined by New York State Social Services Law, which requires the participation of
certain agencies as well as allowing for the appointment of professionals from various fields of practice.
The multidisciplinary approach is an effective strategy to study the issues related to child death and to
move toward solutions. Each case can be reviewed from various perspectives and the collective
expertise of the Team can engage policy and practice reform. The BC CFRT enjoys membership from
community leaders in medicine, law enforcement, child welfare, public health, and behavioral health.
Team members include representation from the following agencies:
Broome County Health Department: Director of Public Health, Director of Maternal Child Health &
Development, Medical Director, Professor, Emeritus
Broome County Attorney’s Office: Deputy County Attorney, Coroner
Broome County District Attorney’s Office: District Attorney
Broome County Mental Health: Commissioner, Program Coordinator
Broome County Office of Emergency Services: Emergency Medical Services Coordinator
Broome County Office of the Sheriff: Sheriff, Detective Sergeant
Broome County Social Services: Commissioner, Director of Child Protective Services
Family Violence Prevention Council: Coordinator
Lourdes Hospital: Forensic Pathologist, Practice Manager
Mothers & Babies Perinatal Network: Executive Director
New York State Office of Children & Family Services: Designated Representatives
New York State Police: Sr. Investigator, Kirkwood; Lieutenant, Sidney
United Health Services Hospital: Neonatologist, Addiction Medicine Specialist, Pathologist
The BC CFRT has been reviewing cases on a monthly basis since March of 2009. Meetings are highly
confidential as dictated by statute and thus are closed to the public. A protocol and procedure manual
was developed by the Team in 2008 and has been renewed in accordance with New York State Social
Services Law and the rules and regulations promulgated by the New York State Office of Children and
Family Services.
Between March 2009 and December 2018, the Team conducted an in-depth review of 104 cases
involving children who died during the years 2007-2018. This summary report provides information
regarding the more general findings of this review process and the Team’s recommendations related to
those findings.
Child Death in Broome County
An important facet to understanding child death is to examine mortality data over a period of time.
Since BC CFRT does not review the death of every child, the following data serves as a point of reference
for the work of the Team. Table 1 presents data related to the total number of Broome County children
who died between the ages of 0-19, and of those children, the total number of infants. It should be
noted, as Table 1 illustrates, about 61 percent of all child deaths in Broome County (2006-2016) involve
infants under the age of one. Additionally, although the number of child deaths in Broome County
account for a very small percentage of the overall number of child deaths in New York State, the number
of children who have died in New York State has been on a steady decline since 2006.

Broome County
Community Health Assessment 2019-2024 117
Table 1
7
Year of
Death
Total # of
Child Deaths
Broome
Aged 0-19
Total Number
of Infants
8
Total Number
of Children
Aged >1
Total # of Child
Deaths
NYS
Aged 0-19
2006
35
17
18
2,463
2007
35
24
11
2,426
2008
30
19
11
2,371
2009
31
26
5
2,309
2010
16
9
7
2,157
2011
21
14
7
2,138
2012
27
11
16
2,046
2013
17
11
6
1,984
2014
18
12
6
1,887
2015
20
13
7
1,875
2016
23
10
13
1,844
Total
273
166
107
Closer examination of infant death data provides further definition as to the age of infants at the time of
their death. Table 2 presents data on infant mortality within Broome County for the years 2006–2016.
Included in Table 2 are infant death rate, defined as deaths under the age of 1 year per 1,000 live births;
neonatal death rate defined as deaths less than 28 days of age per 1,000 live births; and post neonatal
death rate defined as age 28 days and older but less than 1 year per 1,000 live births. It is important to
note that of the 166 infant deaths during this 10 year time period, 117 involved the death of an infant
under the age of 28 days, underscoring the vulnerability of the neonatal period. Deaths in the neonatal
period are often due to conditions of being born premature or congenital defects. Similar to Broome, a
condition in the perinatal period is the leading cause of death for infants across New York State (2005-
2014).
9
7
Source: Vital Statistics of New York State, New York State Department of Health
8
Infant is defined as less than one year of age.
9
NYS Department of Health, Leading Causes of Death, Infant Mortality, New York State, 2005-2014. Retrieved on
1/19/2017 from https://www.health.ny.gov/statistics/leadingcauses_death/gender/nys_infants_by_year

Broome County
118 Community Health Assessment 2019-2024
Table 2
# Infant
Deaths
< 1 year
Infant Death
Rate
# Neonatal
Deaths
< 28 days
Neonatal
Death
Rate
# Post
Neonatal
Deaths
28 days - < 1
year
Post
Neonatal
Death Rate
2006
17
8.0 (5.5)
11
5.2 (3.8)
6
2.8 (1.7)
2007
24
11.3 (5.9)
18
8.5 (4.0)
6
2.8 (1.8)
2008
19
9.2 (5.8)
15
7.2 (4.0)
4
1.9 (1.8)
2009
26
12.6 (5.6)
18
8.7 (4.0)
8
3.9 (1.7)
2010
9
4.4 (5.6)
5
2.4 (4.1)
4
2.0 (1.5)
2011
14
6.8 (5.6)
11
5.4 (4.1)
3
1.5 (1.5)
2012
11
5.3 (5.4)
7
3.4 (3.7)
4
1.9 (1.7)
2013
11
5.3 (5.5)
8
3.9 (4.0)
3
1.5 (1.5)
2014
12
5.7 (5.1)
8
3.8 (3.8)
4
1.9 (1.3)
2015
13
6.6 (5.0)
9
4.6 (3.4)
4
2.0 (1.6)
2016
10
5.0 (5.1)
7
3.5 (3.5)
3
1.5 (1.6)
Total
166
117
49
* Numbers in ( ) reference values in the Upstate Region.
Demographics of Cases Reviewed by the BC CFRT
As noted above, the BC CFRT does not review all child deaths. The Team does not review the deaths of
newborns who die as the result of prematurity or congenital conditions, unless such deaths fall under
SSL §20. As a result, approximately 10 cases are reviewed each year. This report details the findings of a
total of 104 cases which were reviewed from March, 2009 – December, 2018. Table #3 presents data
about the number of cases reviewed by year of death.
Table 3
0
5
10
15
20
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018
Cases Reviewed by Year of Death
N=104
Number of Cases Reviewed N=104

Broome County
Community Health Assessment 2019-2024 119
Table 4 lists the age of the children at the time of their death. It is important to note approximately 50
percent of the cases reviewed involved infants under the age of one. All 48 infant deaths reviewed
involved babies for whom death was unexpected or unexplained.
Table 4
Additionally, 59 cases involved males and 45 involved females. The racial categories are those identified
on the New York State Death Certificate; however, due to the low numbers of those children in the non-
White categories, they are presented here as non-White to protect confidentiality. Of the 104 cases
reviewed, 86 children were White and 18 were non-White.
Manner and Cause of Death
All death certificates involve a determination of the manner of death, as well as the cause of death. The
manner of death is characterized into different categories: natural, accident, homicide, suicide, or
undetermined/pending. The cause of death relates specifically to a physical condition that led to an
individual’s death. Deaths in New York State are certified by physicians, coroners, or medical examiners.
State law was recently amended to also include licensed nurse practitioners. Most of the deaths that
come under the purview of the BC CFRT were certified by a Broome County coroner. All four coroners in
Broome County are medical providers, as dictated by Broome County’s Charter. Several BC CFRT cases
were certified by the Onondaga County Medical Examiner’s Office and several were certified by an
attending physician.
0
2
4
6
8
10
12
14
16
18
20
22
24
26
28
30
32
34
36
38
40
42
44
46
48
50
52
< age 1 1-4 5-9 10-14 15-17
Cases Reviewed by Age
N=104
Number of Cases Reviewed N=104

Broome County
120 Community Health Assessment 2019-2024
Certifying death is a complex process that generally involves an autopsy, a death scene investigation if
relevant, and a review of the decedent’s medical records. Autopsies are performed by physicians who
are specially trained as general pathologists, pediatric pathologists, or forensic pathologists. Table 5
presents the BC CFRT cases by manner of death as determined by the death certificate. Categories are
condensed to protect confidentiality. Further detail regarding the cause of the death is not provided in
this document in order to protect individual confidentiality.
Table 5: Deaths 2007-2018: Children aged 0-17
Natural Deaths: Twenty-five percent of cases were determined to be natural deaths. Some of these
cases involved acute illnesses or conditions suffered by children with chronic medical concerns, whereas
other cases involved an undiagnosed congenital condition or an illness of unknown origin. A few cases
were certified as Sudden Infant Death Syndrome (SIDS).
Accident: A significant number of deaths (49%), were certified as accidental deaths. These cases
involved accidental asphyxiation, drowning, allergic reactions, smoke inhalation, injuries due to a fall,
prescription drug overdose, and transportation-related deaths.
Homicide/Suicide/Undetermined: As noted above, these categories were condensed for confidentiality
and represent twenty-six percent of the deaths reviewed. The cases deemed undetermined involved a
manner of death that could not be firmly established by the coroner or the pathologist after an
investigation was completed.
It is important to note, the BC CFRT process resulted in the recommendation that two death certificates
be changed. The recommendations were considered and, in one instance, the death certificate was
changed to reflect Team findings.
25%
49%
26%
Number of Cases Reviewed N=104
Natural (26)
Accident (51)
Homicide/Suicide/
Undetermined (27)

Broome County
Community Health Assessment 2019-2024 121
Findings and Recommendations
The BC CFRT reviews cases individually in a manner
that is as comprehensive as possible. As referenced
above, priority is given to review cases with DSS
involvement. There were no cases where DSS or any
other local agency involvement could have prevented
any of the 104 cases reviewed. DSS consistently
conducted thorough investigations; appropriately
provided protection for surviving children, when
necessary; and provided families with significant
services and referrals.
The following findings presented in this report
represent the major themes that have emerged from
reviewing cases over the course of several years. The
BC CFRT is most concerned with identifying patterns
of risk that exist in the community, which, if changed,
could result in preventing some child deaths in the
future. It is important to note that it is not possible to
prevent all deaths from occurring; however, much has
been learned about child health and safety by
examining the risk factors that exist in child fatalities.
The Team offers the following findings with corresponding community recommendations.
Finding #1: Infant Sleep Environment – Safe Sleep Practices
There has been much discussion in
recent years about the role of safe
sleep practices in reducing sudden
infant death. As has been found by
child fatality review teams around the
country, the BC CFRT found that sleep
environment is a very important
element to be considered in
understanding how and why some
infants die. This report provides the
opportunity to re-iterate the
importance of the infant sleep environment.
The Team recommends caregivers follow the recommendations provided by the American Academy of
Pediatrics
10
. Infants should be placed alone, on their back, in an empty crib. The crib should meet
10
American Academy of Pediatrics, Retrieved 1/23/17 from
http://pediatrics.aappublications.org/content/early/2016/10/20/peds.2016-2938

Broome County
122 Community Health Assessment 2019-2024
current safety standards and have a firm mattress sized appropriately for the crib, with a tight fitting
sheet. The crib should be free from bumper pads, pillows, blankets, stuffed animals, etc. Additionally,
newborns can benefit by being in close proximity to their parents; if possible, the crib should be
positioned in the same room as the parents. Room-sharing can facilitate breastfeeding and bonding.
Furthermore, infants should not be over-heated.
Of the 104 cases reviewed by the BC CFRT, regardless of death certification, the Team determined 35
cases involved hazardous sleep environments. Hazardous sleep environments involve infants placed to
sleep in environments that place them at significant risk of suffocation or asphyxiation. Such
environments include the presence of pillows, cushions, blankets, comforters, stuffed animals, pets,
siblings, and include instances in which a child is placed to sleep on their stomach. In addition, infants
are at risk when placed to sleep in products not meant for such purpose (such as a couch, chair, boppy
pillow or car seat), when an infant’s size has exceeded the limit set for product safety, or if the product
has not been assembled properly.
Most notable, in 18 cases an infant was co-sleeping with or sharing a sleep surface with at least one
adult. At some point during the sleep episode the adult(s) and/or the bedding created a situation in
which the infant was asphyxiated or suffocated. Co-sleeping between an infant and other individuals or
pets is dangerous. All of these co-sleeping deaths may have been preventable.
As a result of BC CFRT’s above findings that unsafe sleep caused children’s deaths, the BC CFRT reviewed
various educational opportunities parents and caregivers have to learn about safe sleep within our
Broome County community. The BC CFRT determined the safe sleep message is routinely given at local
hospitals, through family care and pediatric physicians, and community agencies. To strengthen this
important message, the Team sponsored a television commercial, purchased educational materials, and
Team members participated in several local news reports. Further, organizations such as Mothers and
Babies Perinatal Network, Broome County’s Health Department and Family Violence Prevention Council
reaffirmed their commitment to continue to educate our community about the importance of safe
sleep.
The BC CFRT recommends the community continue to invest in educating all types of caregivers
regarding safe sleep of infants, including; parents, grandparents, intimate partners, daycare providers,
and babysitters. The community should also continue to invest in the training of professionals, such as
health care professionals and others who work with families. Safe sleep recommendations and
resources are available from the NYS Department of Health and the National Institutes of Health.
Finding #2: Substance Use/Abuse
Another finding of the BC CFRT, in reviewing deaths that occurred 2007-2018, is the relationship
between use of substances and child death. To maintain compliance with state and federal privacy laws
numbers will not be disclosed. In several cases, use of prescription drugs, alcohol, or illicit drugs by a
primary caretaker was determined to be a contributing factor in the events that led to a child’s death. In
other cases, impairment of a caretaker was suspected. Tragically, several children died as a result of
accidental prescription drug poisoning/overdose.

Broome County
Community Health Assessment 2019-2024 123
The BC CFRT found the prescription of opiate drugs the most problematic. The following community
recommendations are made:
Caretakers be better advised by their physicians and pharmacists about the impact various
prescriptions may have on their ability to properly attend to and supervise young children.
Drivers should be advised by their physicians and pharmacists about the impact various
medications may have on their ability to drive and respond to dangers on the road.
All prescription drugs and over-the-counter drugs should be kept out of the reach of children,
and certain drugs should be kept in a locked box.
As improper disposal of prescription medication can give children inadvertent access to
medication, it is important consumers are aware of proper disposal methods for various
prescription medications.
Increase the number of opportunities and continue to emphasize the availability for unused
pharmaceuticals to be properly disposed of within the drop off disposal program provided by
the Broome County Sheriff’s Office.
It should also be noted, many children whose cases were reviewed were exposed to secondhand
tobacco smoke, although such exposure was not directly linked to their death. Secondhand smoke
exposure is a concern for the overall health and well-being of children and is well established in research
literature as a risk factor specifically related to Sudden Unexpected Infant Death. The risk for Sudden
Unexpected Infant Death increases for babies whose mothers smoked while they were pregnant and for
those infants exposed after birth. Chemicals in secondhand smoke appear to affect an infant’s brain in
ways that interfere with the regulation of breathing. In fact, the Surgeon General has concluded that
there is no risk-free level of exposure to secondhand smoke for children, as even brief exposure can be
harmful.
11
Finding #3: Consumer Product Safety
Several cases reviewed by the Team involved use/misuse of a consumer product. To maintain
compliance with state and federal privacy laws numbers will not be disclosed. The Team concluded the
community would greatly benefit from a heightened awareness of possible dangers that could exist in
consumer products, particularly those designed for young children. The following recommendations are
made:
Promote community notification of recalled child products.
Consumers should not modify products from their original design.
Consumers/caretakers should use products as they are recommended by the manufacturer.
Since there is no way to assure that second-hand products meet current safety standards, it is
recommended that caregivers not use products which are second-hand, found, or of unknown
11
U.S. Department of Health and Human Services. 2006, The Health Consequences of Involuntary Exposure to
Tobacco Smoke: A Report of the Surgeon General. Atlanta: U.S. Department of Health and Human Services,
Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic
Disease Prevention and Health Promotion, Office on Smoking and Health. Retrieved 12/28/12.

Broome County
124 Community Health Assessment 2019-2024
history. It is important that all products be assembled with proper parts as directed by
manufacturer instruction.
Encourage consumers to maintain a file for instructions on the products they purchase ….with
particular attention paid to when they should stop using the product because of weight/age
restrictions. Consumers should flag dates to periodically read instructions. Store these essential
documents for use with future children.
Educate consumers that just because a product is sold in the store it does not mean it is safe or
necessary. For instance, crib bumper pads are NOT NECESSARY, yet do present a potential
hazard. The American Academy of Pediatrics states, “Bumper pads should not be used in cribs.
There is no evidence that bumper pads prevent injuries, and there is a potential risk of
suffocation, strangulation or entrapment.”
12
When shopping for products for babies or children,
consumers should carefully inspect products for potential hazards, even if product has not been
recalled.
Children should be supervised when using products/toys.
Finding #4: Reduce Risk - Use Well Established Safety Devices/Procedures
Many deaths reviewed by the Team were deemed preventable. The review process identified issues
regarding child health and safety that could apply to the broader community, even if a particular child’s
death could not reasonably have been prevented. Children’s health and safety can be maximized by
utilizing devices or processes and procedures intended to protect the health and safety of children.
Examples include:
Caretakers should have a general understanding of the various developmental milestones of
babies and young children. Knowledge of children’s developmental ability will enable caretakers
to adhere to safety guidelines appropriate for the age of the child.
Proper adult supervision is critical to children’s health and safety.
Use smoke and carbon monoxide detectors. Ensure batteries are routinely changed.
Pools and other bodies of water should be fenced off and locked. Avoid leaving open
containers full of liquid, such as pails and buckets. Children should always be supervised
around bodies of water.
Prevent fatal automobile accidents; use booster seats, car seats, and seat belts in the
appropriate manner based on weight and age of the child.
Baby monitors can alert caretakers that a baby is having difficulty during sleep; however,
monitors need to be placed in a safe location away from the baby as the electrical cord can
cause hazards.
Medications should be disposed of and stored properly. Medications must be kept out of
reach of children. Some medications may be better stored in a locked box.
Window locks/guards should be used to prevent fatal falls. Window treatments should be free
of dangling cords.
Practice gun safety/keep guns and ammunition locked.
12
American Academy of Pediatrics. Retrieved on 3/18/13 from http://www.aap.org/en-us/about-the-aap/aap-
press-room/pages/AAP-Expands-Guidelines-for-Infant-Sleep-Safety-and-SIDS-Risk-Reduction.aspx.

Broome County
Community Health Assessment 2019-2024 125
Children should be breast-fed as it is associated with a reduced risk of Sudden Infant Death
Syndrome. Breastfeeding improves mother-child bonding and promotes positive health,
psycho-social, economic, and environmental effects.
13
Promote preventive healthcare: prenatal care; pediatric health, dental, and vision care.
Promote immunizations.
Team Accomplishments
The BC CFRT, in partnership with other local organizations and agencies, accomplished a number of
important endeavors since its 2008 inception. These achievements are a reflection of the work of a
dedicated group of professionals in Broome County who care very deeply about the well-being of our
children. The following summarizes some of the more significant accomplishments and outcomes of the
BC CFRT process.
Professional Education: The BC CFRT sponsored two trainings for law enforcement and child
protective workers regarding infant death investigation. Team members also participated in a
number of trainings involving a wide range of topics that relate to child health/safety and child
death investigation.
Safe Sleep Message Strengthened: Two newspaper articles were published to address the issue
and the Team sponsored a television commercial. The Team corresponded with national
media/corporations to reinforce the safe sleep message. The Team also partnered with other
organizations to assist in purchasing educational materials for community distribution.
Community partners continue to strengthen the safe sleep message and participate in the Cribs
for Kids program.
Consumer Product Safety: Five reports involving questionable products were made to the
Consumer Product Safety Commission.
Traffic Safety: Transportation officials installed new signs on a busy road to warn drivers of a
potential safety concern after the Team recommended officials’ review the roadway following a
fatality.
Child Abuse Prevention: In partnership with Broome County’s Family Violence Prevention
Council, the Team supported the “Choose your Partner Wisely” prevention campaign.
Prescription Drug Safety: In partnership with Broome County Sheriff’s Office, additional “drug
drop off” sites were added in the county.
Professional Development: The BC CFRT process has been instrumental in increasing our
understanding of how and why children die. Each of the professionals involved has developed
many new insights that can improve their own professional practice and knowledge base across
multiple disciplines.
Building a Library: The Team is staying updated on recent research related to child death.
Improved Process/Communication: The BC CFRT also acknowledges improvements have been
made in the death investigation and certification process as well as improved communication
between agencies as a result of the review process.
13
U.S. Department of Health and Human Services. The Surgeon General’s Call to Action to Support Breastfeeding.
Washington, DC: U.S. Department of Health and Human Services, Office of the Surgeon General; 2011. This
publication is available at http://www.surgeongeneral.gov.

Broome County
126 Community Health Assessment 2019-2024
Coordinating with other coaltions/planning bodies: The BC CFRT members also collatorate on a
number of other initiatives in the community; such as, Broome Opioid Abuse Council (BOAC),
Family Violence Prevention Council, and Multi-Disciplinary Team (MDT).
Broome’s Child Fatality Review Team used as Model: Upon recommendation of State officials
and other professionals, child fatality review team members from other communities and
communities without review teams have observed Team meetings to determine how their
community may benefit from Broome’s experience.
Conclusion
This Community Report summarizes the general themes of the findings of the Broome County Child
Fatality Review Team from the 104 cases reviewed to date between March 2009 and December 2018.
This work would not be possible without funding from the New York State Office of Children and Family
Services. The members of the Broome County Child Fatality Review Team greatly appreciate the New
York State funding which enables this review process. Our reviews over the past ten years have
provided great insight into the causes of child (and infant) death in our county resulting in insightful
recommendations for – and actual implementation of – community awareness/education campaigns
and new community resources (such as the Cribs for Kids program), advanced education and training for
various emergency responders and medical personnel, improved safety measures and greater
communication and coordination among local providers. Additionally, we hope that our “extra steps” to
communicate with manufacturers whose products have resulted in infant/child injury and death will
ideally be used for product modification to prevent other injury and death. The value of the CFRT
program is significant both for all local communities conducting such reviews and New York State
overall.

Broome County
Community Health Assessment 2019-2024 127
Section Three — Problems and Issues in the
Community
A. Profile of Community Resources
The following list of community resources is inclusive but by no means exhaustive of the many health-
related services available in Broome County. Much of the information about the agencies listed here
was gathered from a combination of community resource guides including United Way’s First Call for
Help Directory, the United Way’s Broome County Family and Youth Services Guide, and the Broome
County Elder Services Guide published by Actions for Older Persons. Additionally, these agencies and
others that provide community services and resources can be found online at their respective websites.
A directory of non-profit community agencies and services can be found online at:
http://www.unitedwaybroome.org/ Detailed information about these agencies can be found in
Appendix G1 and includes the name of the service provider, the target population served, and a brief
description of services provided.
Broome County is known among area providers as a “resource rich” community. There are a large
number of health and human service programs and agencies that share a common goal of improving the
health status of area residents in different ways, yet each has their own specific mission, objectives, and
target population.
There have been significant efforts at the county level to develop an integrated planning approach to
services. Broome County’s Integrated County Planning (ICP) Committee represents a customer-oriented
system for delivering human services that builds on community and individual strengths and relies on
standards, best practices, and outcomes that are valid and measurable. It seeks to accomplish this by
combining several existing planning processes into a more streamlined and understandable process that
guides the allocation and management of resources. The purpose of this approach is to foster
collaboration among community organizations and minimize or eliminate duplication and maximize
effective use of resources. This approach also assists department heads in health and human services to
be aware of resources allocations for specific population groups and concerns. An online, web-based
process for community agencies to request letters of support from county departments has streamlined
communication among agencies applying for grant funding.
Assessment of Services
As part of the Community Health Assessment process, an extensive list of community resources was
compiled. This “Resource Guide” appears in Appendix G and will also be published separately on the
Broome County website along with the 2019-2024 Community Health Assessment (CHA), the 2019-2024
Community Health Improvement Plan (CHIP), and all supporting Appendices. This Resource Guide
contains information about location, hours of operation, and social media presence for community
agencies and is topically organized for ease in locating a service provider. The following sections provide
details on many of these agencies, the services that they provide, and their current capacity for
addressing the health needs of our community.

Broome County
128 Community Health Assessment 2019-2024
B. Access to Care
Hospitals
Broome County has two major hospital systems operating within its geographic boundaries: Our Lady of
Lourdes Memorial Hospital (Lourdes) and United Health Services (UHS) Hospitals. The Lourdes system
has one acute care facility with 242 licensed beds and UHS has two acute care facilities, Wilson Medical
Center (Wilson) which has 280 licensed beds and Binghamton General Hospital (BGH) with 220 licensed
beds (Table 34). Both health care systems are well known and respected in the community. Both
systems have multiple programs including community outreach education as well as primary care sites.
Their primary service areas include Broome, Chemung, Chenango, Cortland, Delaware, and Tioga
Counties, though each draws from different zip codes within the local area.
Lourdes is part of Ascension Health, which is a Catholic not-for-profit system and has a main hospital
campus that includes a hospice program, regional cancer center, breast care center, and ambulatory
surgery center. Lourdes is designated as a Level 1 Perinatal Center, Primary Stroke Center, and is one of
forty-three Sexual Assault Forensic Examiner (SAFE)-Designated hospitals in NYS that provides
specialized care to sexual assault patients.
United Health Services (UHS) is a locally owned, not-for-profit healthcare system governed by an all-
volunteer Board of Directors, which includes community residents. UHS operates four hospitals, two of
which are located in Broome County – Wilson Medical Center and Binghamton General. Wilson Medical
Center is a university affiliated teaching hospital and a Level II Adult Trauma Center with Life Flight
capability that serves as the Regional Trauma Center for South Central New York State and Northern
Pennsylvania. In addition, this facility is a state-designated Primary Stroke Center and offers state-of-
the-art stereotactic radiosurgery at their Cyberknife Center of New York. The hospital is also designated
by NYS as a Level 3 Perinatal Center. Binghamton General provides certified mental health services
which includes rehabilitation for chemical dependence and withdrawal as well as a comprehensive
psychiatric emergency program.
In conjunction with the Community Health Assessment, the area hospitals completed their Community
Service Plans (CSPs). The 2019 Community Service Plans provide details on the major health systems’
efforts and progress toward addressing the priorities identified by the 2019-2024 Community Health
Assessment. The CSPS will be published online at the following addresses:
The Community Service Plan for United Health Services Hospitals will be published to the
following web address: https://www.nyuhs.org/about-us/community-service-reports/
The Community Service Plan for Ascension Our lady of Lourdes Memorial Hospital will be
published to the following web address: https://healthcare.ascension.org/CHNA

Broome County
Community Health Assessment 2019-2024 129
Table 34. Area Hospitals - Licensed Number to Operate and Type of Beds, Broome County, NY
Care Unit
Binghamton General
Lourdes
Wilson Medical Center
Coronary Care
16
Intensive Care
8
12
12
Maternity
25
34
Medical-Surgical
86
194
190
Neonatal Continuing Care
2
Neonatal Intensive Care
6
Neonatal Intermediate Care
6
Pediatric
11
14
Chemical Dependence - Rehabilitation
20
Coma Recovery
1
Transitional Care
20
Physical Medicine/Rehabilitation
24
Psychiatric/Mental
56
Trauma Brain Injury
5
Total
220
242
280
Primary Care & Other Healthcare Services
The list of area primary care centers appears in Appendix G2 and map of locations in Appendix G9. The
catchment area served by both health care systems extends beyond Broome County into Tioga and
surrounding counties. Lourdes operates eighteen primary care offices, eight of which are located in
Broome County including four in Binghamton, two in Vestal, and one in each of Endicott and Whitney
Point. Of these locations, three provide care to pediatric clients including one specifically for
endocrinology (Appendix G3). In addition, Lourdes operates three walk-in clinics in Broome County, two
located in Binghamton and one in Endicott (Appendix G5). UHS operates 10 primary care offices in
Broome County: four are in Binghamton and one each located in Deposit, Endicott, Endwell, Johnson
City, Vestal and Windsor. Of these locations, three provide care to pediatric clients with two locations in
Binghamton and one in Vestal (Appendix G3). In addition, UHS operates four walk-in clinics in Broome
County located in Binghamton, Chenango Bridge, Endicott, and Vestal (Appendix G5). UHS also
maintains two school-based health centers in two high-need elementary schools (Appendix G6).
Specialty services in Broome County are available through both Lourdes and United Health Services. The
medical staffs of the system's four hospitals in Broome, Chenango and Delaware counties include more
than 500 doctors representing a wide range of medical specialties and primary care options.
One additional healthcare system with regional operations in Tioga County and Northeastern
Pennsylvania, Guthrie Medical, operates a clinic in Vestal. This clinic provides family care services and
other specialty services including ophthalmology, endocrinology, audiology, cardiology, optometry, and
urology. This location is one of the primary practice sites responsible for out-migration of health care
services from the county, as patients from this practice generally are referred to Robert-Packer Hospital
in Sayre, Pennsylvania.

Broome County
130 Community Health Assessment 2019-2024
Cornerstone Family Healthcare Federally Qualified Health Center
Cornerstone Family Healthcare (Cornerstone) is a non-profit Federally Qualified Health Center with a
mission to provide high quality, comprehensive, primary and preventative health care services
(Appendix G4). Cornerstone operates 18 locations in Orange, Rockland, and Ulster counties in NY and
Pike County in PA as well as one site in Broome County. Cornerstone has over six hundred employees
including more than 50 Board Certified/Board Eligible physicians, dentists, nurse practitioners,
physician’s assistants, dentists, social work and counseling staff who provide care to more than 40,000
individuals and families annually. A Registered Dietitian and Certified Nutritionist is on staff 5 days a
week and is an integral part of the patient care team, and works one-on-one with patients providing
nutrition and weight loss counseling and chronic disease management. Cornerstone also provides
wellness programs, educational health talks and support groups, chronic disease management services,
health assessments, clinical screening, and health coaching around the topic through a Certified Patient
Educator. Cornerstone also operates a fleet of mobile health and mobile dentristry units. Cornerstone is
nationally recognized as a Patient Centered Medical Home (PCMH) receives US Department of Health
and Human Services funding, and has Federal Public Health Service (PHS) deemed status.
Stay Healthy Center
UHS Hospitals operates the Stay Healthy Center for Community Health located at the Oakdale Mall in
Johnson City to assist area residents with health education needs and referrals to health care services.
This center also collaborates with numerous community agencies and promotes healthy lifestyles. The
Center is open to the public 9 am to 5 pm Monday through Friday and is closed on Saturdays and
Sundays. They offer access to computers for people to perform literature searches on health topics,
have a lending health library, and have a Senior Security program that works with older individuals and
groups.
The staff at Stay Healthy offers several programs and services to individuals, schools and businesses.
These programs are designed to improve the health of the community and include many partnerships
with local organizations. The center also provides insurance counseling. In addition, community groups
in need of speakers with expertise in specific health-related areas can access this resource through the
center. Programs are available for asthma, eating disorders, healthy living, cancer, and tobacco
cessation among others. Services offered include lactation consultants to work with new mothers, child
birth and parenting classes, Care-A-Van shuttle service, Stay Healthy Seniors and Stay Healthy Kids.
The Stay Healthy Center includes a Nurse Direct call center. This call center allows anyone to call in and
talk to a nurse. Callers can request information about UHS programs or ask a health question. This
service can be accessed either by phone or online. The center is staffed with nurses from 7 am to 9 pm,
seven days a week and provides computer assisted: physician referral service, referral triage using
nationally developed and locally reviewed guidelines, and health information for disease management
of asthma, diabetes, and congestive heart failure as well as smoking cessation, weight management, and
prenatal care. In addition to information, the registered nurses at Nurse Direct can provide referrals to
other health education and community services.

Broome County
Community Health Assessment 2019-2024 131
Mission in Motion
In addition to services offered through primary care office sites, Lourdes provides services through two
mobile medical van units through its Mission in Motion program. Both mobile medical unit vans make
health care accessible by providing primary care and cancer screening services to those in underserved
and rural areas in the Southern Tier. One medical unit, the Mobile Mammography van, is a member of
the Cancer Services program funded by NYS and provides no cost/low cost mammograms, pelvic exams,
and Pap tests. This van also provides health care services for women including breast exams, digital
mammography screenings, routine gynecological screenings, and education. The other mobile van, a
primary care medical unit, is used for general wellness and health screenings throughout the area, as
well as a wide variety of occupational health service screenings. It offers a wide range of health care
services to the public including: cancer screenings, health promotion, disease prevention, education and
information, physical exams, occupational health testing, and cholesterol testing. Both mobile units
travel to a wide variety of community sites such as churches, schools, senior centers, and worksites.
Center for Oral Health
In January 2005, in response to a long standing need for dental care in the community, Lourdes opened
a dental clinic, entitled the Center for Oral Health. This center was opened in order to provide increased
access to dental services for children who are uninsured, on Medicaid, or on NY Child’s Health Plus
program, a population that is underserved for dental services in the Broome County area. The initial
start-up grant application was submitted jointly by Lourdes Hospital and the Broome County Health
Department to the NYS Department of Health’s Dental Bureau. This effort was also supported by UHS
Hospitals, who felt the need far exceeded current capacity to serve the dental needs of low income
children and their families. Services are provided by dentists and registered dental hygienists through
the Center for Oral Health include routine cleanings, patient education, fluoride treatments, sealants, x-
rays, urgent care, filings, and extractions. All services offered at the Center of Oral Health are available
on the Lourdes Mobile Dental Clinic and all children at participating schools are eligible to receive a free
dental education, screening, and a parent report to bring home. These services, in turn, are coordinated
with the Broome County Health Department, which has a long-standing dental sealant program in area
schools, so that services are maximized and not duplicated. Lourdes also offers a Patient Financial
Assistance Program to help patients who meet specific guidelines and who are not eligible for any other
available program. The Center for Oral Health is conveniently located in Binghamton, next door to the
Broome County Health Department.
UHS Dental Clinic
Supported by UHS Hospitals, UHS also has a fully operating dental clinic located within Binghamton
General Hospital. The clinic provides care for all ages, from children to the elderly and offers many
treatment options, such as anesthesia or sedation, for patients with special needs, or for those who
have sever handicap limitations or who are compromised medically. Additionally, the clinic provides
patient screenings for oral cancer and treatment for patients undergoing radiation or chemotherapy for
head or neck cancer. It also provides education about oral hygiene, complete examinations, X-rays,

Broome County
132 Community Health Assessment 2019-2024
cleanings, fluoride treatments, fillings, fittings of crowns, bridges and dentures, and extractions and
minor oral surgery. Dental services are offered on a sliding fee scale that covers between 20-60% off a
patient’s bill if they qualify for financial assistance. The clinic is open five days per week by appointment
for patient dental care.
Broome County Mental Health Department
The Broome County Mental Health Department is responsible for planning, developing, and evaluating
mental hygiene services in Broome County. These mental hygiene services include alcoholism and
substance abuse services, mental health programs, and services for mentally retarded and developmentally
disabled citizens. Beyond its regulatory role as the local governmental unit, the Department of Mental
Health is also licensed to operate mental health and chemical dependency programs.
The Broome County Department of Mental Health directly operates both mental health and chemical
dependency programs. These programs include outpatient programs for adults, adolescents and children.
The New York State Office of Mental Health (OMH) licenses the mental health programs. The New York
State Office of Alcoholism and Substance Abuse Services (OASAS) licenses the addiction programs.
Three subcommittees advise the Mental Health Commissioner: Mental Health Subcommittee,
Alcoholism/Substance Abuse Subcommittee, and the Mental Retardation/Developmental Disabilities
Subcommittee. A number of programs operate in each of these three areas such as adult clinic, child and
adolescent clinic, chemical dependency services unit, and the Keep Youth Drug-free and Safe Coalition
among others. In addition to its operations in the three service areas, the Broome County Department of
Mental Health has established contracts with a number of area private, not-for-profit agencies including
Catholic Charities of Broome County, Fairview Recovery Services, Family & Children’s Society, Our Lady
of Lourdes Memorial Hospital, and the Mental Health Association of the Southern Tier.
Emergency Medical Services
Emergency medical services (EMS) are provided by Broome County as well as private emergency squads.
The emergency response provided by the county is a separate department under county government.
Emergency medical response for Broome County is provided by a combination of ambulance services
and non-transporting first response services (Appendix G7-G9). These responders are the physical link
between local hospitals and the geographic townships and serve as the “ultimate safety net.”
Unfortunately, there is no level of government that is responsible for providing EMS to all municipalities.
The success of EMS in the county is tenuously sustained by the support and cooperation of many
community agencies and volunteers. The EMS leadership in the county strives to ensure the availability
of emergency services through recruitment, education, training, and mentoring of EMS personnel.
Despite the fact that communities are not required to have or support EMS, most have some form of
volunteer service agency. In addition to their critical emergency response role, EMS often provide
education and outreach to community members teaching them about recognition of heart attack and
stroke symptoms and when to activate EMS.

Broome County
Community Health Assessment 2019-2024 133
Long Term Care Facilities & Home Care Services
A total of eleven skilled nursing facilities are licensed to operate in Broome County; four are located in
Binghamton, two in Endicott, two in Johnson City, two in Vestal and one in Endicott. Willow Point is a
county facility and the only public option. Although occupancy rates vary, all but one of the facilities
have consistently been at or above 90%. While all provide baseline services, Elizabeth Church Manor and
James G. Johnston Memorial Nursing Home provide outpatient occupational, physical and speech
therapy. Ideal Senior Living Center offers a clinical laboratory and radiology diagnostics on site.
Susquehanna Nursing and Rehabilitation Center operates an Adult Medical Day Care on the premises.
Three of the nine facilities offer the provision for respite care while all nine are contracted to provide
hospice care through Hospice at Lourdes. An updated list of these facilities appears in Appendix G19.
Among these facilities, there are 1,832 skilled nursing beds, a 13% increase from 2013.
CHHAs provide part time, intermittent, skilled services including preventative, therapeutic,
rehabilitative, health guidance and/or supportive care to persons at home. Home health services include
nursing, home health aides, medical supplies, durable medical equipment and appliances as well as at
least one additional service that may include physical therapy, occupational therapy, speech pathology,
nutritional services, or medical social services. Services provided by CHHAs may be reimbursed by
Medicare, Medicaid, private payment, and commercial health insurers. In Broome County, there are
three Certified Home Care Agencies serving Medicare and Medicaid clients. All three agencies provide
similar services, with Lourdes at Home offering audiology and respiratory therapy. Client census rates
vary among the three.
In addition, there are 15 licensed home care services agencies: six are located in Binghamton, five in
Johnson City, two in Vestal, and two in Endicott. Six provide services exclusively in Broome County while
the remaining agencies service one or more counties in addition to Broome County. These facilities offer
home care services to clients who pay privately or have private insurance coverage. These agencies may
also contract to provide services to Medicare/Medicaid beneficiaries whose cases are managed by
another provider or entity, such as providing home health aide services to a certified home health
agency patient or providing a licensed practical nurse for a Medicaid prior-approved private duty nursing
shift.
Broome County has one freestanding hospice program operated by the Hospice at Lourdes. Hospice is a
program that provides care to terminally ill individuals focused on easing symptoms rather than treating
disease. The emphasis of the program is to help individuals remain at home for as long as possible. The
hospice program provides physical, psychological, social, and spiritual support and care for the patient
and their family. Services offered through hospice include nursing and physician services, medical social
services, counseling (including nutrition and bereavement counseling), and physical and occupational
therapy. In addition, hospice can provide home health aide and homemaker services, medical supplies
and appliances, speech therapy, and short-term inpatient care. Hospice is available through Medicaid,
Medicare, private payment and some health insurance carriers. Referrals to hospice may come from any
source, but must have physician certification that the patient has a terminal illness with a life expectancy
of fewer than six months.

Broome County
134 Community Health Assessment 2019-2024
Elder Care Programs & Services
A number of programs and services are available through the Broome County Office for Aging (Appendix
G22). These programs and services include: caregiver services, foster grandparent program, health and
wellness program, health insurance counseling, home delivered meals, home energy assistance, home
repair, in-home services (including homemaker, personal care, shopping, and emergency response
services for the home bound), resource assistance, legal services, and mental health services. In
addition, 10 senior sites off socialization, nutritious meals, and wellness activities. Transportation
services are also available. A list of apartment options for seniors and those with disabilities is provided
in Appendix G23.
Diagnostic and Treatment Centers
Diagnostic and Treatment Centers (Clinics) are free-standing clinics that are separately-owned and are
not operated by a hospital. By contrast, clinics that are owned and operated by a hospital are known as
Hospital Extension Clinics. These free-standing clinics include centers that are federally certified to
provide specialized services, such as surgery or dialysis. In Broome County, there is only one free-
standing Diagnostic Treatment Center, Bridgewater Center for Dialysis, which is located in Binghamton
and has a service capacity of 8 clients. There are three Diagnostic and Treatment Center Extension
Clinics that operate in Broome County, Vestal Healthcare (service capacity 24), LLC, Vestal Healthcare -
UHS Dialysis on Pennsylvania Ave (service capacity 15), and Vestal Healthcare - UHS Dialysis on Park
Avenue (service capacity 24). All four centers provide renal dialysis services for patients with end stage
renal disease (ESRD) with a combined total service capacity of 71 clients.
Healthcare Workforce
Physicians
Though not exhaustive of all practicing physicians in the county, 106 physicians from a broad range of
specialties are listed as members of the Broome County Medical Society as of December 2019. In 2016
the NYS Health Workforce Planning Data Guide (Appendix G10) noted 664 active patient care physicians
in the county 250 in primary care, 94 in general internal medicine, 36 in general pediatrics, 29 in general
surgery, and 25 in obstetrics/gynecology.
In The Southern Tier, which includes Broome, Chenango, Delaware, Tioga, and Tompkins counties, 50%
of physicians are age 50 or older. In 2016, just over 25% of physicians were female and only 3.5% were
from underrepresented minorities (URM) in the Southern Tier of NYS. Compared to 2013, there was a
small increase in the proportion of female physicians (up from 22%) but a large decrease in the
percentage of physicians from URMs (down from 6.1%). There is notably less diversity in the physician
workforce in the Southern Tier than NYS as a whole, which is 31.8% female and 10.6% underrepresented
minority. Compared to NYS, there is a larger proportion of physicians age 50 or older and a smaller
proportion that is female, and the physician workforce is less diverse.

Broome County
Community Health Assessment 2019-2024 135
Physician shortages for the area are captured in the Federal Health Professional Shortage Areas (HPSA).
Primary Care HPSAs are based on a physician to population ratio of 1:3,500 and does not take into
account the number of physician assistants or nurse practitioners. The Health Resources and Services
Administration data for HPSAs indicate a primary care shortage for the low-income population within
the county, and Broome County is designated as a Medicaid Eligible Population HPSA for mental health,
dental health, and primary care. The HPSA primary care designation for these areas represents service
needs for 67,691 residents or 34.1%% of the Broome County population (NYS Health Workforce
Planning Data Guide, 2016). These figures are a substantive increase (169%) from 2013 for which, there
were identified service needs for only 23,713 residents or 12.1% of the Broome County population (NYS
Health Workforce Planning Data Guide, 2013).
In addition, the University of the State of New York Regents report of Designated Physician Shortage
Areas (2013) identified the Deposit service area (including the towns of Colesville, Sanford, and Windsor)
and the Greater Binghamton service area (including the towns of Barker, Binghamton, Chenango,
Conklin, Dickinson, Fenton, Kirkwood, Lisle, Maine, Nanticoke, Triangle, Union, and Vestal as well as the
City of Binghamton) as Primary Care Regents Physician Shortage Areas. In addition, Broome County is
designated as a shortage area for primary care physicians and psychiatrists within the Developmental
Disabilities Services Office. In the category of non-primary care shortage areas, Broome County is
designated for preventive medicine. Both United Health Services hospitals are eligible under the Primary
Care and Non-Primary Care designations.
Like most of the health professions, physicians will be “aging out” in large numbers over the next
decade. Given the sizeable increase in HPSA service need over the past three years, the demand for
primary care services appears to exceeding the supply of primary care providers in Broome County.
Moreover, significant gaps have been noted by local health systems in specialty areas including
ophthalmology, urology, psychiatry, and pathology.
Nurses
Registered Nurses comprise the largest proportion of the healthcare sector workforce. The Center for
Health Workforce Studies (CHWS) reports there are 2,792 Registered Nurses (RNs), 745 Licensed
Practical Nurses (LPNs), and 210 Nurse Practitioners (NPs) in Broome County (Appendix G10). Across all
levels of preparation, the number of nurses was relatively unchanged from 2013.
Nurses staff hospitals, nursing homes, assisted living facilities, home care agencies, outpatient clinics,
primary care and specialty practices, health departments, and hospice programs. For the period 2008 to
2018, the US Bureau of Labor Statistics projected a 22% increase in employment for nurses adding
581,500 new RNs and 155,600 new LPNs to the workforce. In addition, 458,000 RNs and 80,100 LPNs
will be needed to replace nurses who are expected to retire or leave the field during this time period.
14
For New York State, the 2016 report by the CHWS examined the balance between supply and demand
for the registered nursing workforce. Their analysis concluded that there was currently a relative
balance that would likely be maintained over the next decade if current training and retirement patterns
14
The Center for Health Workforce Studies (2011). The health care workforce in New York, 2009: Trends in the
supply and demand for health workers. Albany, NY: Author.

Broome County
136 Community Health Assessment 2019-2024
remained stable. However, the report also indicated that small changes (as little as 10%) in entry into or
exit from the profession or a 2-year change in retirement could significantly alter their projection.
15
Furthermore, recent practice patterns indicate that nursing positions are shifting from the traditional
hospital setting to home health, ambulatory care, and nursing homes. Current workforce models
provide varying estimates and many factors contribute to supply and demand.
16
On the demand side,
the aging population and increasing prevalence of chronic diseases such as diabetes contribute to the
expected need for more healthcare workers. Economic factors and healthcare policy changes are more
difficult to predict. The Affordable Care Act and Medicaid Redesign as well as policy recommendations
of the Institute of Medicine
17
are likely to increase demand while education cycles, training capacity, and
faculty shortages are likely to limit supply. Overall, the net effect nationally is long-term projected
shortages in the nursing workforce.
Between 2016 and 2026, employment in healthcare is predicted to grow faster than other sectors of the
economy, and within the healthcare sector, employment is expected to grow most rapidly for home
health care and in provider practices, whereas hospital employment is projected to be less robust
(Figure 18). In fact, it is anticipated that half of the fastest growing occupations will be in healthcare with
the highest demand for home health aides, personal care aides, physician assistants, and nurse
practitioners (Figure 18).
18
At present, the number of nurses employed in hospital settings still greatly
exceeds those in homecare, long term care, and office settings (Appendix G17).
15
The Center for Health Workforce Studies (2016). Health Workforce Analysis Guide: 2016 Edition. Albany, NY:
Author. Retrieved from http://www.healthworkforceta.org/wp-content/uploads/2016/10/Health-Workforce-
Analysis-Guide_2016-Edition.pdf
16
Keckley, PH., & Coughlin, S. (2012). The new health care workforce: Looking around the corner to future talent
management. Available from the Deloitte Center for Health Solutions.
17
Institute of Medicine. (2010). The future of nursing: Leading change, advancing health. Washington, DC: National
Academies Press.
18
Salsberg, E. & Martiniano, R. (2018, May 9), Health care jobs projected to continue to grow faster than jobs in
the general economy [Health Affairs blog]. DOI: 10.1377/hblog20180502.984593

Broome County
Community Health Assessment 2019-2024 137
Figure 17. Job Growth in Selected Settings within the Health Care Sector, 2006-2016 and Projected 2016-2026
SOURCE: Bureau of Labor Statistics, employment projections, 2016–26: Table 1.9: 2016–26 Industry-occupation matrix data, by industry; Table
2.7: Employment and output by industry, 2006, 2016, and projected 2026; Current Employment Statistics national estimates for employment,
hours, and earnings. Image retrieved from https://www.healthaffairs.org/do/10.1377/hblog20180502.984593/full/
Figure 18. Projected Annual Need for New Workers among Health Care Occupations with the Greatest Need,
2016-2026
SOURCE: Bureau of Labor Statistics, employment projections, 2016–26: Table 1.9: 2016–26 Industry-occupation matrix data, by industry; Table
2.7: Employment and output by industry, 2006, 2016, and projected 2026; Current Employment Statistics national estimates for employment,
hours, and earnings. Image retrieved from https://www.healthaffairs.org/do/10.1377/hblog20180502.984593/full/
Broome County
138 Community Health Assessment 2019-2024
Public Health Practitioners & Other Allied Health Professionals
A study of public health workforce needs conducted in six states, including NY, noted that public health
agencies, particularly those in rural areas had difficulty recruiting RNs. These recruitment issues are
most often related to budgetary constraints, non-competitive salaries, availability of RNs and adequacy
of numbers prepared with the desired level of education. Recommendations from the public health
workforce report relevant to nursing professionals include: providing support and assistance to educate
graduate and undergraduate nurses with essential knowledge, skills, and competencies for public health
practice; developing service obligated scholarship or loan repayment programs similar to the National
Health Service Corps; encouraging educational institutions to be responsive to the needs of local public
health agencies; providing incentives for collaboration between academia and public health agencies;
developing best practice models; supporting curricula for public health in schools of nursing; and
monitoring the size and composition of the public health workforce.
Data extracted from the CHWS 2016 Health workforce Planning Guide for a variety of allied health
professionals are located can be found in Appendices G11 (Healthcare Providers) and G12 (Allied
Health). These tables provide information about the absolute number of providers as well as the
number of providers per 100,000 population for Broome County as well as comparative statistics for the
Southern Tier, Upstate NY, and NYS. Provider rates for select health occupations are presented in
graphic form in Appendices G15 (Healthcare Providers) and G16 (Allied Health). Broome County exceeds
regional provider rates for most of the allied health professions including dentists, occupational
therapists, pharmacists, physical therapists, and speech language pathologists. However, the regional
availability of these allied health professionals, across rural Upstate NY and especially in the Southern
Tier, is woefully inadequate to meet the service needs of the population.
Health Professions Education
Broome County has benefitted from having two schools of nursing located within the area (Appendix
G18). Broome Community College prepares Associate Degree nurses and Binghamton University (BU),
Decker College of Nursing and Health Sciences prepares nurses with Baccalaureate, Masters, and
Doctoral (PhD) degrees. The Baccalaureate program includes both traditional students and those
seeking a second degree. In addition, RNs can obtain a BS or MS degree at BU. A majority of the students
prepared that the Masters level stay in the Upstate NY region often serving in Health Profession
Shortage Areas. The PhD program is the only doctorate focused on rural nursing in the country.
The clinical campus for SUNY Upstate College of Medicine is located in Binghamton with approximately
one-fourth of third and fourth year students complete their clinical experiences at this location. The
Clinical Campus is affiliated with United Health Services Hospitals and a network of family care centers.
The Decker School of Nursing has expanded to become the Decker College of Nursing and Health
Sciences offering graduate degrees in Public Health, Physical Therapy, Occupational Therapy, and
Speech Language Pathology. The Decker College will be located in Johnson City next to the New College
of Pharmacy and Pharmaceutical Sciences. Development of interprofessional experiences and
competencies along with advanced simulation training are included in all health profession curricula.

Broome County
Community Health Assessment 2019-2024 139
Primary Care & Preventive Health Services Utilization
Southern Tier Cancer Services Program
The Cancer Services Program of the Southern Tier (CSP) serves Broome, Chemung, Chenango, Schuyler
and Tioga Counties. The purpose of the program is to increase breast, cervical and colorectal cancer
screenings by offering reimbursement for these services for the uninsured. The program offers breast
and cervical screenings to individuals age 40-64 and colorectal screenings to individuals ages 50-64.
There are exceptions to the age groups in cases where there are increased risk factors (as determined by
the program guidelines). If an individual is diagnosed with breast, cervical, colorectal or prostate cancer,
staff can meet with him or her to determine if they are eligible for the Medicaid Cancer Treatment
Program, utilizing the Cancer Services Program income eligibility criteria. This program provides
Medicaid insurance coverage through the duration of their treatment.
The Cancer Services Program is a program of the New York State Department of Health and funding is
provided by New York State and the Centers for Disease Control and Prevention. The program is only
available to New York State residents.
The majority of individuals who participate in the program are low-income, working, and uninsured
individuals. Recently there has been an increase in the number of individuals contacting the program,
usually through referrals, who have lost their jobs and their health insurance coverage.
Triaging Clients for Public Health Insurance Programs:
The CSP of the Southern Tier screens clients for eligibility over the phone. There is no need for proof of
income or insurance status in order to receive program screening services. Clients are sent a NYS
attestation, stating that they are over 40 and that the insurance status and income information is
accurate. At this time, callers are offered referrals for local insurance navigation programs as a resource
to assist them with reviewing their eligibility for public health coverage program options. Clients are
also referred to Patient Financial Assistance Programs offered through United Health Services and
Lourdes Hospitals. These programs offer uninsured patients billing discounts or charity care based on
their income
Medicaid Cancer Treatment Program Coverage:
The Medicaid Cancer Treatment Program Coverage (MCTP) is a program specifically designed to serve
clients who have been diagnosed through the CSP or who have no health insurance and are in need of
cancer treatment services/procedures. CSP staff meets with clients who have been diagnosed with
breast, cervical, colorectal or prostate cancer and those who have been diagnosed with pre-cancerous
cervical conditions, and complete the MCTP application on behalf of Medicaid Enrollment Officers who
work directly with NYSDOH CSP. The income guidelines are higher, allowing the client to make up to
250% of the Federal Poverty Guideline. In cases of a breast or cervical diagnosis, there is no income
exclusion. The application process is expedited. If approved, the client receives full Medicaid coverage
for a determined timeframe. Generally, if the client is diagnosed with cancer, they receive coverage for a
full year, with annual renewals. CSP staff again meets with the client to complete the recertification
application. In order to be eligible, the client must still be receiving or in need of treatment.

Broome County
140 Community Health Assessment 2019-2024
C. Emerging Issues in the Community
Emerging issues in the community were identified by the Broome County Community Health
Assessment Steering Committee through analysis of health indicators, discussion of partner experiences
and observations of serving client needs, through local surveys conducted by community agencies, from
priorities set by state and local government, and based on current events affecting community
members’ daily lives. The topics identified related to
Prevalent conditions affecting peoples’ lives, especially youth, and resulting in high mortality
and years of productive life lost: the opioid epidemic and the vaping scourge
State and national priorities to improve people’s lives across the lifespan: the Age Friendly
initiative, and
Underlying social determinants of health: food insecurity, housing, transportation, and access to
affordable healthcare
For the first time, Master of Public Health (MPH) graduate students enrolled in a newly established
program of study at Binghamton University were available to participate in the Community Health
Assessment process. These MPH students together with an intern from Binghamton University’s
Anthropology department participated in and contributed to nearly every facet of the MAPP process.
Funding for their work was possible through the Population Health Improvement Program. These
students not only gained invaluable public health knowledge, skills, and competencies but also
significantly expanded local public health capacity to conduct the Community Health Assessment and to
advance the health of Broome County residents through development of the Community Health
Improvement Plan.
The sections that follow reflect the work of these students who were tasked with conducting a review of
the topics: (a) investigating the nature of the issue in Broome County, (b) examining best practices and
the evidenced-base for interventions, (c) exploring strategies currently employed by community
partners to address the issue, and (d) appraising evidence informed solutions that have the potential to
significantly and positively impact the issue.
The Opioid Epidemic
Background
According to the Centers for Disease Control and Prevention (CDC), from 1999 to 2017, more than
702,000 people have died from a drug overdose. Unintentional injury is now the leading cause of death
in the United States for ages 1-44, and drug overdose is the leading cause of unintentional injury for
ages 25-64. In 2017 more than 70,000 people died from a drug overdose, and of those deaths almost
68% involved a prescription or illicit opioid. Two out of three drug overdose deaths involve an opioid
and have been responsible for over 47,000 deaths in 2017 (CDC, 2019). The total economic burden for

Broome County
Community Health Assessment 2019-2024 141
prescription opioid misuse alone in the United States is 78.5 billion per year. In addition to the rising
numbers of overdoses, the National Institute on Drug Abuse reported an increase in the incidence of
neonatal opioid withdrawal syndrome (NOWS) and neonatal abstinence syndrome (NAS) from 2004 to
2014 (1.5 cases per 1000 hospital births to 8.0 cases per 1000 hospital births). The cost of the rising
incidence of NAS and NOWS increased from 93 million in 2004 to 563 million in 2014 (National Institute
on Drug Abuse, 2019).
According to the New York State Department of Health, opioid overdose deaths have significantly
worsened from 2015-2016 with 15.1 deaths per 100,000 population in 2016 in New York state. The
overdose death rate involving heroin in 2016 was 6.5 deaths per 100,000 and deaths involving opioid
pain relievers was 11.7 deaths per 100,000. A subcategory of opioid pain relievers, synthetic opioids
excluding methadone, contributed to 8.3 deaths per 100,000, including illicit fentanyl products. Higher
rates of overdose deaths were seen in males compared with females in 2016 in New York State. An
increase from 7.5 deaths per 100,000 population in 2010 to 22.3 deaths per 100,000 in 2016 was seen
among males, compared with 3.4 deaths per 100,000 in 2010 to 8.1 deaths per 100,000 in 2016 among
females. In 2016 rates of overdose deaths were highest for White non-Hispanics, 19.8 per 100,000
compared with 10.5 per 100,000 for Black non-Hispanics and 12.6 per 100,000 for Hispanics (New York
State Department of Health, Opioid Dashboard)
In Broome County, the crude rate of overdose deaths involving any opioid significantly worsened from
2015 to 2016 with an increase from 14.2 deaths per 100,000 in 2015 to 29.2 deaths per 100,000 in 2016.
The crude rate of overdose deaths involving any opioid aged 18-44 significantly worsened from 2015 to
2016 increasing from 24.3 per 100,000 to 52.0 deaths per 100,000 in Broome County. This rate is
significantly higher for Broome County than seen in the Southern Tier and NYS excluding NYC. The
overdose deaths involving any opioid age adjusted rate significantly worsened from 2015 to 2016, with
an increase from 16.0 per 100,000 in 2015 to 32.1 per 100,000 in 2016 (New York State Department of
Health, Opioid Dashboard). The Broome County District Attorney reported 24 overdose deaths in 2017,
13 overdose deaths in 2018 and 9 overdose deaths in 2019 as of September (Broome County Health
Department).
The aged-adjusted rate per 100,000 for overdose deaths involving heroin in Broome County significantly
worsened from 2015 to 2016, increasing from 8.0 per 100,00 to 15.4 per 100,000. This rate is
significantly higher than those seen in the Southern Tier and NYS. The age-adjusted rate for overdose
deaths involving opioid pain relievers per 100,000 population in Broome County was 18.2 in 2016
compared with 12.0 in NYS. Both the crude and age adjusted rates for overdose deaths involving
synthetic opioids other than methadone have significantly worsened from 2015 to 2016. The age
adjusted rate for all emergency department visits (including outpatients and admitted patients) in 2016
involving any opioid overdose was 139.7 per 100,000 compared with 56.0 per 100,000 in NYS. The crude
rate of emergency department visits in 2016 (including outpatients and admitted patients) aged 18-24
years involving any opioid overdose was 170.8 per 100,000 compared with 104.5 per 100,000 in NYS,
and for ages 25-44 was 316.0 per 100,000 compared with 103.4 per 100,000 in NYS. The age adjusted
rate for all emergency department visits (including outpatients and admitted patients) in 2016 involving
any opioid overdose was 139.7 per 100,000 compared with 56.0 per 100,000 in NYS (New York State
Department of Health, Opioid Dashboard).
These significant increases in overdose deaths and emergency department visits in Broome County
highlight the need for immediate action. It is essential to identify risk factors and eliminate barriers to

Broome County
142 Community Health Assessment 2019-2024
life saving treatment by increasing access and availability to overdose reversal trainings and medication
assisted treatment. The community approach must be further utilized to continue developing
interventions and decreasing the stigma associated with those suffering from opioid addiction, in order
to decrease the prevalence of fatal opioid overdoses in Broome County.
Evidence Base & Best Practices
The CDC has listed several evidence-based interventions that address the opioid overdose crisis. Many
of these practices are already being implemented in Broome County, including, targeted Narcan training
and education, Medication Assisted Treatment (MAT), and Academic Detailing (CDC). Targeted Narcan
distribution ensures that those who are greatest risk of overdose or those who are most likely to
encounter someone who is at risk of overdosing receives Narcan training and is provided with a Narcan
kit. Other evidence-based strategies for Narcan distribution include community distribution and
equipping first responders. Medication Assisted Treatment (MAT) combines behavioral therapy and FDA
approved medications to treat substance use disorders by preventing painful opioid withdrawal
symptoms. Many studies have shown that MAT contributes to significant reductions in opioid use and
overdose. Academic detailing is an educational strategy that is designed to provide tailored training and
technical assistance to healthcare providers, done so by trained professionals using marketing
techniques, to help providers use best practice methods when prescribing opioids to their patients.
When a series of tailored educational sessions were used for a group of providers on Staten Island, a 29
percent decrease in the rate of prescription opioid overdoses on Staten Island was observed (Carroll,
Green, Noonan, 2018).
Current Interventions
Broome Opioid Awareness Council
The Broome Opioid Awareness Council (BOAC) was created in 2014 in response to a significant increase
in opioid related overdoses and fatalities. BOAC focuses on identifying barriers and developing solutions
for the issues resulting from the increase of drug abuse in Broome County. The council functions as a
coalition together with community agencies from treatment and prevention services, law enforcement
and peer response, statistics and data, community education, rural communities, and media and
advocacy sectors to increase community collaboration, with the goal of decreasing youth and resulting
adult substance use and its impact on the community. The focus areas of BOAC encompass an entire
community response including community education, outreach and prevention, law enforcement
response, substance abuse treatment, and educating medical professionals. BOAC seeks to target
factors existing in Broome County that place youth at risk for substance abuse, reduce risk factors and
enhance protective factors, increase community collaboration and awareness, and overall create a
healthier, safer community. Through support from the Broome County Health Department, BOAC has
worked towards implementing multiple response strategies to reduce deadly drug overdoses including
education and public information messaging, harm reduction strategies, and the use of law enforcement
to prosecute fentanyl drug dealers and increased paroling of drugged drivers, which is funded through
STOP-DWI and DA’s office for Advanced Roadside Impaired Driving Enforcement (Broome County Health
Department).
Drug Free Communities

Broome County
Community Health Assessment 2019-2024 143
Drug Free Communities (DFC), a federally funded grant through Substance Abuse and Mental Health
Services Administration, was enacted in 2016 and addresses the factors in a community that increase
the risk of substance use and promotes protective factors that minimize those risks. It also focuses on
strengthening community coalitions with a goal of reducing substance abuse among youth and adults
and works with and supports BOAC’s mission and goals. One of the ways DFC measures current
substance use, risk factors and protective factors is through the administration of the Prevention Needs
Assessment to local schools. This assessment is used to provide data and serves as a tool for education
purposes for the youth and adults of Broome County (Broome County Health Department).
Naloxone Trainings
Naloxone trainings and overdose recognition education are offered through Truth Pharm, Southern Tier
Aids Program, Addiction Center of Broome County, Lourdes Youth Services Alcohol and Drug Education
Prevention Team (ADEPT), and Binghamton University. Binghamton University has become the first
University to be certified as an Opioid Overdose Prevention Site.
Medication Assisted Treatment
Medication Assisted Treatment (MAT) is offered through the Addiction Center of Broome County
(ACBC), United Health Services Southern Tier Drug Abuse Treatment Center and New Horizons. ACBC
provides a Vivitrol Program, the Southern Tier Drug Abuse Treatment Center offers a Methadone Clinic
and New Horizons provides Suboxone (Buprenorphine). MAT will be available through the Family &
Children’s Society soon.
Inpatient/Outpatient services and treatments
Fairview Recovery Services offers community residence for both men and women, as well as supportive
living, shelter and housing plus care. Helio Health provides medically supervised withdrawal and
stabilization services, as well as inpatient rehabilitation services. United Health Services New Horizons
offers both an inpatient and outpatient unit. The Addiction Center of Broome County is providing
intensive outpatient groups and outpatient rehabilitation groups. The Family and Children’s society
provides an outpatient substance use treatment program.
Prescription drop box locations
There are numerous prescriptions drop box locations available in Broome County to return unused
prescription opioids for destruction including the Endicott police dept, Broome County office building,
Broome County Library, and Broome County Sheriff’s Office. Prescription take back days are also offered
through the Broome County Health Department.
Connection to Resources
There are many crisis hotlines available 24 hours a day including the Drug Abuse Crisis Line provided
through United Health Services New Horizons and HOPEline provided through New York State’s Office of
Alcohol Substance Abuse Services (OASAS). The Broome County District Attorney’s office created
Operation S.A.F.E. (Save Addicts from Epidemic) as a hotline for family members or those facing
addiction who need support and resource assistance for treatment options and other available
resources in Broome County. The Broome County Sheriff’s Office developed the Assisted Recovery
Initiative to assist individuals that are suffering from substance use disorder who are voluntarily seeking
treatment.

Broome County
144 Community Health Assessment 2019-2024
Potential Interventions
To further strengthen the interventions already present in Broome County there are potential
interventions to be considered including an Opioid Fatality Review Team, expanded Naloxone trainings
offered more frequently through multiple organizations in Broome County, strengthening peer response
efforts, as well as more organizations offering MAT in Broome County.
Other states such as Maryland and Utah have created local Overdose Fatality Review Teams in response
to the rising number of opioid overdose fatalities. Some of the major goals of these review teams are to
identify missed opportunities for prevention and gaps in the system, build working relationships
between local stakeholders and improve communication within a jurisdiction, recommend policies,
programs or changes to local law to prevent more overdose deaths, and inform local and state overdose
and opioid misuse prevention strategy. (Maryland Department of Health, 2015)
The National Association of County and City Health Officials (NACCHO) provides funding for Opioid
Overdose Epidemic Toolkit for local health departments. This Toolkit monitoring and surveillance,
prevention, harm reduction and response, linkages to care, stakeholders and partnerships (NACCHO)
Summary
In response to the increasing rates of overdose deaths involving opioids in Broome County, community
partners and organizations have begun implementing interventions that identify risk factors, provide
lifesaving treatment, and help those who are suffering with addiction get connected with help and
treatment. Although there has been a positive response from the community, there is opportunity to
strengthen this response even further in Broome County, and expand these interventions while reducing
the stigma surrounding opioid drug use.
The Broome County Community Health Improvement Plan (CHIP) interventions that address this issue
focus on increasing availability and access to overdose reversal trainings and medication-assisted
treatment options, promoting prescriber education and familiarity with opioid prescribing guidelines,
establishing additional permanent safe disposal sites for prescription drugs and organized take-back
days, and building support systems to care for opioid users or those at risk of an overdose. Most of
these interventions reflect evidence-based strategies that have been implemented in other jurisdictions
and have shown to be effective at reducing overdoses or other risk factors that may increase the
likelihood of an overdose to occur (CDC, 2018).
References
Centers for Disease Control and Prevention (CDC). (2018). Understanding the Epidemic. Retrieved from
https://www.cdc.gov/drugoverdose/epidemic/index.html
National Institute on Drug Abuse (2019). New York Opioid Summary. Retrieved from
https://www.drugabuse.gov/opioid-summaries-by-state/new-york-opioid-summary
Carroll, J., Green, T., Noonan, R. (2018). Evidence-Based Strategies for Preventing Opioid Overdose:
What’s working in the United States. Centers for Disease Control and Prevention, 1-40. Retrieved
from https://www.cdc.gov/drugoverdose/pdf/pubs/2018-evidence-based-strategies.pdf
New York State Department of Health Opioid Dashboard (2018). State and County Level Opioid Data

Broome County
Community Health Assessment 2019-2024 145
New York State Department of Health (2018). Opioid Annual Data Report. Retrieved from
https://health.ny.gov/statistics/opioid/data/pdf/nys_opioid_annual_report_2018.pdf
National Association of County & City Health Officials. Opioid Overdose Epidemic Toolkit. Retrieved from
https://www.naccho.org/programs/community-health/injury-and-violence/opioid-
epidemic/local-health-departments-and-the-opioid-epidemic-a-toolkit
Maryland Department of Health. Overdose Fatality Review Program. Retrieved from
https://bha.health.maryland.gov/OVERDOSE_PREVENTION/Pages/OFR-.aspx
Broome County Health Department (2019). Broome Opioid Awareness Council
Broome County Health Department (2019). Treatment Resources in Broome County
The Vaping Scourge
Opportunity
Electronic cigarettes, also known as vapes, e-cigarettes, vape pens, electronic nicotine delivery systems
(ENDS), have been the most commonly used tobacco product among youth since 2014. They contain a
battery that heats a flavored liquid into an aerosol that is inhaled. The liquids usually contain nicotine,
which is a highly addictive substance, and flavorings in a base of propylene glycol and vegetable glycerin
(CDC & NYS Dept of Health). At this time, vaping is not approved by the Food and Drug Administration
(FDA) as a smoking cessation aid, and is not considered to be an FDA-approved form of nicotine
replacement therapy (CDC, 2019)
According to the Centers for Disease Control and Prevention, in 2018 more than 3.6 million middle and
high school students used e-cigarettes in the past 30 days in the United States. This included 4.9% of
middle school students and 20.8% of high school students. Youth are more likely than adults to use e-
cigarettes and use them more than cigarettes, cigars, smokeless tobacco and hookah. In 2017 only 2.8%
of U.S. adults were current e-cigarette users and among the e-cigarette users in adults in 2015, 58.8%
were current regular cigarette smokers, 29.8% were former cigarette smokers, and 11.4% had never
been regular cigarette smokers. In 2015, among adult e-cigarette users, only 1.3% had never been
cigarette smokers, and among youth e-cigarette users aged 18-24 years, 40% had never been regular
cigarette smokers (CDC, 2018).
In New York state, according to the NYS Youth Tobacco Survey, from 2014 to 2016, the e-cigarette usage
among youth doubled from 10.5% to 20.6%, and from 2014 to 2018 this rate increased fully 160%. In
2018, according to the Youth Tobacco Survey 27.4% of high school students reported e-cigarette use.
About five times as many high school students in New York state use e-cigarettes compared with
smoking cigarettes. Few students plan to try smoking cigarettes, but an increasing amount are open to
e-cigarettes and more than half of teenagers believe that nondaily e-cigarette use causes little or some
harm. Of those youth who do use e-cigarettes, a third of them believe nondaily e-cigarette usage is
harmless. Youth and young adults claim their reasons for trying and using e-cigarettes are flavor, taste,
curiosity, and belief that they are less harmful than other tobacco products. The use of e-cigarettes does
not prevent youth from smoking, and those who use e-cigarettes are at an increased risk for starting
smoking and continuing to smoke. More than half of high school students and young adults who smoke

Broome County
146 Community Health Assessment 2019-2024
also use e-cigarettes, known as dual use (NYSDOH). A statewide health advisory on vaping associated
pulmonary illness was issued by the New York State Department of Health in August 2019. From August
2019 to November 2019, NYSDOH reported an increase in the number of Vaping-Related Illness reports
they received, increasing from about 10 the week of August 6th to about 200 as of November 11
th
. The
highest spike in cases reported weekly was the week of September 10
th
with more than 25 cases
reported (New York State Vaping-Related Illness Investigation, NYSDOH).
In Broome County, according to the latest Prevention Needs Assessment conducted in 2018, there was a
reported increase in students that use e-cigarettes. 26.5% of students surveyed reported using an e-
cigarette in their lifetime and 28.8% used one in the past 30 days. These rates are significantly higher
than the national data for past 30-day use, 20.8% in the United States compared with 28.8% in Broome
County, and higher than the state level of high school student e-cigarette use as well (28.8%, 27.4%).
Current Interventions
New York has been a leading state in implementing and amending public health laws to decrease use of
tobacco products, including e-cigarettes, among its residents. Some of these laws include the Clean
Indoor Air Act and the Adolescent Tobacco Use Prevention Act (ATUPA). The Clean Indoor Air Act was
enacted in 1989 and amended in 2017 to include e-cigarettes. This act prohibits the smoking of tobacco
products in almost all places of employment, including restaurants and bars in all of New York state.
ATUBA was enacted in 1992, and prohibits the sale of any tobacco product to minors that are under the
age of 18. Amendments were made to ATUBA to include e-cigarettes under the term “tobacco
products”. Effective November 13
th
, 2019, the minimum age of sale will be increased to 21 years of age
in all of New York State. Smoking and vaping are prohibited at New York playgrounds between sunrise
and sunset if anyone under the age of twelve is present and smoking or vaping outside on hospital
grounds is prohibited as well. Since the early 2000’s many youth anti-cigarette smoking campaigns and
educational programs were developed including NYS Tobacco Control Program and Reality Check. These
programs have now expanded to include anti-vaping messages and provide educational programs for
schools educating youth on the dangers of vaping.
In Broome County, many policies have been implemented and laws amended to limit availability and
public use of e-cigarettes. Public policy, educational programs, and community awareness events have
been utilized as preventative methods in the county. The Prevention Coalition of Broome County, which
is comprised of 12 sectors from within the community, has been a leader in planning, implementing and
evaluating prevention practices and programs in the community. The coalition uses data from the
Prevention Needs Assessment conducted in Broome County to highlight certain substances as high
priority areas among youth to focus prevention efforts. In 2018, they selected alcohol, marijuana, and
tobacco as high priority substances. Tobacco Free Broome and Tioga, which functions as a community
partner of the New York State Tobacco Control Program and is funded by a grant from the New York
State Department of Health, is a partnership of community-based organizations and individuals
committed to building healthier communities through tobacco-free living. Some of the programs
supported by Tobacco Free Broome and Tioga include Tobacco-Free Outdoors, Point of Sale, Smoke-
Free Media, Smoke-Free Multi-Unit Housing, and Reality Check. Reality Check is an educational program
targeted at youth to empower and engage them to produce changes and prevent the use of tobacco
products, including e-cigarettes.

Broome County
Community Health Assessment 2019-2024 147
As of August 2017, Binghamton University has transitioned to a tobacco free campus as a part of a
Tobacco Free Initiative. Under this initiative, the tobacco free policy prohibits the use of any tobacco
products, including e-cigarettes, on all university property. The main goal of this policy is to provide a
healthy campus environment and to promote the well-being and safety of all Binghamton University
faculty, staff, students, and visitors. As a part of this initiative, the University provides smoking cessation
programs and devices that are readily available.
Many public policies have been enacted and amended, with educational programs strengthened in
Broome County to prevent youth from engaging in vaping related activities. However, vaping rates
among youth are still on the rise prompting a need for further strengthening of these interventions.
References
Centers for Disease Control and Prevention (CDC) (2019). About Electronic Cigarettes. Retrieved from
https://www.cdc.gov/tobacco/basic_information/e-cigarettes/about-e-cigarettes.html
New York State Department of Health. (2019). Get the Facts- Electronic Cigarettes (E-cigarettes) and
similar Vapor Products. Retrieved from
https://www.health.ny.gov/prevention/tobacco_control/campaign/e-cigarettes/
New York State Department of Health. (2019). Tobacco Control Policies in NYS. Retrieved from
https://www.health.ny.gov/prevention/tobacco_control/current_policies.htm
New York State Department of Health. (2019). Electronic Cigarette Use by Youth increased 160%
between 2014 and 2018. Retrieved from
https://www.health.ny.gov/prevention/tobacco_control/reports/statshots/volume12/n1_electr
onic_sig_use_increase.pdfhttps://www.health.ny.gov/prevention/tobacco_control/reports/stat
shots/volume12/n1_electronic_sig_use_increase.pdf
New York State Department of Health. (2019). New York State Vaping-Related Illness Investigation.
Retrieved from https://www.health.ny.gov/prevention/tobacco_control/docs/vapireport.pdf
Binghamton University. (2019). Tobacco Free Campus Policy. Retrieved from
https://www.binghamton.edu/operations/policies/security-and-safety/tobacco-free-campus-
policy.html
Prevention Needs Assessment, 2018
https://www.stopbinghamtonvaping.com/
Tobacco Free Broome and Tioga. Who we are. Retrieved from http://tobaccofreebt.org/whoweare

Broome County
148 Community Health Assessment 2019-2024
The Age Friendly Initiative
Integrating the Domains of Livability into Prevention Agenda Priorities
As people are living longer lives it has become essential to create and support initiatives to improve the
experiences of aging. A statewide executive order issued by Andrew Cuomo directs state agencies to
include New York State Prevention Agenda priorities and the AARP/World Health Organization eight
domains of livability for Age Friendly communities, where appropriate, in agency policies, procedures,
and procurements. As a result of his efforts and those of groups and individuals throughout the state,
NYS has been named by AARP and the World Health Organization as the first Age Friendly state in the
nation. Broome County, with rates of residents aged 60 years and older above the state and national
figures, is working to become an Age Friendly community through integrating these priorities and
domains of livability into our county Prevention Agenda.
The inclusion of Age Friendly concepts in the Prevention Agenda highlights the need for community
participation in efforts to improve the health and quality of life of aging adults. Their inclusion means
that Age Friendly concepts will be focused on as priorities for action, that tangible goals will be set, and
that related interventions will be undertaken by agencies throughout the county. The goal of the project
is for all people in our communities to: feel safe in the community, participate in community activities,
be treated with respect, have access to safe, appropriate and affordable housing and transportation,
have access to recreational opportunities and health services, know what services and activities are
available and have access to information by a means they prefer (e.g. online, in print, in person), be
active, vital contributors to the economic, civic, and social life of the community, and receive
appropriate support if they can no longer look after themselves.
Improvements will be brought about through targeted actions and investments by the county, like the
pioneering of multi-faceted programs that support aging in place and the implementing of smart growth
reforms that directly support the prevention agenda goals and ultimately the eight domains of livability.
Such actions and investments are achieved through system level changes, like offering incentives to
agencies in the county for integrating Age Friendly concepts into their action plans, establishing new
procurement guidelines and financing models, and implementing regulatory changes.
This new strategic focus on improving the wellness of people across their lifespan will help to create and
foster a healthier, more integrated, sustainable, and equitable Broome in which people of all ages can
easily receive services, take part in, and move around their community.
Broome Survey
In 2018-2019, nine focus groups were conducted and over 2,000 surveys were collected to assess the
health and wellness of our older adults and identify areas for improvement.
The survey results reveal areas in need of the most urgent attention: Housing, Transportation, Mental
Health, Physical Health, Caregiving, Financials, and Social Integration. A summary of the survey findings
is below.

Broome County
Community Health Assessment 2019-2024 149
Housing
Most older adults reported that their community was a good place to live, and that they were somewhat
confident that they will be able to continue living in their current residence as long as they like. Many do
not plan on moving from their current home (37.92%), but those who would consider moving would do
so to reduce living costs (22.36%) or because they can no longer maintain their home (36.17%). Over
27% reported that their home needed major repairs that would cost $1,000 or more to fix, and about
28% reported that their home needed small repairs that they were unable to take care of themselves.
Repairs can be costly and contractors hard to find, and because some older adults are not physically able
to do the work that they need done themselves, many of their homes need repairs to be livable.
Participants in the survey commented that a need for home repairs, a lack of reliable and affordable
contractors (especially in rural areas), and a lack of Aging in Place organizations (allowing older adults to
help each other as they age) are all major issues that make it hard to stay in their homes. Seniors who
choose to move from their homes are faced with the trouble of finding safe, affordable and clean
housing. Wait lists for subsidized housing can be very long, and affordable options in Broome are often
in areas with high crime rates. They reported a desire for more housing options, including housing for
middle income seniors with a clubhouse/pool, housing that can be purchased rather than rented, one
level housing options and town houses, and senior housing communities with access to transportation,
social meeting places, and walking paths. Many also reported a desire to live in a walkable community
with accessible public green spaces, easy access to outdoor cafes, shopping, sitting areas, and bike trails.
Transportation
Difficulty accessing medical care within the county was the most common issue for older adults caused
by lack of transportation options. This issue, along with difficulty attending social events and obtaining
food, was primarily reported by individuals with incomes below 19,999/ year, compared to higher
income groups. These individuals were also less likely to drive, to ask others for help, more commonly
had physical impairments that prevented them from driving, and more often reported that public
transportation was inconvenient. Accessibility of transportation for older adults is related to their
income in Broome.
These issues have caused isolation in older adults, especially those in rural areas, because of a lack of
transportation options, door to door transportation, and affordable and convenient transportation.
Together these issues prevent seniors from attending social events and necessary appointments. Survey
participants reported a desire for improved transportation options including rural areas, park and ride to
help access downtown area, more information on transportation options, and bus stops and shelters to
protect them from the elements.
Health
The survey found that the health of older adults in Broome varies between income levels. Those with
incomes below $19,999 were more likely to report fair to poor physical health than those with higher
incomes. This may in part have to do with the increased difficulty lower income individuals have with
accessing both the limited home care options and aids available to help with healthy aging in the
community and the limited geriatric health care options for both primary and secondary care needs.
Individuals in this income group also reported less exercise or physical activity. Physical health factors
are also reported to vary based on the age of the senior. Increased age was not directly associated with

Broome County
150 Community Health Assessment 2019-2024
exercise rates, as the 60-65 age group reported less exercise or physical activity than other age groups.
However, older age was associated with increased falls and higher rates of reporting those falls to
primary care providers than younger seniors. Both income and age are negatively correlated with
physical health in Broome.
Those with incomes below $19,999 were also more likely to report fair to poor mental health than those
with higher incomes. However, individuals in this income group were less likely to report barriers to
getting mental health services (22%) than those with higher incomes did (40%), though high costs of
services were one of the most reported barriers to access. This discrepancy may be due to differences in
rates of seeking mental health assistance, and so noticing barriers to access. Survey participants
reported other common barriers to getting mental health services: a lack of mental health professionals
and resultingly long wait lists, difficulty navigating available mental health services and finding a starting
point for a referral, hours of operation for existing mental health services, and stigma associated with
mental health issues. Poor mental health among older adults may be then be due to several factors.
These factors include difficulty of accessing available services, limited respite options for caregivers and
grandparents raising grandchildren and social isolation. These barriers and contributing factors to
mental health in older adults are more likely to negatively influence the health of individuals with lower
incomes.
Caregiving
More than half of older adults surveyed considered themselves current or former caregivers and
reported that various supports would be helpful for themselves or other caregivers. The most common
improvement idea reported as potentially helpful was an increase in information about available
resources for caregivers in the community (51.33%). Other supports that would be helpful include
assistance with transportation (45.26%), short breaks/ respite from caregiving tasks (44.75%), assistance
securing paid help (39.57%), assistance in completing forms and applications (36.03%), assistance with
finding accurate medical information (including understanding medical bills) (32.62%), and connecting
with other caregivers (25.41%).
The participants surveyed would like a place in Town of Chenango for caregivers to drop off their loved
ones when they need a break from their duties, more grief support groups, more paid caregivers to help
them age in place, and some solution to reduce caregivers’ guilt about seeking help to care for their
loved ones.
Financial
During the past year, 23.31% of older adults were unable to pay for some essential health or housing
bill. The top financial issues faced differed between age groups. Adults aged 50-59 years had the most
trouble paying for rent/ mortgage/ taxes, utility bills, and dental care. Adults aged 60-65 and 66-74 years
had trouble paying for dental care, eyeglasses, and rent/ mortgage/ taxes. Adults aged 75 and over
faced issues paying for dental care, eyeglasses, and hearing aids. Older adults during the last year were
also not always able to buy food (6.96%), fill a prescription for medicine (4.89%) pay for health insurance
premiums (3.03%), or obtain needed medical care (2.71%). Many seniors are unable to pay for services
they need because they are over the income threshold to qualify for assistance like Medicaid. Some did
not adequately prepare for the financial expenses brought on by aging. Survey participants reported a
desire for help paying for hearing aids, glasses and dental expenses, and prescriptions.

Broome County
Community Health Assessment 2019-2024 151
Social
Almost 28% of older adults reported feeling socially isolated, especially those with incomes less than
$19,999 and between the ages of 55-65 years. Older adults do not engage in social activities they would
enjoy primarily because of physical (38.21%) and financial (31.18%) constraints, and because they have a
hard time finding activities that interest them (32.51%). Other reported barriers to social engagement
include a lack of awareness about activities that are available (28.33%), lack of transportation (19.01%),
a feeling that they are not welcome (13.12%), and safety concerns (7.22%).
Participants desired more activities for younger seniors, like yoga classes, low impact exercise options at
senior centers, walking clubs, dances and dinners, and meet and greet activities. They reported a need
for more multi-generational programs, like kids at senior centers and seniors in schools. Participants also
commented on tandem/wheelchair bikes on the Rail Trail and classes on how to use iPhones.
Results
The survey has helped to illuminate specific issues that older adults in Broome are facing and has
provided an avenue for respondents to be part of the solution-making process. This information will
help to inform initiatives around the county, and as these initiatives and others currently underway
unfold, future survey results and Prevention Agenda contents will likely be different, reflecting progress
made. As a result of adopting an Age Friendly framework for action through the integration of Age
Friendly concepts into the county Prevention Agenda, the physical, mental, social, and economic
wellness of residents of all ages in Broome are already seeing major improvements.
Food Insecurity
Food insecurity refers to the US Department of Agriculture’s measure for lack of access to
enough food for an active, healthy life for all household members and limited or uncertain
availability of nutritionally adequate foods (Feeding America, 2016). Such households are not
necessarily food insecure at all times and often reflects a balance between meeting basic needs
(e.g., housing) and purchasing nutritionally adequate foods.
An estimated 13% of Broome County residents experience food insecurity compared 12% in
New York State (Robert Wood Johnson Foundation, 2016). Even more startling is that 19.9% of
Broome County children are food insecure (Feeding America, 2017). There is an inextricable
relationship between food insecurity and poverty. In Broome County, 23% of children live in
poverty and 49% of children and eligible for free or reduced lunch in schools (Robert Wood
Johnson Foundation, 2019). Proximity also influences food insecurity. Food “deserts” and
“swamps” are common in Broome County, particularly in the economically stressed areas of
Binghamton, Johnson City, and Endicott (Cornell Cooperative Extension, 2016). Among all
Broome County residents, 12.8% of people have low access to grocery stores (US Department
of Agriculture, 2015).

Broome County
152 Community Health Assessment 2019-2024
0% 10% 20% 30% 40% 50% 60%
SFMNP
SNAP
WIC Cash
WIC
Percent of Farmers' Markets accepting WIC Cash, SFMNP,
WIC and SNAP, 2016
Broome County
Sadly, children who live in households without access to nutritious foods are more likely to be
malnourished compromising their ability to learn and employment potential as well as
protracting the cycle of poverty.
Current Interventions
Many organizations in Broome County are working to address food insecurity. The Broome
County Child Hunger Task Force brings together stakeholders from school, government and
non-profit organizations to increase access to, knowledge of and consumption of healthy foods.
These stakeholders do innovative work at the individual and at the system levels.
Many food pantries are available in Broome County. Food Bank of the Southern Tier
administers the Backpack Program, which sends children home from school on weekends with
food to have at home. In summer 2019, 36 locations participated in the federal Summer Meals
program. Various nutrition and cooking programs exist, offered by Cornell Cooperative
Extension, Healthy Lifestyles Coalition, VINES, and others. Additionally, Volunteers Improving
Neighborhood Environments (VINES) offers community gardens and Farmshare, a CSA program
accepting SNAP benefits and offering income-based discounts. CHOW’s Fresh Mobile Produce
Market is a mobile market that travels throughout Broome County, offering fresh produce and
pantry staples at low or no cost. Customers may use cash, SNAP, WIC, FreshConnect, or Senior
Farmers’ Market Coupons. Several farmers markets in Broome County also accept payment via
food assistance programs (US Department of Agriculture, 2016).
SOURCE: US Department of Agriculture Food Atlas, 2016 Data

Broome County
Community Health Assessment 2019-2024 153
A pilot Fruit and Vegetable Prescription (FVRx) program has been successful in removing cost
barriers and educating about the effect of diet on health among the Medicaid population.
Participants are recruited by their healthcare provider, receive education about nutrition and
healthy eating, and receive FVRx vouchers each which, which they may redeem for fresh,
nutritious food via a VINES Farmshare, the CHOW Fresh Mobile Produce Market, or at the
Broome County Farmers’ Market.
Broome Tioga BOCES has worked extensively to expand breakfast offerings in Broome County
schools via Breakfast in the Classroom, Breakfast after the Bell and Universal Breakfast. Broome
Tioga BOCES has also championed NY Thursdays and Farm to School, increasing the demand for
fresh, healthy and local agricultural products in Broome County schools.
Opportunities
At the time of writing the 2019-2024 Broome County Community Health Assessment,
construction is underway on a grocery store that will serve the North Side of Binghamton
beginning in Spring 2020. The North Side is a food desert; it has been without a grocery store
for over twenty years. Broome County Council of Churches will operate the grocery store, which
will sell food staples and produce at low cost. Profits from the store will be directed toward the
Emergency Food Program, which provides emergency food assistance to Broome County
families. Establishment of this grocery store will increase food security for the approximate
12,000 people who live on the North Side.
Broome County Child Hunger Task Force has also identified opportunities for existing
community garden programs, urban farms, subsidized CSA programs, Farm to School initiatives,
and mobile markets to expand in size and scope.
The Housing Crisis
Opportunity for Action
Housing Affordability
Housing is a prominent issue in our nation with several different demographics being affected. Housing
is classified as affordable when it consumes less than 30% of a household’s income. Out of the 7.3
million households in New York State 2.8 million reported having housing costs that account for 30% or
more of their income. The figures become even more disparate when you split the households between
renters and homeowners. Nearly half of all renters and more than one in four homeowners are above
the affordability threshold. The U.S. Department of Housing and Urban Development (HUD) was tasked
with forming a benchmark for severely burdened households. This measure is for households whose
housing costs account for half or more of their income.
These housing concerns become even worse when you realize the favorable economic trends in New
York City and its surrounding areas. Over last decade, 2007-2017, the median household income for

Broome County
154 Community Health Assessment 2019-2024
renters in New York increased by $1,042 to $42,073. That increase equals about a 2.5% increase. For
homeowners their median household income increased by $1,800 to reach a figure of $89,035. When
you compare Broome County to New York State and National values the differences are apparent.
Broome County median household income is $49,064 compared to the New York State’s Median
household income of $66,426. Income is an important variable in calculating housing burden but there
are other factors affecting one’s ability to afford housing such as taxes and utilities which vary across the
different areas of New York State.
When you separate the renter and homeowner household incomes the disparities become more
noticeable. Only 56.9% occupied housing units in Broome County reporting household incomes that
exceed $35,000. For New York State the average increases to 69.2% of housing units making more than
$35,000. These two values are still behind the national average of 76.7% of housing units reporting more
than $35,000 in income. When you limit the households to only represent renters the differences
become even more apparent. Of the renter-occupied households in Broome County only 38% of those
households reported having a household income above $35,000. New York State had 55% of its rented
units reporting income above $35K with the national average dipping slightly to 52.1%. Depending on
the area’s distribution of households the burden might be different which is why it is important to know
more about your area’s housing information.
Housing affordability is measured in relation to household income so changes in incomes for renters and
homeowners can have a significant impact on affordability. Homeowners in Broome County have a
median household income of $64,205 which is $20,000 less than the New York State reported median
value of $86,273. When compared to the national and New York State averages Renters in Broome
County have a median household income of $24,911 while the corresponding New York State value is
$40,357. These differences in incomes and resources available must be considered when Broome
County’s place among New York State counties is explained. Across the board for renters and
homeowners alike a lower median household income is reported and is significantly less than State and
the metropolitan area median incomes.
Both low and high-income households could devote larges percentages of their income to housing costs,
but lower income individuals are more likely to suffer harmful impacts from the fiscal burden. Housing
cost burdens can increase the financial stress for individuals and households. All aspects of life are
affected. It is harder to put funds aside for emergency, education, savings or retirement. Some
households could be facing eviction or other repercussions. The fiscal stress can conclude in households
moving to lower-cost locations which could have broader implications for New York State’s economy.
While rental and homeowner costs are generally thought to be higher in downstate regions, Broome
County has not been exempt from this issue as housing costs have been on the rise in the Southern Tier.
When comparing housing costs between renters and homeowners the figures appear to favor the belief
that housing costs decrease as you head away from the New York metropolitan area. Median rental
costs which include rent and utilities were less than the national average and almost half the rental costs
of New York State. Broome County median monthly costs to renters was reported as $734 where New
York State had a median rental cost of $1200. The same trend is seen in homeowner households that do
not have a mortgage. The median owner costs for Broome County is $495 which is slightly above the
national median value of $474. New York State reported homeowners have a median cost of $728. The
surprise is in homeowners in Broom County who are currently paying mortgage. Homeowners report a

Broome County
Community Health Assessment 2019-2024 155
median cost of $2,064 which is a sizable difference to the median cost of $1,185 reported for the New
York State homeowners who
Rural and urban areas have been affected just as hard as the income and resource gaps become more
pronounced. Broome county had the second highest percentage of rental households above the
Affordability Threshold in the Southern Tier with 49.9% of rental households. The highest rate in the
Southern Tier area was Tompkins with 54.8% of rental households being at or above the affordability
threshold. For New York State Tompkins county and Broome county are part of the top 15 counties in
percentages of renter households above the affordability threshold. For the Severe cost burden Broome
had the second highest percentage of households with 29% of rental households reporting severe cost
burden with Tompkins having a 33.3% of renter households reporting Severe cost burden. Broome and
Tompkins are part of the top ten counties with Severe cost burden percentages relating to renter-
occupied households. Renters in Broome County are a highly burdened group that is being
disproportionately affected by housing costs.
For homeowner-occupied households the Southern Tier area was in the bottom groupings for both
housing burden measures. 20.2% of homeowner households were reported as being above the
affordability threshold. 7.2% of owners were reported experiencing severe cost burden. Although
Broome county is not the top 15 counties for owner-occupied households experiencing housing
burdens, the 20.2% of owner-occupied households experiencing this burden represents a significant
percentage of our county’s population. In 2017 54% of New York State households were classified as
homeowner-occupied. Broome County’s rate of 65.7% is not only an increase compared to the State
average but is also larger than the national average of 63.8%. Another factor is the difference in
property values when you head further upstate. For New York State 16.1% of its owner-occupied units
have property values under $100,000. The national average for owner units valued under $100,000 is
22.2%. Broome County has double those values with 41.8% of owner units being valued under $100,000.
Although we have a higher percentage of homeowners compared to other parts of New York State our
property values do not aide homeowners in giving them that extra capital like downstate properties do.
Homeowners in Broome county represent a large percentage of the county’s households which
reinforces the cause of concern and interventions to both homeowners and renters.
Opportunity
The Southern Tier benefits from a strategic location nestled in Upstate New York. Located in the
Southern Tier are multiple world-renowned colleges and universities which provide a robust pipeline of
Science, technology, education and mathematic (STEM) graduates. Add to that the thousands of farms
and top manufacturers in the area and it becomes clear why the state is investing in the area. The
Southern Tier has a strong foundation to continue its economic growth with the assistance of New York
State programs. Broome County has an alluring appeal for different demographics. Broome County
housing costs are dwarfed by the expensive rates observed in the NYC metropolitan area. Broome
County boasts a metropolitan area of over a quarter-million people.
With the growth of the universities in the Southern Tier we have witnessed a larger percentage of
students and young professionals being retained in the area which only adds to the appeal. This is an
alluring characteristic for investors. Of the 79,000 occupied household units in Broome County 34.3% or
28,000 households are rentals. This number is higher in the Binghamton metropolitan area as a myriad
of professional workers, students, and families compromise the city’s inhabitants.

Broome County
156 Community Health Assessment 2019-2024
The government has provided financial incentives to help reach this demand. For homeowners and
investors interested in renting or developing rental units there are tax credits, subsidy programs, and
grants that can aid in diminishing costs. Subsidies from the state help renters and the owners alike. The
rent revenue stream is not interrupted while financial stress is alleviated for the renters. Rental
assistance is offered by many different programs which include Section 8 housing vouchers, Housing
assistance from the state, and the USDA Rental assistance for rural units. Since the elderly demographic
is a significant percentage of Broome County they also have their own programs for assistance. For
overburdened elderly and disabled households, the department of HUD has Section 202 and 811
programs for assistance.
For current and prospective homeowners, the Federal and State government provide programs and
grants to those who are eligible so that they can acquire affordable housing. Multiple programs by the
HUD administration and housing authority of Broome County work to empower Broome residents by
aiding income eligible households and persons to become homeowners. It is important to note that the
HUD administration and Housing department adds no local tax burden and is fully funded by HOME and
CDBG annual block grants. This entity manages and monitors all housing rehabs for qualified
homeowners and works closely with affordable housing agencies to improve access to safe, sanitary,
and quality housing for income qualified tenants. Compared to the rest of the state Broome County has
a larger percentage of household units that are occupied by owners when compared to national, state
and metropolitan averages.
HUD entitlement Funds
o CDBG
CDBG program addresses a variety of community development needs that must
meet one of three national objectives: benefit low/moderate income persons;
eliminate/prevent slum and blight; address an urgent need that poses a threat
to the health/welfare of the community.
o Emergency Solutions grant
ESG program is there to help prevent individuals to enter the cycle of
homelessness and re-house homeless individuals into permanent housing
situations. Components of WESG include street outreach, emergency shelter,
homeless prevention, rapid re-housing, data collection via HUD mandated
homeless management information system
o Home investment partnership
The Home program is designed exclusively to create affordable housing for
income eligible persons.
HUD low-income housing tax credit program
o Provides tax credit to states which then offer them to developers of eligible low-income
housing projects.
Help continue to facilitate economic growth while improving living conditions
for the community
Improve health and appeal of the area
Applicable for all potential investors or homeowners
Appeal of affordable housing to for-profit investors.
Broome County
Community Health Assessment 2019-2024 157
o Can produce consistent, steady income from renters. In many housing markets they are
fully occupied dependable performers which can result in a safer investment that
conventional luxury housing.
Large population (students) with need for rental properties as well as
professionals in the area.
Growth of area alongside educational institutions, manufacturers, and growing cities.
Interventions (current)
Local services
o Broome Housing authority
Assists with public housing as well as information distribution
o HUD certified CHDO
Opportunities for Broome Inc.
receives funding assistance from the City, State, and Federal
governments to improve local housing conditions.
Has several low-income housing units
In 2015 Governor Cuomo started the Upstate Revitalization Initiative (URI) which is meant to focus on
growing and further developing upstate areas. The name giving to the URI winning plan for the area was
Southern Tier Soaring. It is play on words on the great expectations for the area.
Upstate Revitalization Initiative
o Create long-term regional plans
o ST strategic position.
o Southern Tier Soaring
URI-winning plan
Binghamton Gateway Project
o Front street homes renovated
o Aimed to create housing for low to moderate income while not sacrificing amenities.
Community Renewal Act/Grant; state initiative
o Most projects in Broome were financed through NYS Homes and Community Renewal
o Home (housing trust fund) Programs in Stueben, Tioga etc. counties
o Community development block grant in Tompkins and Broome
Projects overseen by First Ward Action Council
o First ward action council is a part of Southern Tier Soaring
Front Street renovations
o Next renovations are houses on Meadow street and Spring
Forest avenue
North and Crandall street renovations
o Funded the state house trust fund (Home), community
investment fund and 8 million in federal low-income housing
credit equity.
o Additional funding came from NYSERDA, broome county land
bank and the city of Binghamton
E.J apartments in Endwell
Broome County
158 Community Health Assessment 2019-2024
o Funded by the NYS HOME program, OPDD office, federal
historic tax credits and the NYS energy research and
development agency (NYSERDA)
Century Sunrise: Mix-income communities
o Private venture but still has mixed income so it is an option for lower SES households
Possible Interventions
After the Crandall Street project is completed, Binghamton also will be working on a housing
project on the North Side. According to Leonard Skrill, the assistant commissioner of NYS Homes
and Community Renewal, there are 15 ongoing projects in the Southern Tier, including three
projects in Elmira, four in Tompkins County and two in Steuben County.
o $1.1 million community development block grants, $12.8 million in low income tax
credit NYS Homes and Community Renewal, $1.3 million from HCR’s Housing Trust Fund
corporation, $2 million from Rural and Community investment fund, $2.3 in equity
raised by brownfield tax credits allocated by the DEC, $100,000 from the City of
Binghamton Home and $48,000 incentive grant from New York State Energy Research
and Development Authority.
Overview of Community Health Improvement Plan Strategies
Look over the documents coming in regarding the CHIP interventions, initiatives, and measures.
I need to associate certain government agencies/department with proving housing assistance,
consultation, or direction.
Economic development related to housing security
o How increased employment opportunities, increased social services due to the growth
of the area, alongside any independent actions by the partners.
Transportation Troubles
Transportation has been identified by clients, caregivers, and providers alike as well as in the
professional literature as a barrier to accessing needed healthcare services. This barrier to care can lead
to missed medical appointments or delays in diagnostic testing, gaps in treatment and poor adherence,
delays in obtaining prescription medications, poor management of chronic diseases resulting
preventable exacerbations, and irreversible progression of conditions that would be curable if caught
early. The net effects of these disruptions to clinical care are poor health outcomes for clients and
increased costs to the healthcare system.
Transportation barriers are thought to disproportionately affect economically disadvantaged individuals
who cannot afford to own or operate a private vehicle, those with disabilities who require specialized
equipment or transport, those with functional deficits who may limit when or how they drive to care,
suburban and rural residents for whom public transportation is not available and who bear a heavier
cost burden due to travel distances, and those who are socially isolated and do not have the networks of
family and friends to assist with rides. These vulnerabilities may exist not only for the client in need
healthcare services but also for caregivers, family members, and friends.

Broome County
Community Health Assessment 2019-2024 159
To examine these issues in our community, HealthLinkNY, the Population Health Improvement Program
agency, funded a pilot project to examine transportation vulnerability in the Southern Tier region. The
goals of the project were two-fold: (1) to collect data on transportation needs and (2) to create a referral
mechanism to connect patients with identified transportation vulnerability to mobility management
services to help them keep their healthcare appointments. A select set of slides detailing the key
findings of the pilot project are included in Appendix G. These results were presented to the
Transportation Workgroup, a sub-committee of the Population Health Improvement Program at
HealtheConnections (formerly HealthLinkNY), and prompted further discussion of the benefits,
limitations, scalability, sustainability, and implications of the findings for strategic planning related to
reducing transportation barriers to care.
The project also involved a large media campaign to “spread the word” about availability of
transportation services and resources in the community. Getthere, the mobility management
organization for the southcentral region of NY, also had a prominent presence on the Rural Health
Network website. And, Thompkins 2-1-1, the mobility management organization for Thompkins County
had a prominent presence on the Human Services Coalition website.
During check-in, either the patient or caregiver received a brief questionnaire, which was returned to
the office staff at checkout. The anonymous survey collected the following information: survey
respondent (e.g., client, family member), demographic (e.g., age, gender), insurance (status, type),
geographic (e.g., zip code, rurality), travel (i.e., mode of transport to/from appointment), trouble with
transportation in the past, and need for transportation to their next appointment. At checkout, the
office staff asked two key questions: (1) Did the client have any transportation concerns about getting to
their next appointment? And for those who answered affirmatively, (2) Would the client like to receive a
call about transportation assistance options for your next appointment? If indicated, the office staff
made either a “hard referral” faxing the client’s information to mobility management services, or a “soft
referral” providing the client with information on accessing mobility management services. In response
to any inquiry, mobility management serviced the referral and flagged it as part of the pilot project.
Five pilot sites participated in the project including three different hospital systems with representation
from hospital clinics, primary care, pediatrics, and Cornerstone, the Federally Qualified Health Center.
The sites were located in five different contiguous counties in the Southern Tier and Central region of
NYS. A total of 3,622 surveys were collected over a 9-month period between June 2017 and February
2018. Data were collected in two formats: (a) Survey responses were entered into an Access database
and exported into Excel spreadsheets, and (b) as hard copies with surveys entered manually by a
research assistant on the project.
The data were analyzed by pilot site, county, rurality, and age group. Key findings from this pilot study
revealed differences in transportation vulnerability across each of these variables. The demographics
primarily reflected the characteristics of the population served by each pilot site.
Cornerstone had the highest proportion of Medicare clients (69%). Since the clinic is located in
an urban area of Binghamton, these clients had the largest proportion of survey respondents
who walked or rode a bicycle to their appointment (39%). This group also had high
transportation vulnerability with 38% reporting difficulty in the past as well as getting to their
next appointment.

Broome County
160 Community Health Assessment 2019-2024
Individuals from rural Tioga County also had a high proportion of Medicaid survey respondents
(41%) but only reported moderate transportation vulnerability - 21% reported difficulty in the
past and 12% had difficulty getting to their next appointment. A substantial proportion used a
medivan/taxi to get to their current appointment (11%)
Individuals from the rural areas of Thompkins County had a larger proportion of older
individuals (48% Medicare) with high levels of transportation vulnerability – 36% reporting
difficulty in the past and 26% had difficulty getting to their next appointment. A substantial
proportion used a medivan/taxi to get to their current appointment (9%)
Pilot sites located in suburban areas of Chenango County had a larger proportion of clients with
private insurance (>60% for two sites) and younger clients (pediatric) and had low levels of
transportation vulnerability (3-5% reported difficulty in the past and 2-3% had difficulty getting
to their next appointment. Most drove themselves to get to their current appointment (50-
70%).
Significant differences were noted in transportation vulnerability based on age and with the largest
proportion of individuals who reported difficulty in the past, difficulty getting to their next appointment,
and requesting referral services. Females were more likely to experience transportation vulnerability, as
were individuals in the 30 to 64 age group. Interestingly, no significant differences were found for self-
reported geographic residence across the rural-suburban-urban continuum.
Analysis of referrals to the two mobility management organizations involved in the project revealed a
proportionate number of hard and soft referrals relative to the number of individuals who requested
them. Utilization of the services however was low. It is unclear whether this finding is spurious due to
insufficient data collection or due to clients finding alternative options for getting to their next
appointment. Clearly, the mechanism for linking records of clinical care and transportation needs is
lacking. One potential solution is a population health platform currently being implemented by Care
Compass Network in which community based organizations and healthcare providers can share
information on clients through a common client care plan and would be able to manage transportation
needs and referrals through this portal.
Follow-up discussion considered the acceptability of services. Feedback from clients using mobility
management services reported their cultural aversion to using public transportation citing loss of
independence, inconvenience, and accommodation limitations. A potential solution discussed was the
cost of bring clients to services versus bring the services to the client. Most of the healthcare systems
are in the process of establishing telehealth services. This option can provide timely access at an early
stage of a health issue and elicit a prompt clinical response to avoid the need for spending the time and
money to travel distances for appointments.
Discussion also explored possible reasons for the higher transportation vulnerability among middle-aged
adults as compared to older adults. One hypothesis was that older individuals may have already adapted
to limitations in getting to appointments either by developing a network of people and resources on
which they could rely to get to their appointments (many reported getting to their current appointment
by getting a ride with someone else) or by limiting their activity. Perhaps for the middle-aged adult who
may be experiencing significant chronic health issues for the first time in their lives, they have not
developed the same coping behaviors and social networks in relation to their transportation needs as

Broome County
Community Health Assessment 2019-2024 161
older adults. They may be more aware of and sensitized to their vulnerability because of a transition in
their lives from robust independence to needing to accept help and assistance.
Finally, some of the discussion focused on aging in place. Mobility management services include not only
transportation to receive clinical care, but also for picking up prescriptions, grocery shopping, and other
instrumental activities of daily living. Many community members are not aware of the range of services
available to them. In addition, in the age of online shopping and home delivery, there is emerging
technology that can provide services and deliver goods without having to leave home. Self-driving cars
and drones are two examples. Discussion then turned to, well if people don’t need to leave their home,
what impact will that have on social isolation? Is it possible to design housing and active living
communities that can overcome some of the transportation issues resulting from the way residential
areas are designed and community resources geographically distributed? These questions remain
unanswered.
The role of social factors in accessing healthcare services were evident in this pilot project. The findings
strongly support an association between socioeconomic resources and transportation vulnerability. As
the population of Broome County ages, the issues around “getting there” will become manifest and
have a more prominent role in how care is managed and the extent to which effective clinical
management can be optimized and the most favorable health outcomes can be realized.
Burdens of the Uninsured
The US Census Bureau considers individuals to be “uninsured” if, for the entire year, they were not
covered by any type of health insurance. However, the Kaiser Family Foundation notes that 27% of
individuals without health insurance in 2006 were without health insurance for less than a year,
suggesting rates may be even higher than reported by the U.S. Census Bureau.
Multiple barriers exist to obtaining health insurance including opportunities for full-time employment in
that offer such benefits. While improving, awareness of existing programs remains a barrier to
accessing publicly-funded insurance. This issue is particularly relevant for uninsured children who live in
working families. New York State has a variety of publicly funded programs and collaborates with
employers to educate the community about existing programs. Additionally, with the advent of
facilitated enrollment, access to locations where enrollment can occur has improved. Facilitated
enrollment has also streamlined the process, but staff acknowledges that the form remains lengthy,
questions can appear ambiguous, and obtaining the necessary written documents can be challenging.
Not having health insurance is a substantial health issue as people are less likely to receive preventive
care and more likely to be hospitalized for conditions that could have been prevented. The financial
burden strains family as well as hospital budgets. Uninsured families, who already struggle financially to
meet basic needs, may be financially devastated by medical bills, even for a minor problem; and
hospital/provider systems bear the increasing cost of charitable care.
Information on Health Insurance Coverage can be found in Appendix G24-G32. The percent of uninsured
adults in Broome County was estimated to be 4.8% in 2017, translating to 4,495 persons. The uninsured

Broome County
162 Community Health Assessment 2019-2024
rate has dropped significantly since the last community health assessment was conducted. At that time,
it was estimated 10.5% of the population was uninsured, equating to 20,500 individuals going without
health insurance. In 2010, a historic shift transpired with health insurance coverage in the United States.
The Affordable Care Act was passed and a new government sponsored health insurance model was
initiated in September 2013. For New York State residents, New York opened its health plan
Marketplace, NY State of Health, in October 2013. The Marketplace’s one stop health insurance
experience offers high quality comprehensive health plans. NY State of Health is the only place where
consumers can qualify to get help paying for coverage through premium discounts or tax credits. Eligible
New Yorkers can also enroll in Medicaid, Child Health Plus and the Essential Plan through the
Marketplace all year. In Broome County there are two NY State of Health facilitated enrollment agencies
for the Marketplace: Mothers and Babies Perinatal Network and the Southern Tier Independence
Center.
Examining the demographic breakdown of Broome County residents and health insurance coverage is as
follows; the age group with the highest uninsured rate is that of the 19-64, males have a higher
uninsured percentage than do females, individuals with household incomes of $25,000 or less have a
higher rate of being uninsured. Other demographic correlations depicting lack of health insurance
coverage are seen in populations that have a low poverty threshold and those that classify their race as
African American also seem to have a higher uninsured rate. Over all, from 2000 to 2016 Broome County
has seen a steady increase in adults age 18-64 that who health insurance coverage. Broome County
residents report that 87.6% have a regular healthcare provider and 93.4 % report having coverage.
Broome County is higher than NYS in both of these categories. As hopeful as that sounds, there is still
7.2% of the Broome County population that forgoes care because they are unable to afford to pay for it.
(Appendix G25). As for children over the age of 19 in Broome County, there also has been a steady
increase in health insurance coverage with 97.5% of children reported to be insured, ranking Broome in
the highest quartile of NYS.

Broome County
Community Health Assessment 2019-2024 163
D. Broome County Community Health Assessment 2019-2024 Process
Collaborative Partners
The 2019-2024 Community Health Assessment (CHA) has involved a variety of partners from a broad
cross-section of community and human services agencies in Broome County (Appendix G1).The
committee has benefitted tremendously from a stable membership of committed leaders as well as
inclusion of new members who brought fresh perspectives to the work of the group.
In collaboration with the Public Health Director and the CHA Coordinator, these Steering Committee
members provided the leadership for guiding selection of the mutually derived priorities. The Steering
Committee’s work was also supported by a Supervising Public Health Educator who led the chronic
disease risk reduction interventions and who served as health department liaison on the mental health
and prescription drug initiatives.
Health department senior staff, which included the division directors and department supervisors, was
updated on the ongoing activities of the Steering Committee and CHA process. In addition, they
provided input by making in-house data available and keeping the CHA Coordinator apprised of relevant
changes to programs and services.
In May 2019, Broome County Health Department was awarded a grant from HealtheConnections as part
of the Population Health Improvement Program (PHIP) New York State contract for the Southern Tier
region. Grant funds were used to hire three temporary, part-time Public Health Representatives to
provide support in updating the CHA and CHIP. These individuals were recruited via the newly-founded
Binghamton University Master of Public Health (MPH) program. Partnership with the PHIP and MPH
program was crucial for the completion of the CHA and CHIP documents.
The core support team consisted of the Broome County Health Department Director and the Medical
Director as well as administrative, technical, and interdisciplinary planning support team members.
Collaborative Efforts
Since the last Community Health Assessment, the Steering Committee met on a monthly basis. The
Steering Committee serves as an active workgroup not only monitoring progress on implementation of
the previous Community Health Improvement Plan but also actively seeking new opportunities for
collaboration including funding for evidence-based and promising strategies to address community
needs.
Committee meetings focused on re-evaluating the health status of the county and conducting specific
activities to inform the 2019-2024 Community Health Assessment. The meetings were chaired by the
CHA Coordinator and attendance averaged about 10 members per meeting. Minutes were taken by

Broome County
164 Community Health Assessment 2019-2024
Broome County Health Department staff members. Agendas and meeting minutes were e-mailed to
committee members. In addition, all agendas, meeting minutes, and materials are electronically
archived on the Broome County Health Department shared drive as a formal record of the CHA process.
Bi-weekly meetings between the CHA Coordinator and BCHD staff members were held to assess
progress and to plan for upcoming CHA meetings and activities. Between meetings, Steering Committee
members completed assessment tools and surveys and during meetings contributed to interpretation of
data analyses, providing a contextual understanding of issues underlying observed differences in the
occurrence and rates of disease among residents of the county.
Vision
The vision statement developed by the Steering Committee for the 2010-2013 Community Health
Assessment, and reaffirmed for the 2013-17 Community Health Assessment, continues to reflect the
ongoing work of the Steering Committee.
Community Themes & Strengths Assessment
The Community Themes and Strengths assessment examines topics of interest, engages the community
in relation to their perceptions about quality of life, and explores community assets. A series of four
Community Surveys were conducted via Survey Monkey. These surveys were provided to community
organizations via an email link as well as in portable document format (PDF). Partners were asked to
engage their respective service sectors in completing the surveys and a link to the survey was made
available on the county website.
Particular effort was invested in surveying specific vulnerable groups. The surveys were conducted at
the Dr. Garabed A. Fattal Community Free Clinic where uninsured residents obtain free health services.
In addition, participation was obtained from nearly every senior center in the county to reach rural
elders. All four surveys asked residents about their mental and physical health and overall general
health. Each survey asked participants about topics exclusive to that survey, such as their use of medical,
dental or mental health services; their perceptions about quality of life in the county; concerns and
issues about their community being a safe and healthy place to live; the adequacy of health services
available; and their prioritization of health issues. A summary of the results from this survey appear in
Appendices G46-G65 and are presented in narrative further below.
Community Health Status Assessment
The Community Health Status Assessment examines the health status, quality of life, and risk factors for
disease present in the community. A variety of data sources were used for this assessment including: the

Broome County
Community Health Assessment 2019-2024 165
NYS Prevention Agenda Indicators for Tracking Public Health Priorities, 2019-2024; the County Health
Indicators by Race/Ethnicity (CHIRE); the Community Health Indicators Reports (CHIRS); the County
Health Assessment Indicators (CHAI); the Expanded Behavioral Risk Factor Surveillance System (BRFSS);
and data from the Statewide Planning and Research Cooperative System (SPARCS). These data were
publicly available from the New York State Department of Health website. In addition, other county level
data available online such as from the Census Bureau were downloaded, analyzed, and reviewed by the
Steering Committee with comparisons made to NYS Prevention Agenda 2019 goals.
Furthermore, Steering Committee members presented information about their agency, the populations
they serve, the services they provide, and identified needs and gaps in services during meetings.
Steering Committee members were asked to provide the group with recent assessments or data from
their organization that would inform the process. Annual reports and other publications from
community partners and agencies that service specific population sectors were compiled and reviewed.
Steering Committee members readily shared materials and information.
Local Public Health System Assessment
The Local Public Health Assessment measures the capacity of the local public health system to conduct
essential public health services. The local public health system is viewed as all organizations and entities
within the community that contribute to the public's health and not limited to the local public health
department.
To assess the scope of services provided by community organizations
in relation to the Prevention Agenda priorities, community
organizations were asked to complete the tables in Appendices H1
and H2, indicating how their programming aligned with Prevention
Agenda 2019-2024 priority areas, focus areas, goals and objectives.
The tables were disseminated via email across healthcare
organizations, county governmental departments, higher education,
community-based organizations, and non-governmental agencies. The
information provided by partners via these tables was used to select Community Health Improvement
Plan interventions and metrics.
Forces of Change Assessment
The Forces of Change Assessment identifies factors that are currently affecting or may affect the
community or local public health system. Typically, these factors involve issues that are broader than
the community such as domestic economic and healthcare policy, or uncontrollable elements such as
catastrophic events, or transformations in societal attitudes or values. These factors are important to
identify because they may influence health outcomes. Awareness of these forces can help public health
leaders to proactively anticipate change and formulate a managed response. Further, such analysis can

Broome County
166 Community Health Assessment 2019-2024
provide insight into the gaps that exist between the current situation and ideal circumstances, and
thereby inform public health planning.
Several methods were used for this assessment including analysis of the narrative responses from the
Community Survey, Focus Area Ranking Tool and breakout session themes from the CHA Symposium,
informal discussions with key community leaders, and examination of local headlines as well as national
news events. The data obtained through these activities are woven into discussions within relevant
sections of this report. Some topics were identified as more pressing issues in Broome County. These
key emerging issues are: age friendly communities, the opioid epidemic, vaping and e-cigarette use,
housing, transportation, and food insecurity. They are described in-depth in Section 3c: Emerging Issues.
Development of the Community Service Plans & Community Health Improvement
Plan
Representatives from both area hospital systems served on the Steering Committee. Our Lady of
Lourdes developed its own Community Service Plan (CSP), but endorsed the Broome County Community
Health Improvement Plan (CHIP) and assisted with its development. In partnership with the Steering
Committee, UHS submitted the CHIP as its CSP.
Committee meetings focused on assessment information and data analyses, which were presented and
discussed in detail during meetings. Representatives from area agencies on the Steering Committee also
presented information specific to their target populations and service sector. This process included
quantitative reports of local data as well as qualitative evidence derived from personal experience and
expert knowledge. The information resources and rich discussions provided the basis for examining the
public health priorities for the county. This process is discussed separately in Section 4. The tool and
scoring results appear in Appendix E.
Several activities supported development of the Community Health Improvement Plan (CHIP) and
Community Service Plans (CSPs). First, attendees of the CHA Symposium in April 2019 and CHA Steering
Committee members voted on the Prevention Agenda Priority areas they felt most important for
Broome County using the Focus Area Ranking Tool (Appendix H3). Breakout session notes from the
Symposium were also analyzed for key themes. Results from the Focus Area Ranking Tool and breakout
session key themes guided discussion and selection of two public health priority areas from the
Prevention Agenda 2019-2024.
To determine objectives and interventions for the CHIP, Steering Committee members completed the
two tables in Appendices H1 and H2 , indicating how their organization’s current programming aligned
with selected Prevention Agenda 2019-2024 focus areas, goals and objectives of the selected priority
areas. The resulting collection of local interventions served as an inventory for the Steering Committee
to explore current strategies being used and to consider additional opportunities for action. These
completed documents provided a framework for thoughtful consideration of and discussions about
evidence-based strategies. Collated responses to these tables was shared with Steering Committee
members and was the basis for developing the work plan.

Broome County
Community Health Assessment 2019-2024 167
Once the Steering Committee determined the priority areas on which to focus, a template was
developed for the Community Health Improvement Plan (CHIP). The template was populated with
information solicited from members of the Steering Committee and included identification of
intervention strategies to be used, potential activities or action items, key stakeholders, and possible
metrics to use for measuring process and outcomes. This information provided the data elements for
the initial draft of the CHIP. The draft document was distributed prior to the November Steering
Committee meeting and discussed. The plan was refined over the next month based on Steering
Committee input. The final version of the CHIP was unanimously approved by the Steering Committee.
This CHIP will serve as the basis for ongoing Steering Committee meetings during which it will likely
undergo further refinement. As the CHIP is implemented and evaluated, specific actions/interventions
may be modified and new ones added in a continuous and dynamic plan, do, check, act (PDCA) cycle.
The Steering Committee will continue to meet on a monthly basis to assess progress to date and adapt
the CHIP as circumstances direct.
Community Health Assessment Symposium
The Symposium was conceived of by the CHA Steering Committee in spring of 2018 as a way for
stakeholders from various sectors to engage with local, regional, and state level data, in order to make
data-informed prioritizations of local health issues. A Symposium sub-committee was convened in
August 2018 to plan and execute the Symposium, which occurred April 12, 2019.
All CHA Steering Committee members were invited to the Symposium, as were other organizations
whose work aligns with the five NYS Prevention Agenda Priority Areas. Invitees representing
organizations were each asked to invite one client served by their organization, who could represent the
community. In total, 40 individuals from 17 organizations attended (Appendix H4). None brought a
client.
The Symposium was separated into a morning and afternoon session (Appendix H5). The morning
session consisted of presentations by local organizations. The opening keynote by Dr. Yvonne Johnston
provided valuable context for the current state of public health in Broome County and the frameworks
for the CHA and Prevention Agenda (Appendix H6). Each subsequent presenter shared the work their
organization is doing to address public health in Broome County and data collected by their
organizations. The data presented broadly illustrated current public health issues, social determinants of
health, health disparities, and progress being made by specific programs. The Broome County
Community Health Assessment Community Survey results were also presented during the morning
session.
The afternoon session consisted of five breakout sessions. Each breakout session aligned with one of the
five New York State Prevention Agenda 2019-2024 priority areas. Symposium attendees cycled through
each of the five breakout sessions, which lasted 20 minutes per session. A scribe took notes during each
session. Local subject matter experts led the breakout sessions, facilitating discussion about their
priority area around the following criteria:
- Total health care costs

Broome County
168 Community Health Assessment 2019-2024
- Absolute number of individuals affected
- Worsening trend over the past five years
- Broome County performance compared to US/ NYS health goals
- Presence of health disparities
- Measurability/ indicators to monitor change
- Opportunity to continue current, local interventions
- Feasibility for potential intervention
- Availability of funding for initiative
- Social determinants of health: transportation, housing, socio-economic status, education and
employment
At the end of the Symposium, attendees used the Focus Area Ranking Tool (Appendix H3) to rank the
top five New York State Prevention Agenda 2019-2024 focus areas they felt most important. Attendees
were given a list of all 20 New York State Prevention Agenda 2019-2024 focus areas separated by
priority area and asked to rank only their top five in order of importance, with 1 being the most
important and five being the least important. They were instructed to base their ranking on the data
presentations and breakout sessions during the Symposium.
Symposium Data
Scoring the Focus Area Ranking Tool
Unweighted Totals
For each of the 20 focus areas, the total number of votes for each ranking (e.g. 1, 2, 3, 4, 5) was added.
These totals were then added together for each focus area to obtain the Unweighted Total for each
focus area (Appendix H7).
Weighted Totals
Being that there were 20 focus areas in total, and that a ranking of 1 was considered most important of
the top five focus areas and a ranking of 5 was least important of the top five focus areas, weights were
assigned to numerical rankings as follows:
- 1- weight of 1.0
- 2- weight of 0.95
- 3- weight of 0.90
- 4- weight of 0.85
- 5- weight of 0.80
For each focus area, the unweighted total for each ranking was multiplied by its respective weight as
described above to obtain the Weighted Total for each focus area (Appendix H7).
Results for the Focus Area Ranking Tool
Analysis of the “importance” assigned to each focus area, as obtained through weighted and
unweighted totals, was used to generate the Top 5 Focus Areas list (Appendix H8 “Focus Area Ranking
Broome County
Community Health Assessment 2019-2024 169
Tool Results”). Notably, the same five focus areas appeared in the same order when ranked by their
weighted and unweighted totals (Appendix H8).
Themes from Breakout Discussions
Scribes took notes during each breakout session. Notes from each session were aggregated and a
content analysis was performed to identify key themes in each of the five breakout sessions. Of note,
social determinants, health across the lifespan, and educating the general public about availability of
resources all emerged as themes in multiple breakout sessions (Appendix H8 “Breakout Group
Themes”).
Community Survey
Responses from the Community Surveys are located in Appendix G46-G65. There were four surveys
which addressed the topics of community health concerns (Survey #1), community health resources
(Survey #2), quality of life (Survey #3), and environmental quality (Survey #4). The number of responses
to each survey were 348 to Survey #1, 67 to Survey #2, 380 to Survey #3 and #259 to Survey #4.
Demographic Information
The same ten demographic questions were asked on all four surveys. The majority of respondents were
female (70.7%) and White, non-Hispanic (83.2%) which is reflective of the county’s demography and
higher response rate for females (Appendices G46, G48). All age groups were represented with the
modal age group 50 to 59 years old (Appendix G47).
When asked about highest education level achieved, 8.4% of respondents indicated that they had less
than a high school education, 5.8% had a high school education, and 78.4% had more than a high school
education (Appendix G49). Most respondents were employed in the last year, with 60.9% employed full
time and 10.5% employed part time. Others indicated that they were either retired (16.7%),
unemployed (2.7%) or a stay-at-home parent or caregiver (1.3%) (Appendix G50).
When asked about disability status, 10.9% of respondents indicated they have a non-developmental
disability and 1.1% answered that they have an intellectual disability (Appendix G51). Most respondents
have employer-based insurance (67.9%), while 17.5% have Medicare, 6.5% have Medicaid, 2.0% have
direct-purchase, 1.5 have military insurance, 7.4% have another insurance, and 1.5% are uninsured
(Appendix G52).
Twenty percent of chose not to provide information about household income. Seven percent reported
annual household incomes of less than $20,000, 8.2% reported $20,000 to $29,999, 16.6% reported
$30,000 to $49,999; 8.8% reported $50,000 to $59,999; 6.4% reported $60,000 to $69,999; 5.8%
reported $70,000 to $79,999; and 26.9% reported $80,000 or more (Appendix G53).
Almost one tenth (9.1%) did not live in the county (Appendix G54).
Survey #1: Community Health Concerns

Broome County
170 Community Health Assessment 2019-2024
This survey asked respondents about their perceptions of health concerns in Broome County. From a list
of 12 community health concerns, respondents were instructed to pick the top five that were of greatest
importance for Broome County and rank them from one (highest priority) to five (lowest priority).
Access to quality healthcare was the biggest community health concern identified. Of the 348
respondents to Survey #1, 233 ranked access to quality healthcare in their top five community health
concerns (Appendix G55). It also had the largest ranking of 1 (indicating greatest importance) with 107
rankings of 1. Behind access to quality healthcare, the other health concerns in the top five were mental
health, substance use (includes alcohol), developmental/ other disability services, and chronic disease
(Appendix G55).
This survey also asked respondents if a number of health conditions were concerns for them or
someone they know, and if they know where to go for help with that concern. The percent of
respondents concerned about a health condition was more or less the same as those knowing where to
go for help with it, for most conditions. Of note, although adult overweight/obesity, depression, and
mental health are each concerns for half of respondents, only 40%, 43.7%, and 41.1% (respectively)
know where to go for help with it (Appendix G56).
Survey #2: Community Health Resources
This survey asked about the formal and informal mechanisms by which individuals receive health
resource information and healthcare services. When asked about where they get information about
health resources in their community, a whopping 80.6% of respondents reported using the Internet
(Appendix G57). This suggests that education via websites, news outlets and social media may be an
effective way to reach Broome County residents regarding health resources.
With regards to engagement with the healthcare system, 79.1% of respondents reported having a
healthcare provider they see regularly (Appendix G58). Almost one third of respondents (31.3%, 21
individuals) needed healthcare in the last year but did not seek it (Appendix G59). The most often cited
reasons for this was too long of a wait time for an appointment (n=9), cost (n=6) and fear or distrust of
the healthcare system (n=5) (Appendix G60).
Respondents were also asked to rate the availability, accessibility and adequacy of various health and
human services including general health services; emergency services; maternal and child health
services; elder services; substance use services; disability services; food access and food insecurity; and
other/ community-based services. Of note, respondents rated the following services inadequate:
inpatient mental health services (47.8%), outpatient mental health services (44.8%), inpatient youth
mental health services (41.8%), transportation (41.8%), affordable housing (41.8%) and worksite
wellness programs (41.8%). Also of note is that respondents generally rated food access sites as
available/ sufficient: grocery stores (50.7%), farmers’ markets (43.3%) and food pantry/ emergency food
programs (47.8%) (Appendix G61).
Survey #3: Quality of Life
Survey #3 asked about activities, resources, and services that influence the quality of life for Broome
County residents. Respondents rated these items as poor, fair, good, very good or excellent (a “no
opinion” option was also included).

Broome County
Community Health Assessment 2019-2024 171
There were several noteworthy findings with regard to quality of life. One quarter (25.7%) of
participants rated the quality of economic opportunities in Broome County as poor, and an additional
40.1% rated them as fair. Broome County was also not rated favorably as a place to age (14.3% poor,
28.8% fair) or in terms of safety (14.4% poor, 29.6% fair). Overall quality of life was rated as satisfactory
(41.5% good, 22.5% very good). Respondents also rated Broome County as a satisfactory place to raise
children (34.3% good, 22.9% very good). Schools were rated very positively by respondents (39.7% good,
21.2% very good, 10.8% excellent), as was community engagement opportunities (36.5% good, 21.1%
very good, 8.1% excellent) and support during times of stress (13.6% excellent) (Appendix G62).
Survey #4: Environmental Quality
The final survey asked respondents about their perceptions of environmental quality in Broome County.
They did so by identifying myriad environmental issues as no problem, a small problem, a moderate
problem, a large problem, or a major problem (“I don’t know” was also an option).
Road maintenance/ repair emerged as a large issue; 25.5% of respondents said it was a large problem
and 50.6% said it was a major problem. Flooding (27.4% large problem, 30.1% major problem) and
abandoned buildings (24.3% large problem, 34.4% major problem) were also identified as issues
negatively impacting Broome County (Appendix G63).
The issues identified as least problematic from an environmental quality standpoint were inadequate
garbage collection (32.0% no problem, 32.4% small problem), noise pollution (22.8% no problem, 43.2%
small problem) and pedestrian crosswalks (31.3% no problem, 30.1% small problem) (Appendix G63).
Healthy Behaviors
In addition to the ten demographic questions on every survey, there were another two questions that
appeared on all four versions of the survey. The first asked, “What keeps you from making healthier
choices such as quitting smoking, exercising more, or eating healthier?” The second asked “What
changes would you like to see in Broome County to make it a healthier place to live?”
The most-frequently cited impediment to healthy choices was time constraints (13.9%). Lack of
willpower or motivation (8.3%), work-life balance (5.2%), and cost of healthy food (4.7%) were other
high-ranking barriers to making healthy choices. Roughly half of respondents did not answer this
question (Appendix G64).
When asked about changes that would make Broome County a healthier place, increased/ improved
mental health services was cited most often (10.3%). Improved walkability and bikability (7.4%); reduced
crime and improved neighborhood safety (7.0%); increased/ improved primary and general healthcare
services (6.3%); and reduced environmental impact and pollution (5.5%) followed. A total of 43.4% of
respondents did not answer this question Appendix G65).

Broome County
172 Community Health Assessment 2019-2024
Section Four — Local Health Priorities
A. Prevention Agenda Priorities
The following New York State Prevention Agenda 2019-2024 priority areas and goals were identified by
the Broome County Community Health Assessment Steering Committee as the local health priorities for
the Broome County Community Health Assessment 2019–2024:
1. Priority Area: Prevent Chronic Disease
Focus Area 1.: Healthy Eating and Food Insecurity
Goal #1: Increase access to healthy and affordable food and beverage choices
Goal #2: Increase skills and knowledge to support healthy food and beverage choices
Goal #3: Increase food security
Focus Area 2: Chronic Disease Preventative Care and Management
Goal #1: Increase cancer screening rates for breast, cervical, and colorectal
cancer
Goal #2: Increase early detection of cardiovascular disease, diabetes, prediabetes
and obesity
Goal #3: Promote evidenced-based care to prevent and manage chronic diseases
including asthma, arthritis, cardiovascular disease, diabetes and
prediabetes and obesity
2. Priority Area: Promote Well-Being and Prevent Mental and Substance Use Disorders
Focus Area 1: Mental and Substance Use Disorders Prevention
Goal #1: Prevent opioid and other substance misuse and deaths
Goal #2: Prevent and address adverse childhood experiences (ACES)
Goal #3: Reduce the prevalence of major depressive disorders
Goal #4: Prevent Suicides
Summary of the Process for Identification of Local Public Health Priorities
Local public health priorities were identified in an iterative process by the Steering Committee beginning
in April 2019 at the CHA Symposium event (described in Section 3d) and formalized at the November
2019 CHA Steering Committee meeting.
The CHA Steering Committee discussed data presented at the Symposium and data collected from the
Symposium (via the Focus Area Ranking Tool and breakout session themes) at their May 2019 meeting
(Appendix H8). The need to align selected CHA priority areas with other initiatives (e.g. DSRIP) and with
hospital Community Service Plans (CSPs) was indicated. The group spoke at length about how the social
determinants of health play into the top-ranking focus areas, and current Broome County initiatives to
address those issues and related social determinants of health.

Broome County
Community Health Assessment 2019-2024 173
At the June 2019 meeting, the CHA Steering Committee voted unanimously to select the priority area of
Prevent Chronic Disease for inclusion in the 2019-2024 Broome County Community Health Improvement
Plan. This decision was based in part on voting from the Symposium. Three of the five highest-ranking
focus areas are focus areas under the Prevent Chronic Disease priority area (Appendix H8). This decision
was also due to the fact that many programs already exist in Broome County to prevent or mediate
chronic disease, and which actively measure their performance. These programs and data gathered
from them can be utilized in the CHIP to measure progress towards selected metrics.
The CHA Steering Committee also voted unanimously to select the priority area of Promote Well-Being
and Prevent Mental and Substance Use Disorders. One of the remaining five highest-ranking focus areas
from the Symposium voting were related to this priority area (Appendix H8). In addition, local data
indicate that Broome County has been hard-hit by the opioid epidemic. Opioid-related hospitalizations,
emergency department visits and deaths are occurring at higher rates in Broome County than New York
State or the Southern Tier. In many cases, these rates have only worsened in the last four years.
The group also voted unanimously not to include the priority area Promote Healthy Women, Infants and
Children, but to address this topic via goals, objectives and interventions under the two selected priority
areas. Upon reviewing the themes from the Symposium breakout sessions, the Steering Committee
agreed that social determinants of health and adverse childhood experiences (ACEs) in particular are
critical to address during childhood, in order to yield positive long-term health outcomes.
Also of note, during the September 2019 meeting, the CHA Steering Committee discussed at length the
emerging public health issue of vaping and e-cigarettes, especially in light of recent, nationwide
unexplained vaping-associated pulmonary illness. Vape and e-cigarette use is of particular concern
among youth. Committee members agreed not to include this topic as a focus area within the CHIP,
since interventions are still fledgling and may not have a strong evidence base. Instead, this topic is
addressed as an “emerging public health issue” for the 2019-2024 CHA (Section 3c).
The Steering Committee considered the many current interventions taking place in Broome County for
inclusion in the CHIP during the October and November meetings. During this time, BCHD staff was also
in touch with community and healthcare organizations to glean further information on their activities
and metrics for evaluating progress (Appendix H1 and H2).
The final CHIP was presented at the December 2019 meeting. The Steering Committee voted
unanimously to accept it. With regards to the unselected priority areas of the Prevention Agenda, the
Steering Committee certainly appreciated that these three priority areas involve very important public
health issues. Even as we recognized their significance to the health of a community, other areas were
given higher priority for reasons described below.

Broome County
174 Community Health Assessment 2019-2024
HIGH PRIORITY: Promote Well-Being and Prevent Mental & Substance Use
Disorders- Mental and Substance Use Disorders Prevention
Since the 2013-17 CHA, mental and substance use disorders (especially opioid use) has transitioned from
an emerging public health issue to a public health crisis. Local data indicate that Broome County is
experiencing a higher rate of opioid-related hospitalizations, emergency department visits and deaths
than the Southern Tier or New York State. Many organizations have launched interventions to address
the growing opioid epidemic since the 2013-2017 CHA. These interventions have led to improvements in
opioid-prescribing practices, expansion of medication-assisted therapy (MAT) and increased naloxone
trainings for the general public. These and other established interventions currently exist and are
gathering data on their performance, which will allow the Steering Committee to measure progress
towards CHIP metrics.
HIGH PRIORITY: Prevent Chronic Diseases – Healthy Eating and Food Security
The Focus Area of “Reduce Obesity in Children and Adults” was one of selected focus areas of the 2013-
17 CHA. Since 2012, NYSDOH has revised Prevention Agenda focus areas and “Reduce Obesity in
Children and Adults” no longer exists. However, the overarching goal of the new “Healthy Eating and
Food Security” focus area is “Reduce obesity and the risk of chronic disease”.
There are currently several well-established interventions taking place in Broome County to address
healthy eating and food security. Community partners have been working in this area since at least 2012
when the 2013-2017 CHA was written; in many cases, organizations have been working on this issue for
even longer. This collection of evidence-based programs that already exist and are actively collecting
data in the community was part of the reason this focus area was selected for the 2019-2024 CHIP.
HIGH PRIORITY: Prevent Chronic Diseases – Chronic Disease Preventive Care and
Management
Broome County has a larger percent of the population aged 65 years or older (18.3%) than the Southern
Tier (17.8%) or New York State (15.4%) (National Center for Health Statistics Population Data, 2016). As
the population continues to age, the number of chronic diseases are expected to increase. Effective
chronic disease prevention and self-management has the potential to improve health outcomes and
decrease Medicare and Medicaid spending. There are a number of established chronic disease self-
management programs in Broome County, which will feed into the 2019-2024 CHIP.

Broome County
Community Health Assessment 2019-2024 175
Summary
Mental health disorders are medical conditions that affect cognition, mood, social relationships, coping,
and functional ability. Substance use disorders involve the recurrent use of drugs and alcohol, and can
disrupt an individual’s physical, mental, and social well-being. Prevention at the community level,
including interventions that address social determinants of health, will likely decrease the morbidity of
mental and substance use disorders overall. In particular, adverse childhood experiences (ACEs) can
have a lifelong impact on mental health and well-being and are thus a modifiable risk factor. Further,
mortality among people with substance use or mental health disorders can be reduced through
interventions delivered at the individual, community, and health systems level (e.g. Narcan trainings,
tobacco cessation).
Chronic disease refers to a medical condition that is persistent or recurrent. Cardiovascular disease and
diabetes are common chronic diseases responsible for a large proportion of hospitalizations that result
in excess morbidity for individuals and place a heavy cost burden on the healthcare system. A common
underlying and potentially modifiable risk factor for both conditions is diet. Unfortunately, a portion of
the population suffers from lack of knowledge of or access to healthy food choices. Thus, interventions
directed at improving dietary choices and increasing food security can prevent the onset of these
conditions and therefore offer an opportunity for primary prevention. For individuals with existent
disease, efforts are tertiary in nature and seek to maximize health and minimize short-term and long-
term complications that can result in expensive hospitalizations. Chronic disease self-management can
also have beneficial effects as tertiary prevention of disease morbidity for both cardiovascular disease
and diabetes.

Broome County
176 Community Health Assessment 2019-2024
Section Five — Opportunities for Action: The Community
Health Improvement Plan
This section presents the 2019-2024 Community Health Improvement Plan (CHIP) developed
collaboratively with community partners in a narrative format. A CHIP is a strategic roadmap for
addressing public health issues in a community. This CHIP was generated from the results of the
preceding Community Health Assessment (CHA) and was developed collaboratively with a broad
coalition of community partners and stakeholders. The CHIP operationalizes the Broome County vision
for maximizing the opportunity for all people to take responsibility for their own well-being and achieve
their optimal quality of life. And, the CHIP details how our local public health department and our
community will work together to improve the health of Broome County residents.
In addition to making the CHA planning process explicit and the ensuing wrokplan available to the
community in this document, a separate spreadsheet will be simultaneously submitted to NYS
Department of Health and this file includes all of the detailed information below. This format provides
New York State Department of Health with a data collection tool that can be used across all 62 counties
in NYS to assess the CHA/CHIP planning that has occurred over the intervening year or more of planning
and conducting the CHA and developing the CHIP. This format is also used for monitoring ongoing
assessments of the process and progress toward implementation the CHIP as well as evaluation of
stated objectives and achievement of defined goals.
Priority Area #1: Prevent Chronic Disease
Focus Area #1: Healthy Eating and Food Security
Goals: 1.0 Reduce obesity and the risk of chronic disease, 1.1 Increase access to healthy and
affordable foods and beverages, 1.2 Increase skills and knowledge to support healthy food and
beverage choices
According to the Centers for Control and Prevention (CDC), obesity and overweight are the second
leading cause of preventable death in the United States (US), which may quickly top tobacco as the
leading preventable cause of death. The CDC also states by the year 2050, if obesity trends continue as
they are, life expectancy in the US is predicted to be shortened by 2- 5 years. Obesity is a risk factor for
many chronic conditions including high blood pressure, high cholesterol, stroke, heart disease, type 2
diabetes, asthma, some cancers, and osteoarthritis. Alarmingly, these conditions are now appearing in
adolescents and children. Currently, the percent of adults who are obese in Broome County is 25.7%,
which is higher than the NYS Prevention Agenda target. The percent of children and adolescents who
are obese in Broome County is 17.7%, which is higher than the rest of the state and the NYS Prevention
Agenda 2 target 16.7% (2016 NYS Expanded Behavioral Risk Factor Surveillance System). To reduce the
incidence, prevalence, and burden of obesity and chronic disease, it is necessary for communities to
create environments that support healthier behaviors and make healthy choices, easier choices. This
involves engaging and mobilizing key stakeholders, decision makers, and community partners to work
within all levels of the health impact pyramid and across all sectors to promote “health in all policies.”

Broome County
Community Health Assessment 2019-2024 177
Focused efforts in this area include increasing healthy eating and food security, while collectively
working to eliminate racial/ethnic and socioeconomic health disparities.
Overview and Measures
Goal 1.0: Reduce the percentage of children who are obese in Broome County
Objective 1.1: By 2024, reach a childhood obesity rate of 12.9% among the target demographic, a
reduction from the baseline of 13.9%.
To accomplish this, the Broome County Health Department (BCHD) WIC Program will continue to
provide a decreased fat WIC food package, education once a year for children ages 2-4 about healthy
lifestyles including diet and exercise, and measure BMIs for children receiving nutrition counseling.
Progress towards this objective will be evaluated based on self-report measures gathered from WIC
participants regarding their knowledge and consumption of healthy foods and beverages, in addition to
their BMI data. Partner roles and resources include:
BCHD provides promotion of healthy lifestyle education and services of the WIC program.
UHS will oversee and administer UHS Stay Healthy Kids Program.
LOURDES will oversee the activities conducted by the PACT program.
Both UHS and Lourdes will ensure communication to providers about referrals to the Broome
County WIC program, for pregnant women, lactating women, post-partum women, infants and
children up to 5 years of age.
Objective 1.2: By 2024, decrease the percentage of school age children with obesity by 1 % from 17.7%
to the Prevention Agenda goal of 16.7%.
Several interventions will be used to reach this objective; they include: UHS - 1) UHS Stay Healthy Kids
Coordinator continues to work with Head Start schools to provide monthly classes on site, to children
age 3-5. Healthy eating and exercise tips are provided to children and their parents. The program is 18
classes per month. (2) The “Kids on Track” 8-week program continues in the Spring and Fall for children
5-13. This program covers exercise and nutrition appropriate to the age group. K-12 Schools - 1) School
Wellness Programs/Policies - establish and incorporate strong nutrition standards for food marketed,
provided and sold in schools, provide healthy eating learning opportunities through rock on cafe,
students using walking or biking to get to school, schools providing universal breakfast, grab and go
options, breakfast in the classroom, incorporating smarter lunch room strategies to increase access and
promote healthy eating, participating in Farm to School. The partners’ roles and resources include:
UHS - provides a Stay Healthy Kids Coordinator who educates headstart students, public school
age children/parents on healthy eating and beverage consumption choices,
Care Compass Network - innovation funding to UHS for Community based Nutrition Wellness
(education to take place at Cornell Cooperative Extension of Broome County).
BCHD will work with school districts to ensure wellness policies are following the required
standards set forth by the Healthy Hunger Free Kids Act, and provide technical assistance and
support to assist with any updates.
Objective 1.3: By 2024, decrease the percentage of adults ages 18 years and older with obesity, from
25.7% to 23.7%.
Several interventions will be used to reach this objective: BCHD - Work with community based
organizations, worksites and recreation venues to create policies related to sugary drink reductions,

Broome County
178 Community Health Assessment 2019-2024
healthy meeting guidelines and/or food procurement standards, LOURDES - Develop medical weight loss
program to support people aged 18 years and above with a BMI >30 in achieving a decrease in their BMI
and improvement in overall health, BCHD- Utilize NYSDOH, CDC, and locally developed messaging to
garner earned media on healthy eating, & promoting healthy beverages
Goal 1.1: Increase access to healthy and affordable foods and beverages
Objective 1.1.1: By 2024, decrease the percentage of adults from 31.9% to 27.9%, who consume less
than one fruit and less than one vegetable per day.
Several interventions will be used to reach this objective: Increase CHOW mobile markets in high risk
neighborhoods, Cornell Cooperative Extension to provide nutrition education, menu and budget
planning to SNAP recipients, OFA - Provide healthy meals & snack at Senior Centers and community
events, increase redemption of Office for Aging and WIC participants farmer's market coupons, open
grocery store on Northside of Binghamton (food desert) Volunteers Improving Neighborhood Program
(VINES) will increase access to and number of community gardens and Farm Share opportunities, in high
risk neighborhoods.
Goal 1.2: Increase skills and knowledge to support healthy food and beverage choice
Objective 1.2.1: By 2024 LOURDES (Adults) Increase the number of adults by 100 (from 200 to 300)
that improve their knowledge of and engagement in healthy eating habits by utilizing the Fruit and
Veggie RX Program.
To accomplish this LOURDES Dieticians in Lourdes Primary Care practices offer referred patients
information on healthy eating habits and "coupons" to purchase fruits and veggies. This is in
collaboration with Rural Health Network and Care Compass Network.
Objective 1.2.2: By 2024, Increase by 10%, from 22% to 32%, the percentage of WIC infants who
continue to be breastfed until 6 months.
To achieve this objective all WIC prenatal clients will be offered breastfeeding peer counseling and free
breastfeeding classes once a month, once baby is delivered peer counseling services will be provided
frequently and consistently to ensure increased duration.
Goal 1.3: Increase food security
Objective 1.3.1: Decrease percentage of population who did not have access to a reliable source of
food during the past year from 13.8% to 12.6%.
Interventions employed to achieve this objective include: 1) Promote and support screening of pediatric
patients by healthcare providers, facilitate referral and support active connection to WIC and/or SNAP;
2) Promote screening of older-adult populations for food insecurity, facilitate referral and support active
connection to SNAP 3) Continue to provide universal breakfast and lunch for k-12 in all schools 4)
Increase participation in summer lunch sites that serve families throughout Broome County.
Measures for these objectives include:
WIC Obesity -1) Number of WIC participants receiving a reduced fat food package, percentage of
children with obesity (among children ages 2-4 years participating in the Special Supplemental Nutrition
Program for Women, Infants, and Children [WIC]) 2) Number of WIC participants receiving general
nutrition education and active learning information and being assessed for height/weight every year.

Broome County
Community Health Assessment 2019-2024 179
School Age Obesity: 1) Number of students impacted by specific policies that address healthier nutrition
standards for food and beverages sold in schools (2) Number of school districts adopting specific policies
that address healthier nutrition standards for food and beverages sold in schools (3) Number of school
district wellness policies that address free drinking water, 4) Number of school districts participating in
Universal Breakfast 5) Number of students participating in Breakfast in the Classroom/Grab n' Go
Breakfast, 6)Number of school districts participating in Breakfast in the Classroom/Grab n' Go Breakfast
education classes 7) Percentage of children who are overweight [defined as having an age and gender
specific BMI at >85th to 95th percentile] 8) Percentage of children who are obese [defined as having an
age and gender specific BMI at >95th percentile] 9) Number of students using active transport methods
to/from school.
Adult Obesity: 1) Percentage of adults ages 18 years and older with obesity 2) Percentage of adults who
consume more than one or more sugary drink per day 3) Number of policies or food procurement
standards adopted in worksites, community based organizations, recreation venues and health care
institutions.
Increase access to healthy and affordable foods and beverages: 1) Percentage of adults who consume
less than one fruit and less than one vegetable per day, 2) Number of SNAP recipients educated on
nutrition, budget and meal planning, 3) Number of OFA Senior Sites providing healthy meals, 4) Number
of Seniors participating in OFA's Healthy Meals on Wheels, 5) Sales revenue from WIC, EBT, and SNAP
benefits for new grocery story on Northside Binghamton, 6) EBT, SNAP sales at Regional Farmer's
Market, 7) Number of CHOW mobile markets serving high risk neighborhoods
Increase skills and knowledge to support healthy food and beverage choices: Fruit and Veggie Rx
Program: 1) Number of adult patients participating in the fruit and veggie RX program 2) Number of
adult patients to redeem fruit and veggie Rxs 3) Number/percentage of adult patients who improve
knowledge of and engagement in healthy eating by using Rx program.
WIC Breastfeeding Program: 1) Percentage of WIC infants breastfed for 6 months 2) Number of WIC
prenatal clients linked with breastfeeding peer counselor, 3) Number of WIC prenatal clients attending
breastfeeding classes.
Increase Food Security: 1) Percentage of population who did not have access to reliable source of food
during the past year 2) Number of pediatric/primary care healthcare providers screening and providing
referrals to WIC/and or SNAP, 3) Percentage of households receiving SNAP, 4) Percentage of population
with low income and low access to grocery stores.
Focus Area #2: Preventive Care and Management
The CDC estimates that six out of ten Americans have at least one chronic disease, and four out of ten
have two or more. The productivity and quality of life for people living with a chronic disease such as
diabetes, heart disease, stroke and cancer is limited which in turn impacts their families as well. Most
chronic diseases are preventable and can be managed successfully with healthy behavior changes. In
Broome County, some populations suffer disproportionately from preventable chronic disease
conditions. Non-Hispanic and Black populations have significantly higher levels of mortality and
hospitalizations associated with heart/stroke and diabetes indicators. In addition, other health
determinants such as poverty and lower education status increase the need for chronic disease

Broome County
180 Community Health Assessment 2019-2024
management models, especially for many enrollees of Medicaid Managed Care plans who consistently
rely on hospital emergency rooms for emergent care of preventable health conditions. It is critical that
the Delivery System Reform Incentive Program (DSRIP) focuses on helping Medicaid members reduce
their risk and help manage chronic diseases and their risk factors. Chronic diseases need to be
appropriately diagnosed and managed in order to reduce the complications, burden of morbidity,
hospitalizations, poor function status and mortality that comes with chronic disease. Necessary
collaborations with healthcare systems and other community sectors need to ensure that successful
strategies exist for chronic disease management opportunities, especially where the most vulnerable
and high risk populations are concerned.
Overview and Measures
Goal: 4.1 Increase cancer screening rates
Objective 4.1: By 2024, increase the percentage of adults by 5% who receive a colorectal cancer
screening based on the most recent guidelines (ages 50 to 75 years) from 72% to 78%
Interventions include: Removal of structural barriers to cancer screening such as providing flexible clinic
hours, offering cancer screening in non-clinical settings (mobile mammography vans, flu clinics), offering
on-site translation, transportation, patient navigation and other administrative services and working
with employers to provide employees with paid leave or the option to use flex time for cancer
screenings, work with CSP to enhance marketing and communication efforts around colorectal cancer
screening in the priority population.
Goal 4.2: Increase early detection of cardiovascular disease, diabetes, prediabetes and obesity
Objective 4.1.2: By 2024, increase the percentage of children and adolescents ages 3 -17 years with an
outpatient visit with a primary care provider or OB/GYN practitioner during the measurement year
who received appropriate assessment for weight status during the measurement year by 5% (baseline
75%).
Intervention to achieve this objective is based on utilizing the US Preventive Service Guidelines and HIT,
to consistently implement screening practices/policies to identify children at risk for overweight or
overweight, and refer to behavioral and nutritional education programs.
Objective 4.2.2: By 2024, promote at least 3 strategies that improve the detection of undiagnosed
hypertension in health systems. The evidence based intervention that will be used to promote
strategies that improve the detection of undiagnosed hypertension in health systems is the CDC Million
Hearts Program.
Goal 4.3: Promote evidence-based care to prevent and manage chronic diseases including asthma,
arthritis, cardiovascular disease, diabetes and prediabetes and obesity
Objective 4.3.1: By 2024, decrease the percentage by 5% of adult Medicaid members, identified
through DSRIP with diabetes whose most recent HbA1c level indicated poor control (>9%).
Interventions employed for this objective include: UHS and Lourdes Primary care network offices to
work closely with the diabetes centers to implement standards of medical care in diabetes, work with
HIT to implement/modify EMR to include reminder system for screening, follow up and case
management activities.

Broome County
Community Health Assessment 2019-2024 181
Goal 4.4: In the community setting, improve self-management skills for individuals with chronic
diseases, including asthma, arthritis, cardiovascular disease, diabetes and prediabetes and obesity
Objective 4.4.1: By 2024, increase from 225 to 325 the number of adults with chronic conditions
(arthritis, asthma, CVD, diabetes, CKD, cancer) who have been identified and referred to take a course
or class to learn how to manage their condition.
Both hospital systems will provide standards of care to identify and assist with management of diabetes
by: 1. Promote testing for prediabetes, and risk for future diabetes in asymptomatic people in adults of
any age with obesity and overweight (BMI 25 kg/m2 or 23 kg/m2 in Asian Americans) and who have one
or more additional risk factors for diabetes, including first degree relative with diabetes, high risk
race/ethnicity, and history of cardiovascular disease. 2. Promote testing for all other patients beginning
at 45 years of age. 3. Promote repeat testing at a minimum of 3-year intervals, with consideration of
more frequent testing depending on initial results and risk status 4. Refer patients who are diagnosed
with obesity, CVD, or diabetes to community chronic disease self-management program (Stamford
Evidence Based Chronic Disease Self Management Program)
Measures for these objectives include:
Cancer screening: 1) Number of health systems that implement or improve provider and patient
reminder systems 2) Number of patients reached through patient reminder systems 3) Compliance with
screening guidelines among patients reached through patient reminder systems/among patients of
health systems that adopted systems 4) Provider, clinic or insurer breast and colorectal cancer screening
rates,
Early detection of chronic diseases- obesity: 1) Percentage of children who are overweight [defined as
having an age and gender specific BMI at ≥85th to 95th percentile 2) Percentage of children who are
obese [defined as having an age and gender specific BMI at ≥95th percentile] 3) Number & Percent of
children screened 4) Number of primary care providers conducting BMI screening 5) Number of hospital
systems implementing childhood BMI screening policy/system change.
Early detection of chronic diseases-hypertension: 1) Number of health systems with policies/practices
to identify patients with undiagnosed HTN 2) Number/percentage of patients served by health systems
with policies/practices in place 3) Number of patients identified with undiagnosed HTN.
Promote evidence-based care to prevent and manage chronic diseases- diabetes: 1) Screening rate for
diabetes and pre-diabetes among adults age 45+ 2) Number of patients identified as having diabetes or
pre-diabetes who receive follow-up by Stay Healthy Center 3)Number of patients receiving diabetes
education 4) Percentage of adults (age 45+) diagnosed with pre-diabetes or type 2 diabetes who are
referred to diabetes self-management training (DSMT) 5) Number of rural residents participating in
chronic disease self-management 6) Number of rural residents participating in chronic disease self-
management, 7) Percent of adult Medicaid members with diabetes identified through DSRIP with
controlled HbA1c
Chronic disease management in the community setting: 1) Number of health systems with
policies/practices to identify, refer patients with diabetes or prediabetes, obesity, CVD 2)
Number/percentage of patients served by health systems with policies/practices in place 3) Number of
patients identified with diabetes/prediabetes 4) Number of patients referred to community based
chronic disease self-management programs like Stamford Chronic Disease Self-Management Program or
National Diabetes Prevention Program.

Broome County
182 Community Health Assessment 2019-2024
Priority Area #2: Promote Mental Wellbeing and Prevent Mental &
Substance Use Disorders
Focus Area #!: Prevent Mental and Substance User Disorders
In the United States, age adjusted mortality rates related to prescription opioids have increased
contemporaneously with heroin drug poisoning over the past decade. A similar pattern is evident in NYS
with mortality rates increasing simultaneously with heroin drug overdose. The increase in opioid-related
deaths has not been evenly distributed across age groups nor concentrated primarily among youth. In
fact, middle-aged adults (25-34, 35-44, and 45-64 years of age) have experienced a disproportionate
share of this epidemic. Opioid-related emergency department visits and inpatient hospital admissions
have across the state. Counties within NYS with core urban areas are in the worst quintile. Broome
County has one of the highest opioid overdose death rate in NYS. The Steering Committee recognizes
the opioid epidemic as an emerging threat to the health and well-being of Broome County residents. A
task force, the Broome Opioid Abuse Council (BOAC), was formed in December of 2014 to formally
coordinate efforts directed toward addressing the opioid abuse crisis. The coalition is led by the Director
of the Broome County Health Department and comprised of multi-disciplinary team members who serve
on four subcommittees: community education, treatment and prevention, law enforcement, and
education of medical professionals. They are tasked with identifying critical priorities, developing a
unified plan, and implementation solution-oriented strategies that will have a substantive impact. BOAC
reports are available on the Broome County Health Department website. Issues associated with
substance disorders are closely connected to that of mental well-being, and adverse childhood
experiences. Broome County is seeing a substantial need for mental health and suicide prevention
interventions. Destigmatizing mental health and substance use disorders is critical in developing
community resilience. Building capacity for improved mental health diagnosis, treatment and recovery is
something that the Broome County community has clearly demanded attention of. The 2019-2024
Community Improvement Plan has dedicated the next section to improving our community’s mental
health and substance use disorders needs.
Overview and Measures
Goals: 2.2 Prevent opioid overdose deaths
Objective 2.2.1: By 2024, reduce the age-adjusted overdose deaths involving any opioid from 32.1% to
22.1% per 100,000 population.
Several interventions conducted by a vast array of community partners are underway to make an impact
on this objective: UHS: Medication Assisted Treatment ( MAT) in the Broome County Sheriff's
Correctional Facility. Counseling in the jail to engage inmates in treatment after their release, the
continuing of patients on MAT if they were on MAT at the time of their arrest, detoxification protocols
for inmates with OUD, same day access to MAT for inmates leaving the jail, MAT maintenance program,
Care Compass Network (DSRIP), LOURDES, Addiction Center Broome County, Fairview Treatment and
Recovery Center, Helio Health, Broome County Schools, Mental Health Association of the Southern Tier
and UHS: Adopting evidence based substance use screening tools for early identification, intervention,
and referral to resources and treatment (Alcohol Use Disorders Identification Test)-AUDIT, The Drug

Broome County
Community Health Assessment 2019-2024 183
Abuse Screening Test - DAST, Screening Brief Intervention to Treatment-SBIRT) Expansion of Inpatient
Recovery and Rehabilitation Services through Helio Health. Identification Test-AUDIT, The Drug Abuse
Screening Test - DAST, Screening Brief Intervention to Treatment-SBIRT), Expansion of Outpatient
Recovery and Rehabilitation Services through the Addiction Center of Broome County at second facility
in Endicott, Compass Network Innovation funding to Truth Pharm, Inc.: Administration and evaluation of
Clearing the Confusion education program- in process seeking accreditation from OASAS and SAMHSA.
UHS and Lourdes: Initiate Medication-Assisted Treatment in Binghamton General Hospital Emergency
and Lourdes Hospital Emergency Rooms.
Objective 2.2.2: By 2024, increase the number by 10 per year of providers attending Buprenorphine
trainings.
This objective will rely on the collaboration with Care Compass Network (DSRIP), UHS and LOURDES
Health Care Systems to promote trainings, recruit providers and conduct trainings.
Objective 2.2.4: By 2024, expand Peer Support Services by increasing engagement of priority
population from 50% to 80%.
To achieve this objective it will be necessary to recruit, train, and retain peers, coordinate peer response
efforts for hospital ERs, law enforcement agencies, and first responders, engage additional first
responders to develop and implement protocol for peer referrals to patients who want services,
enhancing and/or updating peer response model/language protocol.
Objective 2.2.4: By 2024, expand Peer Support Services by engagement of priority populations in
emergency departments from 0 to 10%.
This primary intervention engages and work with local hospitals to develop protocol for referrals to
peers in emergency departments.
Objective 2.2.5: By 2024, implement 2 prevention and response strategies by establishing 1) linkages
to care and 2) working with grassroots organizations and agencies to increase harm reduction
education projects.
The intervention needed to achieve this objective is to link community members with agencies who
provide narcan training and education.
Objective 2.2.6: By 2024, build capacity for a more effective, comprehensive and sustainable local
prevention and response effort by strengthening the infrastructure of the Broome Opioid Overdose
Awareness Council (BOAC)
Goal 2.3: Prevent and address adverse childhood experiences
Objective 2.3.1: By 2024, (developmental objective) Increase communities reached by opportunities
to build resilience by at least 10 %.
The primary intervention to help achieve this objective is Care Compass Network (DSRIP) conducting
ACE's and Youth Mental Health Fist Aid trainings in schools.
Goal 2.4: Reduce the prevalence of major depressive disorders
Objective 2.4.1: By 2024, (developmental objective) Increase communities reached by opportunities
to build resilience by at least 10 %.

Broome County
184 Community Health Assessment 2019-2024
The intervention associated with this objective is reliant on the Prevention Coalition conducting
Prevention Needs Assessment Survey in Broome County schools to determine risk and protective
factors, using data to develop evidence-based action plans.
Objective 2.4.2: By December 31, 2024, reduce by 5% the past year prevalence of major depressive
episode among adults aged 18 or older. Baseline TBD ICD 10 codes
In order to achieve this objective the following interventions will be employed: Execution of Care
Compass Network (DSRIP) projects related to integration of behavioral health (BH) in LOURDES and UHS
primary care sites ( 3ai, behavioral health/ substance use screens 4.a.ii. and crisis stabilization 3.a.ii.)
Adopting evidence based behavioral health screening for early identification, intervention and referral
to resources/treatment. Focusing on Medicaid and uninsured) ages 18-64 with a Patient Health
Questionnaire (PHQ) -9 score of 10 and above. Ensure sound referral process to a behavioral health
consultant for those screened at high risk. Recruit and train behavioral health consultants, social
workers who are trained in Eye Movement Desensitization and Reprocessing (EMDR) evidence based
recovery and the medical model. A uniformed approach to provider education and patient education.
The development of tools to engage patients. Addressing social determinants with an emphasis on
transportation.
Objective 2.4.3: By December 31, 2024, reduce by 5% the past-year prevalence of major depressive
episodes among adolescents aged 12-17 years. Baseline TBD ICD 10 codes
The interventions necessary to achieve this objective include: 1) Adapted integration model of BH in
UHS and LOURDES primary care clinics for use in pediatric and family care: Adopt evidence based
behavioral health screening for early identification, intervention and referral to resources/treatment
specifically for adolescents 2) Implementation of Recovery High School Model at Broome Tioga BOCES.
Goal 2.5: Prevent suicides
Objective 2.5.1: By 2024, reduce suicide attempts by Broome County adolescents (youth grades 9 to
12) who attempted suicide one or more times in the past year. Baseline TBD ICD 10 codes
In order to achieve this objective it is necessary to use the following interventions: Integrate use of Zero
Suicide evidence based intervention, Dialectic Behavioral Therapy, suicidal ideation workflows adoption
and safety planning in primary care and Cognitive Therapy Programs for at risk youth and families in
primary care settings
Objective 2.5.2: By 2024, reduce Age-adjusted suicide death rate per 100,000 population from 11.8%
to 8.0%
In order to achieve this objective it is necessary to use the following interventions: Address compassion
fatigue with specialized mental health trainings targeting mobile crisis team members, primary care
and behavioral health providers, ER staff, law enforcement, Broome County Suicide Awareness For
Everyone (BC SAFE) presence in the community at events to advocate for Suicide awareness and
education.
Measures for these objectives include:
Open Access Program: 1) Age-adjusted overdose deaths involving any opioid, 2) Number of opioid
overdose deaths, 3) Outpatient emergency department visits, hospitalizations. 4) Number unique clients
admitted to OASAS-certified chemical dependence treatment programs.

Broome County
Community Health Assessment 2019-2024 185
MAT in Broome County Correctional Facility: 1) Number of inmates receiving MAT 2) Number of
inmates receiving counseling 3) Number of inmates provided same day access to MAT maintenance
program upon release.
Adoption of substance use screening tools in primary care: 1) Number of healthcare, education, mental
health agencies adopting screening tools 2) Number of healthcare, education, mental health agencies
adopting practices, policies, protocol for evidence based screening tools.
Expansion of inpatient services in Helio Health: 1) Number of unique individuals receiving in patient
services through Helio Health.
Expansion of outpatient services in ACBC second location: 1) Number of unique individuals receiving
outpatient services from ACBC,
Truth Pharm Clear the Confusion Educational Series: 1) Pre/Post education test results measuring
knowledge, attitude changes 2) Number of educational sessions conducted 3) Number of attendees at
educational sessions,
Initiate Medication-Assisted Treatment in Binghamton General Hospital Emergency and Lourdes
Hospital Emergency Rooms: 1) Number of hospital system emergency departments providing MAT 2)
Number of emergency department providers trained to prescribe MAT 3) Reduce the age-adjusted
overdose deaths involving any opioid, 4) Number of opiod overdose deaths, 5) Outpatient emergency
department visits, hospitalizations 6) Number unique clients admitted to OASAS-certified chemical
dependence treatment programs.
Buprenorphine training for health care providers: 1) Number of providers attending training 2) Number
of providers prescribing MAT 3) Number of Primary Care Sites providing MAT
Expansion of Peers in identified areas of Broome County: 1) Number of peers recruited, trained and
retained 2) Number of hospital systems engaged to create protocol for peer referrals in emergency
departments 3) Number of first responders, including law enforcement agencies that develop and
implement protocol for making referrals to the peer response team.
Collaborating with Community Based Organizations to increase harm reduction messaging and narcan
training: 1) Number of agencies partnering to increase harm reduction education messaging and narcan
training.
Increasing Community Resilience: 1) Number of schools participating in First Aid for Youth Mental
Health Training. 2) Number of educational professionals trained in Youth Mental Health Training 3)
Number of health care providers trained in Youth Mental Health Trainings. 1) Number of Broome County
Schools conducting PNA. 2) Number of schools developing and implementing actions plans to address
risk and protective factors.
Integrating behavioral health into primary care, pediatric, family practice: 1) Percentage of adults with
poor mental health for 14 or more days in the past month, 2) Number of primary care clinic adopting BH
screening for early identification, intervention and referral to resources/treatment. 3) Number of
Medicaid and uninsured ages 18-64 with PHQ 9/10 score, referred to and established with treatment
resources within a two-week timeframe, 4) Number of providers/social workers/health consultants
trained in behavioral health, 1) Number of primary care clinics/pediatric/family care adopting BH
screening for early identification, intervention and referral to resources/treatment for adolescents 2)
Number of youth referred to and established with treatment resources within a two week timeframe, 3)
Number of providers and support staff trained in Youth Mental Health First Aid, 4) Number of

Broome County
186 Community Health Assessment 2019-2024
middle/high school youth referred and served in out of school time programs and or individualized
supports, 5) Number of youths who report improvement in emotional and mental health, 6) Increase
compliance with behavioral health appointments among youth.
Prevention of suicides with training in compassion fatigue for healthcare, law enforcement and other
front line professions that deal with crisis situations regularly: 1) Number of healthcare, behavioral
health, crisis management, law enforcement professionals trained in compassion fatigue and mental
health first aid, 2) suicide death rate per 100,000 population.
